Medical Education
Jan 2016

In the aftermath of the Flexner Report of 1910, American medical education emphasized scientific knowledge over communication and empathy [1]. However with the “information age” propelling rapid scientific advancement, creating an overwhelming abundance of information, and democratizing the availability of medical information (though not necessarily medical knowledge) to anyone with Internet access, medical education has been thrust into a new era that emphasizes empathy, humanity, communication, and partnership with patients and families. As a result, medical schools are revising their curricula to integrate principles of patient- and family-centered care (PFCC) and to emphasize the importance of communication and how physicians can help patients and families translate information into helpful, care-oriented knowledge during clinical encounters. In the words of American physician Francis Peabody (1881-1927), “One of the essential qualities of the clinician is interest in humanity, for the secret of the care of the patient is in caring for the patient” [2]. The addition of PFCC content to medical school curricula is poised to bring caring and humanity into the education of our future clinicians.
The Institute for Patient- and Family-Centered Care defines PFCC as an approach to the planning, delivery, and evaluation of health care that is grounded in mutually beneficial partnerships among health care professionals, patients, and families [3]. Families are included in this definition of health care relationships because they can be important sources of care and support for patients.
In 2001, the Institute of Medicine report Crossing the Quality Chasm: A New Health System for the 21st Century made patient-centeredness one of “the aims for improvement” for the health care system, arguing that patient and family engagement and partnerships result in higher patient satisfaction, improved clinical outcomes, and reduced errors [4]. Almost a decade later, the Lucian Leape Institute Roundtable on Reforming Medical Education report, Unmet Needs: Teaching Physicians to Provide Safe Patient Care, urged medical educators to place more emphasis on teaching systems, teamwork, and patient and family engagement to promote safe care practices [5]. Furthermore, following passage of the Affordable Care Act of 2010, the Center for Medicare and Medicaid Services (CMS) aligned its priorities with PFCC, investing in patient safety by tying reimbursement to patient (and family) satisfaction, patient outcomes, and quality and safety Physician Quality Reporting System (PQRS) data [6].
To keep current with national standards, as well as culture shifts in health care around patient and family engagement and technology usage, the University of Michigan Medical School (UMMS) implemented a major curriculum revision, which included the incorporation of PFCC concepts. Co-authors of this paper Jennifer Stojan and Joseph House have been intimately involved in the revisions. To accomplish this goal, UMMS engaged co-authors Kelly Parent and Kori Jones from the University of Michigan Health System’s Department of Patient- and Family-Centered Care and its volunteer patient-family advisors (VPFAs) to develop and implement coursework for medical students that emphasizes PFCC principles in classroom and home settings.
PFCC was incorporated into two courses in the new UMMS curriculum: “Doctoring: Caring for Patients, Families and Communities” (Doctoring), a longitudinal course that includes patient-student partnerships and home visits to help lay the foundation for thoughtful and skilled clinical practice, and “Initial Clinical Experience” (ICE), a longitudinal clinical experience course organized around three aspects of health care—patients, teams, and systems. The goal in each of these courses is to improve communication skills of both patients and the health care team, thereby improving the care of the patients within the health care system and recognizing the value of partnering with patients and family members.
Prior to the PFCC orientation, an anonymous online survey was sent to the first-year UMMS medical students; 127 out of 170 (75 percent) responded assessing their beliefs about the value of patient and family engagement and participation. Students were asked three PFCC-related questions (see figures 1-3). The data indicated that a majority of new UMMS students believe that the needs and ideals of the patient and family, as well as their participation in care planning and decision making, should be central to physician practice; however, a significant number of students entering medical school either were unsure whether, or did not believe that, family members should be part of the care team (40.9 percent) or welcomed to participate in care (37 percent). These findings indicate that if we expect students to embrace patients and family members as part of the care team, we must engage patients and families as educators with theoretical learning, learning through story, facilitated discussion, and personal reflection beginning the first week of medical school and continuing throughout all phases of medical training.
