Policy Forum
Jan 2017
Evidence-based practice standards are not yet well defined for assisting potential victims of human trafficking. Nonetheless, health care professionals are learning to be first responders in identifying, treating, and referring potential victims. As more public and private sector resources are used to train health care professionals about human trafficking, more evaluation and research are needed to develop an effective standard of care. Adopting a public health lens and using the “National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care” can guide critical decision making and actions. Through collaboration between researchers and policymakers, lessons learned in health care settings can inform future evidence-based standards of care so that all patients receive the services that they need.
Human trafficking, a form of modern-day slavery, is a crime. The initial federal law, the Trafficking Victims Protection Act (TVPA) of 2000, has been reauthorized three times to increase society’s power to address victims’ needs and to put an end to this injustice. Under the law, a trafficking victim is a person induced to perform labor or a commercial sex act through force, fraud, or coercion. Any person under age 18 who performs a commercial sex act is considered a victim of human trafficking, regardless of whether force, fraud, or coercion was present [1].
Health care professionals who encounter a potential victim of human trafficking in a health care setting should be guided by ethical principles, while simultaneously recognizing that other perspectives and standards are needed to guide their actions and decision making. According to Beauchamp and Childress, the fundamental principles governing physician-patient relationships are beneficence (the obligation to prevent harm and promote good), nonmaleficence (the obligation to do no harm), justice (the obligation to provide others with whatever they are owed or deserve), and autonomy (the obligation to respect the self-determination of other persons) [2]. These principles are important directives for health care professionals faced with a potential victim of human trafficking in a health care setting, and they guide and form the foundation for any effective response. Better service delivery begins with training about human trafficking, adoption of a public health lens, and understanding of social determinants of health. As training programs and the public health lens become more widely adopted, building practice-policy feedback loops will help ensure that evidence-based standards of care are developed and applied effectively to all populations at risk for human trafficking.
To better understand human trafficking, the US Department of Health and Human Services (HHS) in 2008 sponsored a National Symposium on the Health Needs of Human Trafficking Victims. This symposium served as a follow-up to its exploratory study on HHS programming for victims [3]. During the symposium, more than 150 health care professionals discussed human trafficking, their role in addressing the needs of victims, and ways to improve the health care system’s response to victims. Participants stated that training professionals in the medical field is imperative to improve identification of, and service delivery to, victims [4]. HHS, through its National Human Trafficking Resource Center and with input from both for-profit and not-for-profit organizations, developed and implemented valuable online and in-person training for health care professionals on identifying and responding to trafficking victims [5]. The provision of training for first responders, e.g., physicians, dentists, nurses, is in alignment with the five-year Federal Strategic Action Plan on Services for Victims of Human Trafficking in the United States, 2013-2017 [6]. HHS also created the “Stop. Observe. Ask. Respond to Human Trafficking (SOAR) to Health and Wellness Training” to educate health care professionals and other community leaders about human trafficking and victim identification [7].
Early victim identification is an important aspect of training because research has shown that many victims interface with the health care system but few are helped [8]. One study showed that 88 percent of victims had contact with at least one health care professional at some point during the period in which they were being trafficked; however, none were identified or offered assistance to get out of bondage during the encounter [9]. Another study of emergency department personnel found that 29 percent thought human trafficking was a problem in their emergency department population; however, only 13 percent of the study participants felt confident or very confident that they could identify a victim of human trafficking, and fewer than 3 percent had ever been trained to recognize victims [10].
When it comes to identification of human trafficking victims, several barriers exist for both health care professionals and patients. Professional-related barriers include clinicians’ lack of knowledge regarding human trafficking, failure to apply trauma-informed care, and cultural assumptions about the victim [11-13]. Patient-related barriers include patients’ failure to self-identify as human trafficking victims due to fear, shame, and lack of awareness of victim status and rights; lack of knowledge of US laws and contractual obligations in cases of labor trafficking; and language barriers and illiteracy. Health care facilities that develop protocols that take into account all these factors will be poised to deliver appropriate health care for victims of human trafficking.
According to Jonathan Todres, “Public health methodologies can move us from confronting harm only after millions of people have suffered to strengthening individuals’ and communities’ capacities to prevent human trafficking” [14]. The public health lens is a powerful tool in the effort to end human trafficking because it focuses on prevention, ending violence, and understanding the social determinants of health [15, 16]. Population health looks at “the health outcomes of a group of individuals, including the distribution of such outcomes within the group” and links these to social determinants on the one hand and policies and interventions on the other [17]. Health care professionals who adopt a public health lens view human trafficking as part of a spectrum of interrelated violence and systemic inequities that are influenced by the social determinants of health.
