Medical Education
Feb 2018

Graphic medicine is a swiftly growing movement that explores, theoretically and practically, the use of comics in medical education and patient care. At the heart of graphic medicine are graphic pathographies, stories of illness conveyed in comic form. These stories are helpful tools for health care professionals who seek new insight into the personal, lived experience of illness and for patients who want to learn more about their disease from others who have actually experienced it. Featuring excerpts from five graphic pathographies, this essay illustrates how the medium can be used to educate patients and enhance empathy in health care professionals, particularly with regard to informed consent and end-of-life issues.
Over the past eight years, graphic pathographies have become powerful tools in medical education and patient care [1, 2]. From these stories, practitioners and trainees can discover details they might not have known or fully understood about how an illness can impact a person’s daily living. Similarly, patients can learn new information from others who contend with the same illness. These new perspectives can help lessen the isolation that patients often feel and can also help patients cultivate practical skills that might enhance their autonomy and moral agency. This essay provides a brief overview of the advantages of the comic medium as well as a practical method for teaching graphic pathographies, with special attention to empathy, informed consent, and end-of-life decision making.
Two key goals of medical practice are competence and compassion. In order to be competent, one must understand illness in all its complexity—that is, both its pathophysiology and its impact on the patient on a social and emotional level. Physicians must come to know and comprehend a patient’s story, perhaps especially how the patient experiences illness when she is not in the doctor’s office. An awareness of this lived experience of illness helps physicians help their patients to manage disease and its sequelae. Information learned through stories is more likely to be retained [3]; this is perhaps a chief reason that medical education features case-based learning. When we both hear and see stories unfold, perhaps we remember things even more vividly—hence the presence of real patients who tell their stories to medical students [3] and the ability of seasoned medical practitioners to remember “one patient, Mr. Z, twenty years ago,” who presented with unusual symptoms. Graphic pathographies are thus an excellent means to retain information and hone the interpretive abilities necessary to treat the whole patient.
As a medium, comics have several benefits for trainees and patients [1, 2]. From the outset, comics can seem inviting because of their association with pleasure reading and lightheartedness. Moreover, the medium seems inherently accessible: there’s little expectation that one must interpret a comic in a certain way. As cartoonist Chris Ware says, “You don’t blame yourself for not ‘getting’ a comic strip—you usually blame the cartoonist” [4]. This psychological advantage can be particularly important to medical students who are inundated with heavy reading and continually under pressure to get things right on exams and in their new duties on the wards. For a patient or family member who wants to learn about a disease, comics can be disarming—an inviting, nonthreatening way to familiarize oneself with a condition that is perhaps itself inherently threatening.
The comics form also has several advantages over words or images alone. Because words and images complement each other in comics, neither has to do the work of meaning-making alone. This provides yet another psychological advantage for medical trainees and professionals who continually operate under severe time constraints. Dense text, comprising many words and complex sentence structures, can seem overwhelming when one wants to understand ideas both clearly and quickly. The same can be true of flow charts and figures whose details are so granular that they prompt a busy professional to crave a straightforward verbal summary of high-yield information. By contrast, the relative succinctness of comics text, which “can communicate in a panel that is 2 inches by 2 inches in size something that might take 3 pages in some circumstances to describe by writing” [5], seems user-friendly, and the icon, or “any image used to represent a person, place, thing, or idea,” can resonate with readers because of its universality [6]. Consider, for instance, how a smiley face can prompt similar understanding—and perhaps feeling—in people of different backgrounds, ethnicities, and sexes. The smiley face is not specific to any one group of people; rather, it is readily identifiable as universally human. In short, according to Michael Green, the comic medium’s “visual aspect helps [medical] students become more careful observers, discerning hidden messages and nonverbal cues when interacting with patients” [5]. Perhaps most important, as readers encounter the verbal and visual together, both the left and right hemispheres of the brain are engaged, which can enhance both cognitive and affective learning [7].
