Policy Forum
Nov 2016
Although recent changes in health care delivery have improved routine and gender-affirming care for transgender people, common approaches to care are still often based on a binary (i.e., male/female) gender framework that can make patients with gender-nonconforming (GNC) identities and expressions feel marginalized. Binary representation perpetuates invisibility, discrimination, and victimization—and subsequent poorer health—among GNC patients. In response, clinicians and health care systems should extend their efforts to provide gender-affirming and responsible care to GNC people. This article reviews terminology related to gender, the limited research—and necessary directions for future research—on GNC communities, and provides strategies for health care professionals and systems to ensure provision of gender-affirming and responsible care to GNC patients.
Recent years have seen rapid changes in health care delivery for patients identifying as transgender. These shifts include increasing clinicians’ ability to provide patient-centered, gender-affirming care for transgender people and structural and organizational improvements to ensure that provision of care occurs in an affirming environment [1-6]. For example, health care organizations are increasingly including “gender identity or expression” in patient nondiscrimination policies and mandatory cultural competence training inclusive of principles of gender-affirming care [1]. In addition, federal health insurance plans are now more likely to cover gender-affirming care [1, 2], and several health care associations have recently released statements on requirements for caring for transgender and gender-nonconforming people [3-5]. Although these advances are a significant step forward, they implicitly rely on binary definitions of sex and gender. Such thinking forces those who self-identify as gender nonconforming into a binary mold (e.g., if someone isn’t male, they must be “male-to-female”) and perpetuates medical systems’ lack of patient-centered and competent care for gender-nonconforming (GNC) people who do not identify with one of these binary labels. Given this reality, there remains a pressing need to better understand and optimize health care for GNC people.
What is gender nonconformity? Gender nonconformity can refer to a gender identity—one’s personal and subjective sense of gender—that is neither male nor female. It can also refer to a gender expression characterized by mannerisms and behaviors that are not conventionally associated with an assigned gender. People with nonconforming gender identities can identify with more than one gender (e.g., bigender), no gender (e.g., agender), or feel that their gender fluctuates or is undefinable by traditional terms (e.g., genderfluid). Nonconforming expressions can incorporate or exclude aspects of masculinity or femininity that differ from societal norms based on assigned gender (see figure 1). Gender nonconformity is independent of sexual orientation, and a particular sexual orientation cannot be inferred based on gender nonconformity. Notably, the taxonomy presented above is still grounded in Western and postcolonial attempts to categorize gender; even the concepts “bigender” or “third gender” reinforce gender binaries, othering (the tendency to marginalize) gender variance instead of accepting it in modern language and culture. In contrast, some South Asian countries recognize Hijra (people assigned male at birth who have a feminine gender expression) as a gender [7].
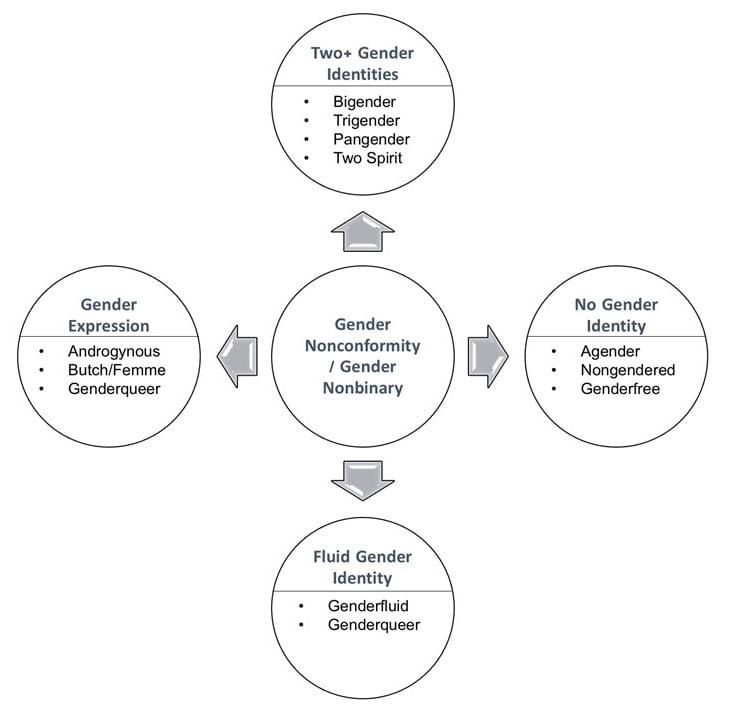
Figure 1. Common terminology for nonconforming gender identities and expressions.