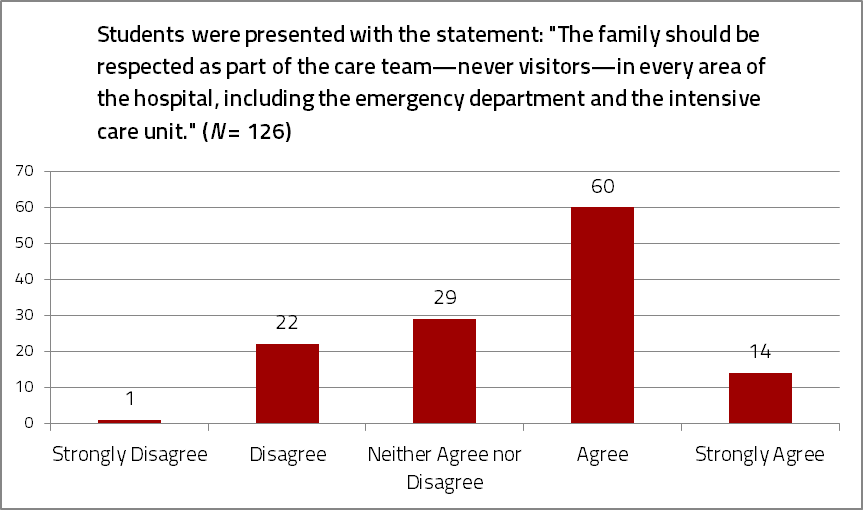
Figure 1. Incoming UMMS medical students’ responses to a survey question about respecting family presence.
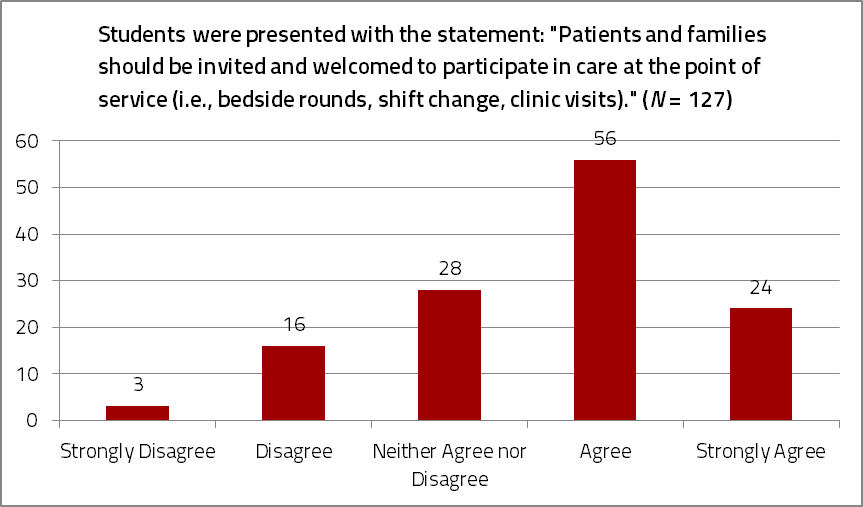
Figure 2. Incoming UMMS medical students’ responses to a survey question about recognizing the role of the patient and family as health care team members.
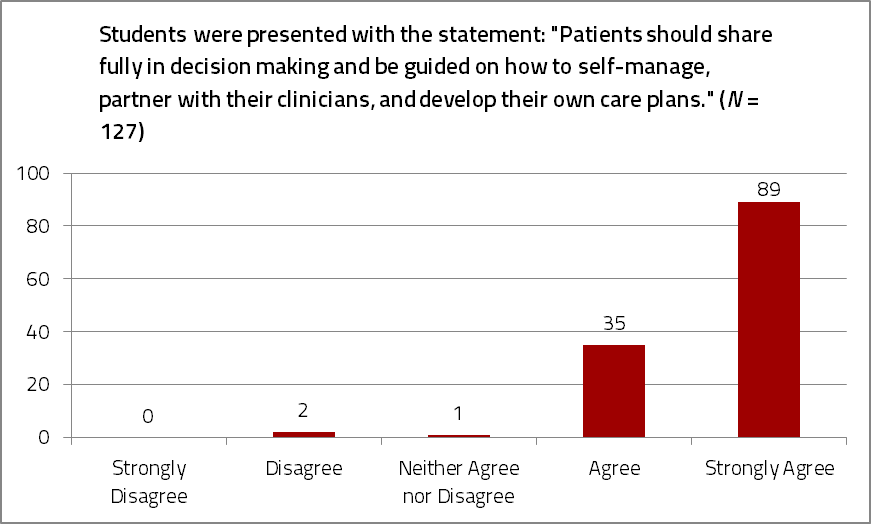
Figure 3. Incoming UMMS medical students’ responses to a survey question about welcoming the participation of patients’ families in medical decision making and self-management.