Visual thinking strategies (VTS) is a helpful approach to teaching graphic pathographies. The beauty of VTS is its seeming simplicity that can nevertheless lead to rich discovery, discussion, and insight [8]. VTS poses three basic questions:
The process allows one to begin with intuition, a “gut feeling” about what’s happening. The second question shifts attention to careful observation, finding evidence to support intuition. This, in turn, leads to discussions about interpretation, as one viewer claims that a given detail means something and another disagrees and suggests an alternative meaning. The VTS approach mirrors that of experienced clinicians. Consider the following panel as an example of how one might use VTS to facilitate students’ understanding of a patient and her circumstances [9].
Copyright © 2015 by The Pennsylvania State University Press. Reprinted by permission of The Pennsylvania State University Press.
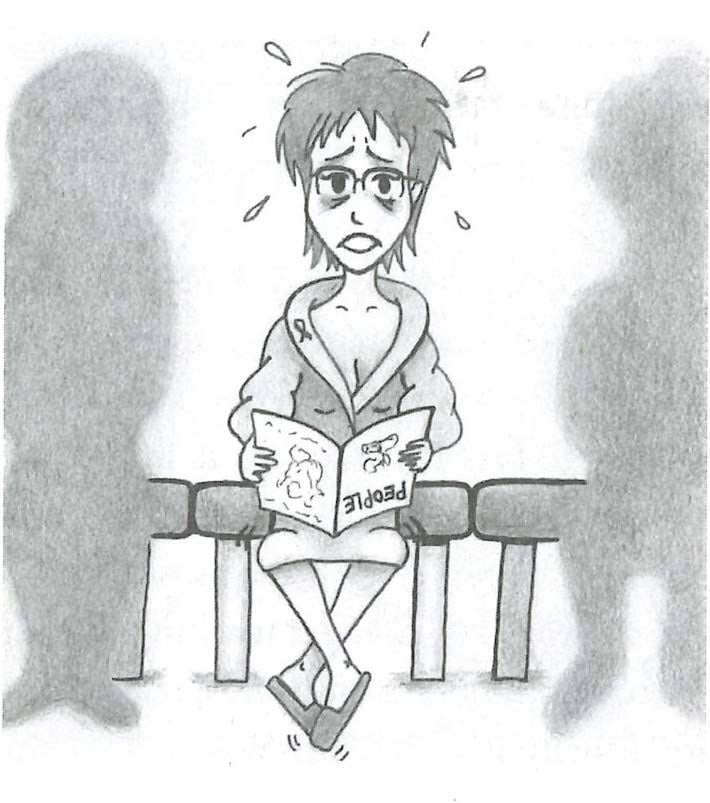
When the first author (KRM) uses this panel with trainees, she modifies VTS a bit and begins by asking, “How does this make you feel?” Responses center around discomfort and fear and lead to the next question, “What’s going on here?” A collective “aha” moment occurs when one person mentions the small ribbon on the right lapel of the patient’s robe: students instantly understand that the story depicted in the panel has something to do with breast cancer. They understand the patient’s fear, noting her wide eyes shadowed in dark circles, and the sweat and nervous tapping of feet, both of which are suggested by emanata, lines or words that protrude from a character or object to show what’s going on physically or internally. Students note that the patient is holding a magazine upside down and that humanoid shadows flank her on either side. She’s not really reading the magazine, nor is she aware of the people beside her; she can concentrate on nothing but the anxiety coursing through her body that’s lost in an oversized robe, the garment that defines her current identity as a vulnerable patient.
In her autobiographical Cancer Vixen: A True Story [10], Marisa Acocella Marchetto depicts herself (and her mother) similarly stunned and afraid as a physician explains an upcoming biopsy. A single panel features two women with bulging eyes sitting across from a physician who is seated behind a desk. A text bubble above the physician contains four lines of scribble, each of which contains a single word or phrase: “cancer,” “lumpectomy,” “may not be invasive,” and “lymph nodes,” respectively. A text box along the top of the panel reads, “Before the dreaded core biopsy, Dr. Mills fills us in.” And at the bottom, another text box reads: “The last doctor’s visit without a tape recorder” [11].