Victimization of gender-nonconforming youth and adults. Research on gender nonconformity is scarce, with most studies using person- or observer-reported nonconforming behaviors (e.g., gender roles taken by children during imaginative play or appearance in adolescents and adults) to measure gender expression [8-14]. What is apparent from the available research, however, are the disproportionate levels of discrimination and victimization against GNC people, including those who also identify as transgender and/or lesbian, gay, bisexual, or queer (LGBQ). Children and adolescents with GNC expressions experience more bullying, victimization, and childhood abuse than their gender-conforming peers [12, 15, 16]. Harmful experiences persist into adulthood, with 19 percent of lesbian, gay, and bisexual adults in one study experiencing chronic daily discrimination based on gender nonconformity [11]. Furthermore, in a survey of transgender and gender-nonconforming adults, 31 percent of genderqueer adults reported experiences of police harassment, 20 percent worked in underground economy settings [17]—possibly due to a combination of job discrimination, poorer educational attainment secondary to bullying, and limited job opportunities—and 19 percent lost jobs due to “anti-transgender bias” [18]. In the same survey, 83 percent and 16 percent of genderqueer adults reported harassment and sexual assault, respectively, prior to age 18 [17]. With regard to health care, GNC adults often delay necessary care for fear of bias, present themselves as male or female when accessing care to avoid discrimination, and can self-medicate rather than engage with the health care system [17].
Gender-nonconforming people’s health care needs. GNC people’s high rates of victimization, coupled with limited social and cultural structural support, set the stage for health disparities. Childhood GNC is associated with poor adult mental health [14]. In particular, youth and adults who were GNC children have greater risk of lifetime depressive symptoms and higher prevalence of posttraumatic stress disorder (PTSD) than their gender-conforming peers [8, 9, 12, 13]. Consistent with minority stress theory, which links minority affiliation to poorer health through stress and discrimination [19], victimization mediates the development of depression and PTSD among GNC people [13, 20]. Although higher proportions of youth who were GNC children have nonheterosexual sexual orientations compared with gender-conforming youth, the majority identify as heterosexual [12], and mental health conditions described above remain associated with gender nonconformity independently of sexual orientation [12, 21]. This finding suggests that the discrimination and victimization of people who are gender nonconforming can lead to poorer mental health outcomes, irrespective of sexual orientation. It is also worth noting that, among GNC adolescents, natal males have a lower average body mass index (BMI) and natal females have a higher average BMI compared with gender-conforming adolescents after controlling for sexual orientation [10]. Although the clinical significance of these findings requires further evaluation because reported average BMIs were within the healthy range, childhood harassment for gender nonconformity is associated with body shame [22] and lower levels of physical activity [10, 23].
The above research highlights early and persistent health challenges experienced by GNC people. However, striking gaps remain in our knowledge of GNC people’s utilization of health care services and physical health outcomes, longitudinal models of GNC people’s health and the impact of gender-affirming services on their health, protective and supportive factors, and how each of these interacts with additional aspects of identity (e.g., race, culture, sex). Also lacking is an understanding of which gender-affirming services—social, psychological, medical, or legal—are desired by GNC people. Many people may prefer a nonconforming expression achieved through means other than medical support (e.g., clothing, hairstyle), but how should health care professionals respond when less reversible gender-affirming treatments (e.g., cross-gender hormones, surgeries) are requested? For example, how might a professional care for Morgan, a genderqueer, female-assigned person if the patient wants to masculinize their appearance through testosterone or chest reduction surgery? How might the clinician’s feelings towards treatment change if one of Morgan’s previous caregivers already initiated testosterone therapy? Or if Morgan is sixteen instead of thirty-six? Many clinicians already struggle to provide care to people who want to transition genders on a binary spectrum despite the availability of evidence-based guidelines [24, 25]. However, in view of demonstrable health benefits of gender-affirming health care interactions and accessible transition options among transgender populations [26-28], we posit that GNC people are likely to derive similar benefits. Therefore, we and others [6] urge clinicians to extend similarly tailored care to this group.