Department of PFCC staff and VPFAs served multiple roles in curriculum design, development, and implementation. For Doctoring, PFCC staff helped to recruit VPFAs who could serve as meaningful mentors to medical students and as patient-family panelists whose personal stories would illustrate lessons on communication, health disparities, stigma, and social and cultural identities. PFCC staff and VPFA collaborated with ICE course faculty to create a four-hour orientation consisting of an overview of PFCC; a panel representing the perspectives of four patients and family members and one surgeon; videos emphasizing empathy, patient safety, and PFCC point-of-care interactions; and VPFA-facilitated small group discussions encouraging students to reflect upon all elements of the orientation. To create this curriculum, PFCC staff solicited VPFA input on topics to be included. Suggestions encompassed how to listen, how to communicate both factual and emotional information, how to engage patient and family participation, and how to address difficult situations and escalating behaviors. VPFAs also shared ideas for teaching methods: storytelling, personal coaching, small-group discussion, simulation training, case studies, shadowing patients and families, and interactive exercises teaching how to identify words that are understandable and inclusive.
Medical students were also engaged in the curriculum design process. A focus group of seasoned medical students was convened to better understand a “stereotypical profile” and mindset of first-year medical students. They were asked what they wished they would have learned about empathy, relationships, and communication as new medical students and what they considered to be effective teaching methods. In response to the fact that as many as 50% of first-year medical students expect to become surgeons and are unclear as to how PFCC principles relate to the practice of surgeons, a surgeon was added to the orientation panel to lay the foundation of a patient- and family-centered surgical culture early in medical education.
Didactic education. Classroom education serves as the theoretical foundation for the benefits of patient and family presence and partnership at the point-of-care; interpersonal skills and communication and education strategies that promote trust, partnership and self-management; and the identification of opportunities to engage patients and families to enhance quality and safety. Presentations include the sharing of literature reviews and best practice models as well as tips and strategies for “what works,” as told by those who have received care.
A focus on stories. VPFA panels provide an important venue to learn through story. In both courses, stories serve as the heart of education given their ability to create human connections and emotionally move and motivate us to action. VPFA panelists address the challenges and burdens of illness and injury, the social complexities and stigma of illness and hospitalization, and the differences between empathetic and sympathetic interactions. Story as a personal motivator was also explored. In the pre-orientation survey, incoming students were asked to anonymously share in writing personal health care stories that affected them in profoundly positive or negative ways. Seventy-eight out of 127 students (61 percent) responded with memorable stories (38 positive and 40 negative), and five students expressed that it was these profound experiences that led them to pursue a career in medicine.
Patients and families as mentors. The Doctoring course matches two first-year medical students with a patient mentor who is living with a chronic illness or condition. These patient mentors welcome students into their lives and homes, engaging the students in open and honest dialogue about their illness, health care team, and health care system navigation. This unique opportunity allows students to understand illness and the health care system through the “patient’s eyes.”
VPFAs as discussion facilitators. After listening to didactic presentations and personal health care experience stories, students have the opportunity to discuss, both in small groups and in writing, how these stories affect us as people and future physicians. PFCC staff selected and trained VPFAs to serve as discussion facilitators. The methodology was to create a space where those who provide care and those who receive care could ask questions, listen to answers, and find a commonality—recognizing that commonality has the potential to reduce vulnerability and stigma, bridge racial and cultural divides, and build trust and relationships.
Although VPFAs as educators provide many benefits, several concerns have been raised as well. Staff and faculty have expressed concern about the time and resources needed to select and train patient and family members to be effective educators. Additionally, concerns have been raised regarding patient and family members pushing their own agendas, anticipated difficulty in maintaining professional boundaries when VPFAs are co-educators one day and patient and family members receiving care the next, and the emotional weight that affecting stories and relationships may have on the emotional development of the student, particularly when there is such limited time for faculty to debrief with students.