Examining graphic pathographies via VTS can remind students and physicians of the terror patients sometimes feel when faced with an overwhelming diagnosis, as is the case in Smith’s and Marchetto’s panels. Comprehending this truth might inspire empathy for patients or, when feeling isn’t possible, a practice of empathy—calling a patient with test results as soon as they are available, for example, instead of waiting until the end of the workday. The panels can also provide insight into the processes of clinical medicine. From the bug-eyed gaze of Marchetto’s characters and the squiggly lines in the central text bubble, students immediately grasp that the patient is hearing—or at least registering or comprehending—almost nothing of what she is being told. The text box at the bottom underscores the message that consenting a patient is not always as effective as one hopes it will be. The patient herself knows that she will need to record what her physician says in the future so that she can listen to it over and over until it sinks in and makes sense.
Panels like these have important potential benefits for patients as well as medical professionals. For one thing, these first-person perspectives of illness can provide a patient with a sense of community: “other people know what I feel right now; they have survived, and I can, too.” Cultivating a sense of community is a primary goal of support groups, of course, but many people are not comfortable sharing feelings or intimate details of their illness with strangers. Indeed, groups that are meant to provide support sometimes ironically make people feel even more vulnerable when, for instance, members of the group share bad experiences, relapse, or even die [12].
A benefit of support groups that graphic pathographies also provide is helpful information to educate and empower readers. For example, while Marchetto’s comic serves as a cautionary tale about the challenges of meaningful informed consent, it also, as it turns out, can actually help facilitate informed consent. Elsewhere in the pathography, Marchetto presents a series of panels that explain—and raise weighty questions about—the extravasation that can occur during chemotherapy. While patients might be told that chemicals can leak and damage tissue, the comic conveys specific implications of what that possibility might look like in real life. For Marchetto, this single side effect could cause permanent disability because she draws cartoons for a living [10]. Fuller comprehension of the implications of extravasation might suggest to a reader of Cancer Vixencritical questions worth pursuing with her own physician before beginning treatment.