Understanding gender-affirming health care practices. Clinicians should understand how to validate and support GNC patients by providing gender-affirming care. Although resources for doing so previously were limited—including the omission of GNC people from commonly used gender transition guidelines, such as the World Professional Association on Transgender Health (WPATH) Standards of Care prior to its most recent version [24]—evidence-based guidelines and widely used clinician sources of medical information now address gender-affirming care for GNC people [24, 25, 29, 30]. More recently, several national regulatory and health professions education organizations have recommended strategies to promote equitable care for people who identify as GNC [31, 32], which can be categorized by recognized medical competencies (see table 1).
| Knowledge for Practice |
|
Define and understand the differences between gender identity and gender expression, including the nonbinary diversity within each. Discuss options for social, medical, and surgical gender affirmation and the roles of different health professionals in each type. |
| Patient Care |
|
Respect and affirm identities using a patient-centered approach. Discuss gender histories and developments with patients across the lifespan. Tailor the medical history and physical exam based on patient experiences and needs, including gender identity and expression. Screen patients for childhood and current trauma, depression, anxiety, substance use, body image, and disordered eating. Discuss protective factors and sources of resilience. |
| Systems-Based Practice |
|
Provide a medical home for GNC patients, including ensuring a welcoming and affirming climate and training all staff members. Work as part of an interprofessional team in order to provide patient-centered care. Be knowledgeable about, and include social support and community resources in, care plans. Include GNC people in community- and patient-engaged care delivery. |
| Practice-Based Learning and Improvement |
|
Be aware of your own biases toward GNC identities and expressions and implement strategies to mitigate biases. Discuss and use existing guidelines for transitioning with patients and develop openness to nonbinary medical transitions. |
| Interpersonal and Communication Skills |
|
Work with patients to ensure minimization of stigmatizing forces within health care systems (i.e., by knowing how to document gender nonconformity in electronic health records and ensuring safety in waiting rooms and other public areas). |
| Professionalism |
|
Assume shared responsibility for reducing stigma and health disparities experienced by GNC people across their lifespans. |
A foundational concept is to understand and value the diversity embedded within the term “gender” and the panoply of ways people may choose to describe and express their gender. With this core understanding of gender in mind, clinicians can focus on optimizing interactions with individual patients. For example, GNC people might use gender-neutral pronouns (e.g., they/them/theirs); clinicians’ nonjudgmental use of this language assists with establishing rapport and cultivating respectful relationships. Discussing with patients their gender histories and evolution can aid clinicians’ understanding of how they can personally express respect for and affirm patients’ gender. Clinicians should elicit their patients’ experiences of trauma and stress and screen for associated conditions including depression, anxiety, substance use, body image, and disordered eating. Conversations with patients should address how the patient’s gender identity influences these conditions and how gender-affirming care may be part of a comprehensive care plan to improve health. Moreover, in discussing these matters, clinicians should see their patients as individuals who have coped with hardship and identify sources of patients’ resilience. These conversations, particularly concerning histories of trauma and patients’ personal relationship with their body, inform how physical exams can be tailored to minimize stress (e.g., use their preferred language for gendered body parts, position patients for procedures in ways least likely to trigger traumatic memories) [33]. For example, during a Pap test, patients may prefer a position without footrests or insert a speculum themselves to retain autonomy. Importantly, clinicians can try more mindfully to notice that they have biases or make judgments that impede the formation of strong patient-clinician relationships. Becoming aware of such biases and developing strategies to mitigate reactions so that they do not adversely influence a patient’s care are critical components of gender-affirming and responsible care.