Understanding the social determinants of health and highly vulnerable populations. Social determinants of health are the circumstances in which people are born, grow up, live, and work that affect health. Families and communities vary in their past experience with and vulnerability to harm. Anyone can become a victim of human trafficking. However, social determinants of health make some groups particularly vulnerable to trafficking. These populations include: people with a history of childhood abuse and neglect; children who have been in foster care or who have spent time within the juvenile justice system; runaway and homeless youth; people with disabilities; undocumented immigrants; people with low incomes; lesbian, gay, bisexual, transgender, and questioning people; migrant workers; and racial and ethnic minorities [18]. With regard to racial and ethnic demographics and human trafficking, very little discourse has occurred and even less research exists. Figure 1 shows that of confirmed sex trafficking victims whose race was known, 40.4 percent were black, 25.6 percent were white, 23.9 percent were Hispanic, 4.3 percent were Asian, and 5.8 percent were other [19]. Likewise, figure 2 shows that of confirmed labor trafficking victims whose race was known, 55.7 percent were Hispanic, 18 percent were other, 14.8 percent were Asian, 9.8 percent were black, and 1.6 percent were white [19]. The high rates of human trafficking within communities of color present an excellent opportunity for professionals, researchers, and policymakers who are knowledgeable about minority health disparities to contribute their expertise to human trafficking prevention and intervention strategies.

Figure 1. Sex trafficking victims by race. Reprinted from “2013 National Crime Victims’ Rights Week Resource Guide,” © 2013 US Department of Justice Office of Justice Programs Office for Victims of Crime and National Center for Victims of Crime [19].
Note: Data from 2011 US Department of Justice special report [20].
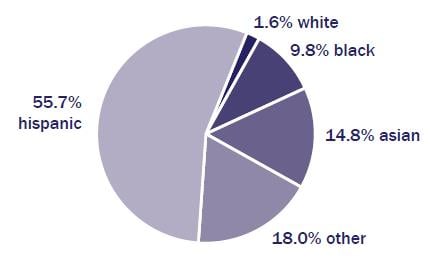
Figure 2. Labor trafficking victims by race. Reprinted from “2013 National Crime Victims’ Rights Week Resource Guide,” © 2013 US Department of Justice Office of Justice Programs Office for Victims of Crime and National Center for Victims of Crime [19].
Note: Data from 2011 US Department of Justice special report [20].
Prevention and intervention strategies. Anti-trafficking and local, state, and national minority health experts can braid together their knowledge about vulnerable populations and their approaches to best serve these populations. One tool developed by the US Department of Health and Human Services Office of Minority Health is the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care (The CLAS standards) [21]. The CLAS standards aim to ensure effective, equitable, and respectful care and services that are responsive to diverse needs. They encourage effective communication between the health care professional, health care facility, and the surrounding community. The 15 standards address inequities at every point of patient contact with the health care system and encompass three broad themes: (1) governance, leadership, and workforce; (2) communication and language assistance; and (3) engagement, continuous improvement, and accountability. Examples of CLAS standards include (1) conducting regular assessments of community health assets and needs and using the results to plan and implement services that respond to the cultural and linguistic diversity of populations in the service area; and (2) partnering with the community to design, implement, and evaluate policies, practices, and services to ensure their cultural and linguistic appropriateness. By using the CLAS standards, health care professionals and the health care system can better care for victims of trafficking by engaging appropriate community partners and developing culturally competent interventions. In applying cultural competency tools such as the CLAS standards in health care facilities, health care professionals can understand the many stressors faced by these vulnerable populations.
Beneficence and nonmaleficence call for the use of a trauma-informed approach that is sensitive to the patient’s past experiences with the health care system and society. A trauma-informed approach to care maximizes healing and recovery while minimizing the risk of retraumatization [11]. Both the CLAS standards and a trauma-informed approach are examples of evidence-based standards; both are directly related to the experiences and risk factors of those who have been trafficked. Health professionals can build upon these standards and use them to address the needs of victims of human trafficking. Evidence-based practice standards such as the CLAS standards and a trauma-informed approach that can be applied effectively to all populations will be shaped by practice-policy feedback loops.
Relative to other problems such as intimate partner violence, anti-trafficking practice-policy feedback loops, in which health care professionals and researchers inform the work of policymakers, are in their infancy. While some researchers have developed and tested appropriate screening tools, little research exists on the evaluation and development of evidence-based practices for identifying and treating victims of trafficking [22, 23]. Progress has been made, however, in developing and disseminating recommended practices and protocols in institutions [24]. Health care professionals can also seek guidance from trauma-informed care resources such as the Substance Abuse and Mental Health Services Administration’s National Center for Trauma-Informed Care and through learning networks [11]. A large and well-organized learning group is the Health, Education, Advocacy, Linkage (HEAL) Network, which provides a platform for interdisciplinary health professionals to discuss recommended care for treating victims of human trafficking. Members can join working committees focused on topics such as education and training, prevention, and protocol development [25]. The goal is that health care professionals trained in identifying trafficking victims will build up an evidence base of care needs and treatment outcomes that will inform standards of care, which can be further refined as they are used in practice. The accumulation of knowledge through practice-policy feedback loops will move the anti-trafficking field forward over time.