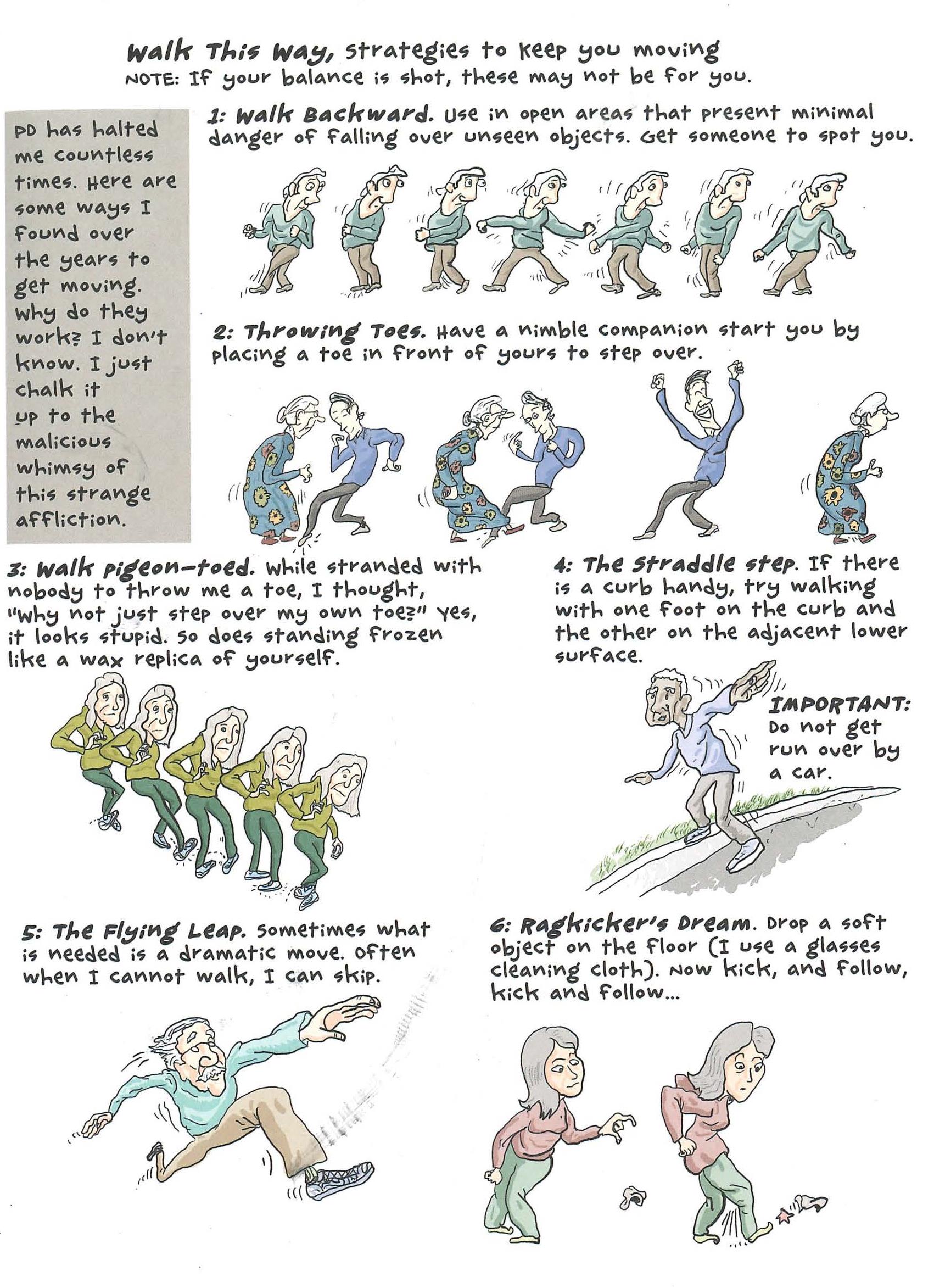
Peter Dunlap-Shohl provides another example of how graphic pathographies can empower patients in practical ways. In My Degeneration: A Journey Through Parkinson’s [13], he provides a full-page panel of “strategies to keep you moving” for those with Parkinson’s disease.
Copyright © 2015 by The Pennsylvania State University Press. Reprinted by permission of The Pennsylvania State University Press.
The sequential pictures essentially create a how-to guide for practicing the various forms of walking, and the words add helpful context, clarification, and caution. As we see from Marchetto’s and Dunlap-Shohl’s work, readers can learn practical, even technical, information in the privacy of their own homes as they view panels at their own pace. They can think about what they see, they can research terminology, and they can take the book with them to their next doctor’s appointment to ask for clarification—all of which can contribute to meaningful informed consent.
Most graphic pathographies touch, in some way, on mortality—likely because the illness experiences have been profound enough to impel people to tell their stories in the first place. Understandably, most people find discussions about dying and death difficult and distressing. Sharon Rosenzweig illustrates family members’ “dis-ease” in “Judgment Call” [14].
Figure 3.
Panel 3 from “Annals Graphic Medicine—Judgment Call,” by Sharon Rosenzweig [14]
Rosenzweig draws viewers into a vortex of jumbled, contradictory emotions in the center section of the panel, such that the reader vicariously participates in her anxiety. The reader is unmoored, unsure how to move through the panel—figuratively mirroring the lack of direction Rosenzweig experiences: the expected left-to-right, top-to-bottom process of reading does not hold here. In resonating with the chaos that Rosenzweig depicts, patients and family members might feel a sense of community, while physicians might be reminded anew of the need for empathy when dealing with exhausted families.