Personalized care. It is incumbent upon health professionals to continue striving to meet the needs of individual patients, even when evidence of the effectiveness of interventions is lacking. A key focus for future research should be the health impact of gender-affirming care for GNC people. Although evidence supports the benefits of gender-affirming transitions for transgender adults [26-28], no studies have yet evaluated the impact of—or how to tailor—medical or surgical gender-affirming care among GNC people. However, because many GNC people seeking gender-affirming care present as male or female and anecdotal evidence suggests that gender-affirming models can promote better care for these individuals, it’s reasonable to expect that the health benefits of these models might be similar to those demonstrated for transgender people. In the absence of evidence, the core principles underlying the WPATH Standards of Care should be applied when initiating medical and/or surgical care for GNC people (see table 2).
|
“Exhibit respect for patients with nonconforming gender identities (do not pathologize differences in gender identity or expression)” [34]. “Provide care (or refer to knowledgeable colleagues) that affirms patients’ gender identities and reduces the distress of gender dysphoria, when present” [34]. “Become knowledgeable about the health care needs of transsexual, transgender, and gender nonconforming people, including the benefits and risks of treatment options for gender dysphoria” [34]. “Match the treatment approach to the specific needs of patients, particularly their goals for gender expression and need for relief from gender dysphoria” [34]. “Facilitate access to appropriate care” [34]. “Seek patients’ informed consent before providing treatment; offer continuity of care” [34]. “Be prepared to support and advocate for patients within their families and communities (schools, workplaces, and other settings)” [34]. |
Each patient’s unique treatment goals must be ascertained when initiating medical therapy for GNC patients. For example, recall that Morgan, who was birth assigned female and self-identifies as genderqueer might not wish to have a penis or be a man. But such a patient might wish to achieve cessation of menses and consider mastectomy in order to avoid ongoing chest binding, which can be confining and uncomfortable. Eliciting these goals of care from the patient and, in the process, discussing specific body regions that cause distress without focusing on binary gender transitions should determine the specific recommendations that a clinician can make (which, in the case of the above genderqueer patient, could include achieving menstrual control via continuous combined oral contraceptives, depot medroxyprogesterone acetate injection, or placement of a progestin-eluting IUD as well as referral to a surgeon to discuss the option of mastectomy). Participation in shared decision making requires the clinician to review all the available treatment options—including specific risks, benefits, and desired and undesired side effects—and address patient concerns associated with each modality.
Overcoming systems-level challenges. GNC people should have access to a gender-affirming medical home where all components of care can be discussed nonjudgmentally in an environment that minimizes stigma and discrimination. Yet delivery of quality care to GNC patients may be challenged by systemic barriers both inside and outside health care facilities. Many state laws do not include gender identity in nondiscrimination policies [35, 36]. Similar to patients who are underinsured or uninsured, GNC patients who lack insurance coverage for gender-affirming care may be prohibited from obtaining necessary care. Strategies for enhancing the institutional climate have been extensively discussed [1, 28, 29]. Clinicians can take the lead in implementing many of these strategies, including ensuring that all front-desk and clinical staff participate in creating a welcoming and affirming environment, coordinating optimal care through interprofessional teams, referring patients to social and community services as part of personalized care plans, and involving GNC patients in systems-level decisions impacting their care by including them on community advisory boards.
People with GNC identities and expressions face significant discrimination and victimization that contribute to the development of poorer mental, physical, and behavioral health. Although GNC expression and maltreatment are apparent at a young age, the latter can be mitigated by family, peers, and others with the capacity to protect and promote well-being, including health care professionals. By adopting a patient-centered approach to care, utilizing available resources to affirm patients’ genders, advancing research to better address the health and health care of GNC people, advocating for patients within and outside the health care system, increasing access to gender-affirming services, and engaging GNC patients on health care advisory boards, clinicians can continue working to ensure delivery of gender-affirming and responsible care to GNC patients.