Students have also expressed concerns about scheduling and spending time with their patient mentor and being equitably exposed to patient-family panelists who represent a balance of real-life experiences (e.g., well-educated and health care savvy vs. health illiterate and underserved). Efforts to familiarize students with patients and families from diverse cultural, geographical, educational, and socio-economic backgrounds is a constant challenge that requires innovative solutions that build trust and create relationships with underserved communities. A series of home visits in Doctoring is one effort that UMMS has programmed to help respond to these needs.
Finally, to ensure that the principles of PFCC are sustained across the medical education continuum, the curriculum must continue throughout medical school and into residency and fellowship. We must also find a way to set standards of education for attending physicians on these same principles of empathy, communication, and partnership, for without their validation, rising clinicians will not be able to extend classroom learning to the clinical setting.
While it is too early to determine how PFCC curriculum influences behavior and patient care over time, a preliminary evaluation of medical student impressions of this curriculum has indicated a very favorable response to the PFCC curriculum objectives. More than 94 percent “agreed” or “strongly agreed” that the sessions increased their understanding of: “the challenges of illness/injury for patients and families,” “the benefits of patient and family partnerships at the point of care,” and “the different elements of patient- and family-centered care applied in clinical settings.” In an excerpt of an essay reflecting her impressions of the PFCC curriculum, one UMMS first-year medical student grasped the intended goals of the curriculum:
I sat in the lecture hall donning my short white coat for the first time as we were launched into a talk about something called “Patient- and Family-Centered Care” where we heard about the importance of incorporating family values and beliefs into making medical decisions and partnering ‘with’ patients rather than doing things ‘to and for’ them…. Here we were, first year medical students who had not even begun our basic science courses yet. We could barely pronounce the conditions these patients named, let alone understand them. We had no knowledge of the organ systems affected by their illnesses or the pathology of their diseases. There we were, in the audience, with our white coats on, our only contributions being a set of open ears and a desire to see their experience through their eyes…. And that’s when it hit me—this was why we were there. To see, from the very beginning, that patients can be experts in their own medical experience; to recognize that our personal interactions can be just as important as understanding the medical science behind their illnesses; and to realize that we are not here to be perfect human beings, rather we are here to grow into professionals who can connect with and share in the experience of people who seek our help.
We are assessing students at the end of each term with respect to their skill in communication, patient care, knowledge, and participation surrounding socio-behavioral topics and are exploring the engagement of VPFAs as part of the evaluation process. Revision of curriculum content and teaching methods will be incorporated accordingly.
Our advice to others seeking to create similar programs is this: first, it is important to engage VPFAs who have diverse personal experiences in the health care system and grasp the core principles of PFCC, are unbiased and able to meet first-year medical students where they are, and are willing to attend training to ensure successful panelist storytelling and small-group facilitation. Second, education should be centered on personal stories and reflection, which creates the foundation for empathic relationships. Third, input from both VPFAs and seasoned medical students should be solicited in designing the PFCC curriculum in a way that will reach the students. Fourth, it is valuable to create an assessment and coaching component so that VPFAs can participate in student evaluation of PFCC principles and behaviors. Finally, it must be recognized that PFCC education is not a “one and done” lecture; it must be continued throughout medical education if true change is to be sustained. Standardization of PFCC-focused processes and expectations among residents, fellows, and attending physicians would ensure that what is being learned in the classroom is being supported and reinforced in patient care.
Peabody FW. Landmark article: March 19, 1927: the care of the patient. JAMA. 1984;252(6):818.
Institute for Patient- and Family-Centered Care. Frequently asked questions. http://www.ipfcc.org/faq.html. Accessed December 3, 2015.
Institute of Medicine Committee on Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
Lucian Leape Institute at the National Patient Safety Foundation. Unmet needs: teaching physicians to provide safe patient care. Report of the Lucian Leape Institute Roundtable on Reforming Medical Education. Boston, MA: National Patient Safety Foundation; 2010. http://c.ymcdn.com/sites/www.npsf.org/resource/resmgr/LLI/LLI-Unmet-Needs-Report.pdf. Accessed November 12, 2015.
Centers for Medicare and Medicaid Services. HCAHPS: Patients’ Perspectives of Care Survey. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-instruments/HospitalQualityInits/HospitalHCAHPS.html. Accessed December 3, 2015.