The US health care system relies on the belief that health care professionals follow codes of ethics and a body of knowledge grounded in evidence-based research and training. Although quantitative evidence-based research accumulates over time, health care professionals can contribute to the body of knowledge of trauma-informed and culturally competent care by sharing and testing potential promising practices. As in other fields, these changes will not wait for comprehensive evidence-based research. The process of learning is much more fluid. Lessons learned in health care settings can inform future evidence-based standards of care so that all patients receive the services that they need. With training, a public health focus, and practice-policy feedback loops, health care professionals will be able to see, understand, and respond appropriately to victims of human trafficking in their waiting rooms.
Victims of Trafficking and Violence Protection Act, 22 USC sec 7101-7113 (2000). http://www.state.gov/j/tip/laws/61124.htm. Accessed September 19, 2016.
Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 2nd ed. New York, NY: Oxford University Press; 1983.
Clawson H, Dutch N. Addressing the needs of victims of human trafficking: challenges, barriers, and promising practices. US Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/basic-report/addressing-needs-victims-human-trafficking-challenges-barriers-and-promising-practices. Published July 20, 2008. Accessed November 23, 2016.
Williamson E, Dutch NM, Clawson HJ. National symposium on the health needs of human trafficking victims: post-symposium brief. US Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/sites/default/files/pdf/75841/ib.pdf. Published July 15, 2009. Accessed November 23, 2016.
National Human Trafficking Resource Center. Online trainings. https://traffickingresourcecenter.org/material-type/online-trainings. Accessed September 19, 2016.
US Department of Justice Office for Victims of Crime. Coordination, Collaboration, Capacity: Federal Strategic Action Plan on Services for Victims of Human Trafficking in the United States 2013-2017. http://www.ovc.gov/pubs/FederalHumanTraffickingStrategicPlan.pdf. Published January 2014. Accessed September 19, 2016.
US Department of Health and Human Services Office of Trafficking in Persons. SOAR to Health and Wellness Training. http://www.acf.hhs.gov/endtrafficking/initiatives/soar. Updated September 8, 2016. Accessed September 19, 2016.
Chisolm-Straker M, Richardson L. Assessment of emergency department (ED) provider knowledge about human trafficking victims in the ED. Acad Emerg Med. 2007;14(suppl 5):S134-S134.
Substance Abuse and Mental Health Services Administration. SAMHSA’s concept of trauma and guidance for a trauma-informed approach. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014. HHS publication (SMA) 14-4884. http://store.samhsa.gov/shin/content/SMA14-4884/SMA14-4884.pdf. September 19, 2016.
Todres J. Moving upstream: the merits of a public health law approach to human trafficking. North Carol Law Rev. 2011;89(2):506.
Powell CL. Human trafficking. In: Markle W, Fisher MA, Smego RA, eds. Understanding Global Health. 2nd ed. New York, NY: McGraw Hill; 2013:117-140.
Chon K. The power of framing human trafficking as a public health issue. US Department of Health and Human Services Office of Trafficking in Persons. http://www.acf.hhs.gov/endtrafficking/resource/publichealthlens. Published January 11, 2016. Accessed September 15, 2016.
Kindig D, Stoddart G. What is population health? Am J Public Health. 2003;93(3):381.
Clawson H, Dutch N, Solomon A, Goldblatt Grace L. Human trafficking into and within the United States: a review of the literature. US Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/basic-report/human-trafficking-and-within-united-states-review-literature. Published August 30, 2009. Accessed November 23, 2016.
US Department of Justice Office of Justice Programs Office for Victims of Crime; National Center for Victims of Crime. 2013 National Crime Victims’ Rights Week resource guide. https://www.ncjrs.gov/ovc_archives/ncvrw/2013/pdf/2013ResourceGuide-Full.pdf. Published 2013:24. Accessed September 19, 2016.
Banks D, Kyckelhahn T. Special report: characteristics of suspected human trafficking incidents, 2008-2010. Washington, DC: US Department of Justice Bureau of Justice Statistics; 2011:1. http://www.bjs.gov/content/pub/pdf/cshti0810.pdf. Accessed November 8, 2016.
US Department of Health and Human Services Office of Minority Health. The National CLAS standards. http://minorityhealth.hhs.gov/omh/browse.aspx?lvl=2&lvlid=53. Updated September 1, 2016. Accessed September 19, 2016.
Cannon AC, Arcara J, Graham LM, Macy RJ. Trafficking and health: a systematic review of research methods [published online ahead of print May 17, 2016]. Trauma Violence Abuse. doi:10.1177/1524838016650187.
Alpert EJ, Ahn R, Albright E, Purcell G, Burke TF, Macias-Konstantopoulos W. Human trafficking: guidebook on identification, assessment, and response in the health care setting. Massachusetts General Hospital; Massachusetts Medical Society; 2014. Accessed September 19, 2016.
HEAL network website. https://healtrafficking.org/. Accessed September 19, 2016.