Human Rights Campaign Foundation. Healthcare Equality Index 2016: Promoting Equitable and Inclusive Care for Lesbian, Gay, Bisexual and Transgender Patients and Their Families. Washington, DC: Human Rights Campaign Foundation; 2016:36. http://hrc-assets.s3-website-us-east-1.amazonaws.com//files/assets/resources/HEI_2016_FINAL.pdf.Accessed July 26, 2016.
US Department of Health and Human Services. Section 1557 of the Patient Protection and Affordable Care Act. http://www.hhs.gov/civil-rights/for-individuals/section-1557/. Accessed September 1, 2016.
American Geriatrics Society Ethics Committee. American Geriatrics Society care of lesbian, gay, bisexual, and transgender older adults position statement. J Am Geriatr Soc. 2015;63(3):423.
Daniel H, Butkus R; Health and Public Policy Committee of the American College of Physicians. Lesbian, gay, bisexual, and transgender health disparities: executive summary of a policy position paper from the American College of Physicians. Ann Intern Med.2015;163(2):135-137.
American Academy of Pediatrics. American Academy of Pediatrics opposes legislation that discriminates against transgender children [news release]. Raleigh, NC: April 18, 2016. https://www.aap.org/en-us/about-the-aap/aap-press-room/Pages/AAPOpposesLegislationAgainstTransgenderChildren.aspx?nfstatus=401&nftoken=00000000-0000-0000-0000-000000000000&nfstatusdescription=ERROR:+No+local+token.Accessed September 1, 2016.
Reddy G. With Respect to Sex: Negotiating Hijra Identity in South India. New Delhi, India: Yoda Press; 2006.
Bos H, de Haas S, Kuyper L. Lesbian, gay, and bisexual adults: childhood gender nonconformity, childhood trauma, and sexual victimization [published online ahead of print April 1, 2016]. J Interpers Violence. doi: 10.1177/0886260516641285.
Van Beusekom G, Bos HM, Kuyper L, Overbeek G, Sandfort TG. Gender nonconformity and mental health among lesbian, gay, and bisexual adults: homophobic stigmatization and internalized homophobia as mediators [published online ahead of print April 25, 2016]. J Health Psychol. doi: 10.1177/1359105316643378.
Harrison J, Grant J, Herman JL. A gender not listed here: genderqueers, gender rebels, and otherwise in the National Transgender Discrimination Survey. Harv Kennedy Sch LGBTQ Policy J. 2012;2:13-24.
Harrison J, Grant J, Herman JL, 22.
Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, et al; Endocrine Society. Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab.2009;94(9):3132-3154.
Feldman J, Deutsch MB. Primary care of transgender individuals. UpToDate®. http://www.uptodate.com/contents/primary-care-of-transgender-individuals. Accessed July 20, 2016.
Olson-Kennedy J, Forcier M. Overview of the management of gender nonconformity in children and adolescents. UpToDate®. http://www.uptodate.com/contents/overview-of-the-management-of-gender-nonconformity-in-children-and-adolescents. Accessed July 20, 2016.
Joint Commission. Advancing Effective Communication, Cultural Competence, and Patient- and Family-Centered Care for the Lesbian, Gay, Bisexual, and Transgender (LGBT) Community: A Field Guide.Oakbrook Terrace, IL: Joint Commission; 2011. http://www.jointcommission.org/assets/1/18/LGBTFieldGuide.pdf.Accessed July 26, 2016.
Association of American Medical Colleges. Implementing Curricular and Institutional Climate Changes to Improve Health Care for Individuals Who Are LGBT, Gender Nonconforming, or Born with DSD: A Resource for Medical Educators. Washington, DC: Association of American Medical Colleges; 2014. https://www.aamc.org/download/414172/data/lgbt.pdf?utm_referrer=http%3A%2F%2Foffers.aamc.org%2Flgbt-dsd-health.Accessed July 26, 2016.
Coleman, Bockting, Botzer, et al, 167.
Human Rights Campaign. Maps of state laws & policies. http://www.hrc.org/state_maps. Accessed September 1, 2016.
American Civil Liberties Union. Non-discrimination laws: state by state information—map. https://www.aclu.org/map/non-discrimination-laws-state-state-information-map. Accessed September 1, 2016.