Despite the emotional challenges that come with end-of-life conversations, seasoned physicians know that they are critical for competent and compassionate care of the whole person. In figure 4, Michael J. Green’s autobiographical “Betty P.” [15], which Green initially wrote as a poem for the Penn State Hershey Physicians Writers Group that the first author (KRM) founded and hosts, illustrates the damage that can result to both patient and doctor when these conversations don’t happen.
Figure 4.
Panel 3 from “Annals Graphic Medicine—Betty P.,” written by Michael J. Green and illustrated Ray Rieck [15]
Reading that this terminally ill woman has been abandoned by her children and seeing the anguish etched in her face, the reader is able to view the situation through the doctors’ eyes. Surely, allowing a merciful death would be better than intervening and thereby prolonging the woman’s agony. When the patient codes and the intern, Green, must administer CPR, the reader vicariously participates in his agony as well [15].
Figure 5.
Panel 5 from “Annals Graphic Medicine—Betty P.,” written by Michael J. Green and illustrated by Ray Rieck [15]
The repulsion Green feels as he batters her frail body is surpassed only by the guilt he feels for violating his own moral code. Forced by circumstance to disobey his oath to “First, do no harm,” Green is haunted by guilt and shame—so much so that he not only recounts this story to his younger colleague but also creates this comic years after the fact. In this way, “Betty P.” is an excellent tool to use with medical students to impress upon them the importance of having end-of-life conversations, no matter how difficult they might be. “Betty P.” can also be a helpful tool to use with patients and family members to impress upon them the importance of making their wishes known before it’s too late.
Graphic pathographies, like any other tool, are not a panacea for learning or for teaching. The greatest impediment to their wholesale use in clinical medicine is likely the misguided perception that “comics are for kids” and therefore have little to offer participants in the high-stakes arena of managing serious disease. However, as the recent shift toward using comics to further both patients’ and physicians’ understanding of illness suggests, the field of graphic medicine has important implications for the empathic practice of whole-person medicine.
Green MJ, Myers KR. Graphic medicine: use of comics in medical education and patient care. BMJ. 2010;340:c863. http://www.bmj.com/content/340/bmj.c863.long. Accessed October 12, 2017.
Myers KR. Graphic pathography in the classroom and the clinic: a case study. In: Czerwiec M, Williams I, Squier SM, Green MJ, Myers KR, Smith ST. Graphic Medicine Manifesto. University Park, PA: Pennsylvania State University Press; 2015:88-93.
Smokyland. Comics words. https://smokyland.blogspot.com/2007/04/comics-words.html?m=0. Published April 12, 2007. Accessed September 28, 2017.
Keller DM. Comic strips carry serious messages for medical students. Medscape. March 4, 2013.
McCloud S. Understanding Comics: The Invisible Art. Northampton, MA: Tundra Publishing; 1993:27.
Schneider EF. Quantifying and visualizing the history of public health comics. In: iConference 2014 Proceedings:995-997.
https://www.ideals.illinois.edu/bitstream/handle/2142/47384/340_
ready.pdf?sequence=2. Published 2014. Accessed December 14, 2017.
Murawski M. Openthink: visual thinking strategies (VTS) and museums. Art Museum Teaching. https://artmuseumteaching.com/2014/04/29/openthink-visual-thinking-strategies-vts-museums/. Published April 29, 2014. Accessed September 28, 2017.
Smith PW. Graphic pathography in the classroom and the clinic: a case study. In: Czerwiec M, Williams I, Squier SM, Green MJ, Myers KR, Smith ST. Graphic Medicine Manifesto. University Park, PA: Pennsylvania University Press; 2015:99.
Marchetto MA. Cancer Vixen: A True Story. New York, NY: Alfred A. Knopf; 2006.
Marchetto, 89.
Katz L. Support group. In Myers KR, ed. Illness in the Academy: A Collection of Pathographies by Academics. West Lafayette, IN: Purdue University Press; 2007:160.
Dunlap-Shohl P. My Degeneration: A Journey Through Parkinson’s. University Park, PA: Pennsylvania State University Press; 2015:35.




{kind=link}
{kind=link}
{kind=link}