Medical Education
Sep 2025
Peer-Reviewed

Despite the inclusion of health equity and public health in undergraduate and graduate medical curricula, many medical students and trainees have minimal understanding of health insurance coverage for children of families with low incomes. Since children’s eligibility for Medicaid and the Children’s Health Insurance Program (CHIP) significantly influence their care, this article proposes that students and trainees, especially in pediatrics, should receive formal instruction about Medicaid and CHIP in 3 key areas: program structure; eligibility determinations, redeterminations, and range of covered or partially covered services; and enrollment requirements and processes. This article also suggests the nature and scope of expertise required to responsibly offer such instruction in classroom- and clinic-based settings.
While medical students and residents in the United States are taught much about anatomy, physiology, organ systems, and disease management, education on health insurance and Medicaid is lacking. Of topics learned in medical school, trainees have reported having the lowest confidence in their knowledge of health policy and economics.1 Nevertheless, exposure to health policy and health equity in medical school is occurring through public health clubs or optional public health and health policy electives in medical schools and residencies.2 For example, one student-led program sought to raise awareness of racial bias in medicine and demonstrate how racial injustice can be incorporated in preclinical medical student education.3,4However, few schools or residencies mandate an extensive public health curriculum, and fewer provide comprehensive education on public insurance. The Association of American Medical Colleges reported that 132 of 147 medical schools taught some health care financing in required courses preclinically,5 but, in our experience as recent medical school graduates, this teaching was limited to superficial topics, such as the broad differences between Medicare, Medicaid, and private insurance—content that covered only what is tested on United States Medical Licensing Examination board exams.6
Upon reviewing the board exam content distribution for the specialties of emergency medicine, pediatrics, and family medicine, we found that none require knowledge of health insurance programs, let alone specifics of Medicaid or similar programs.7,8,9 However, the American Medical Association has adopted a policy encouraging medical schools and residencies to provide more in-depth health care economics education.10 Thus, the pressure is on medical schools or individual physicians to cover this content more thoroughly.
Given the brief coverage trainees receive, in this article we first discuss the benefits of coverage and then propose several key points about insurance coverage that trainees should understand: (1) the general structure of Medicaid and the Children’s Health Insurance Program (CHIP), (2) who qualifies for Medicaid as compared to CHIP and what services each cover, and (3) how patients and families can enroll in Medicaid or CHIP. Additionally, we propose who may be the best qualified to deliver this content to medical students and residents.
It is estimated that roughly 36% of children in the United States in 2023 had health insurance coverage through a Medicaid program and 10% through CHIP.11 Additionally, Medicaid and CHIP programs covered two-thirds of children in families with low incomes (below 200% of the federal poverty level, or FPL) in 201512 and approximately 44% of children with special health care needs in 2019.13 Although the rate of uninsured children has dropped to near 5%, it is estimated that approximately 55% of these children qualify for Medicaid or CHIP programs.14,15 Based on these numbers, one can assume that most medical students and residents will care for patients either eligible for or insured by Medicaid or CHIP.
Research suggests that the expansion of Medicaid and CHIP coverage reduces pediatric hospitalizations, care gaps, and mortality and improves health outcomes.16,17,18,19,20 There’s also mounting evidence of the positive impact of insurance coverage beyond children’s immediate health, including higher educational attainment,21 better adult health, and decreased poverty for children and their families on Medicaid,22 although it is hard to differentiate between the impacts of CHIP and Medicaid because children frequently switch between programs as their family’s income fluctuates.
Medicaid is jointly state and federally funded and designed to help individuals with low incomes, including pregnant individuals, families, the elderly, and individuals with disabilities.23 Each state must follow minimum federal requirements but otherwise may administer Medicaid as they see fit.24 There is no cap to the funding match that the federal government provides for qualified services, and states may apply for waivers to administer the program in other ways if it is determined that the proposed changes are in line with Medicaid goals.24,25 Therefore, there is significant variation from state to state in services covered, payment structures, and qualifying income levels. For example, the default pay structure is fee-for-service; however, most states adopt managed care plans.26 Additionally, Medicaid benefits that states can opt into include, but are not limited to, dental care, physical therapy, home health care, hospice, prosthetics, and targeted case management programs.26,27
There’s also mounting evidence of the positive impact of insurance coverage beyond children’s immediate health.
Although Medicaid covers both adults and children, CHIP is focused solely on expanding health insurance coverage for children. CHIP was initially created in 1997 to offer coverage to children in families with household incomes too high to qualify for Medicaid but too low for health care to be affordable.28 CHIP can be operated by states as a separate program from Medicaid or as a Medicaid expansion wherein CHIP is a subprogram of Medicaid. Similarly to Medicaid, CHIP is jointly state and federally funded. While the percentage of CHIP’s funding from the federal government is larger than Medicaid’s (approximately 15% higher), unlike Medicaid, there is a federal cap to the CHIP funds allocated to each state annually.29 Thus, if a state has hit its annual cap, applicants are not allowed to enroll or are placed on a waiting list.
Although pediatric Medicaid and CHIP cover many of the same services, such as routine checkups and vaccinations,27,30 there are some key differences between the two. The federal government mandates that Medicaid programs in every state fully cover all services outlined under the Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) Program for any child under the age of 21, which includes comprehensive and preventative care consisting of vision and hearing care, mental health care, developmental services, and dental care.20,30,31 CHIP programs are not subjected to the same EPSDT coverage minimums, which can lead to gaps in services depending on the state, as states can opt in to offer some services that are optional at the federal level. Moreover, for pediatric Medicaid programs, premiums and cost sharing are federally prohibited in most cases, whereas many CHIP programs have premiums or cost sharing that increase in proportion to family income.32
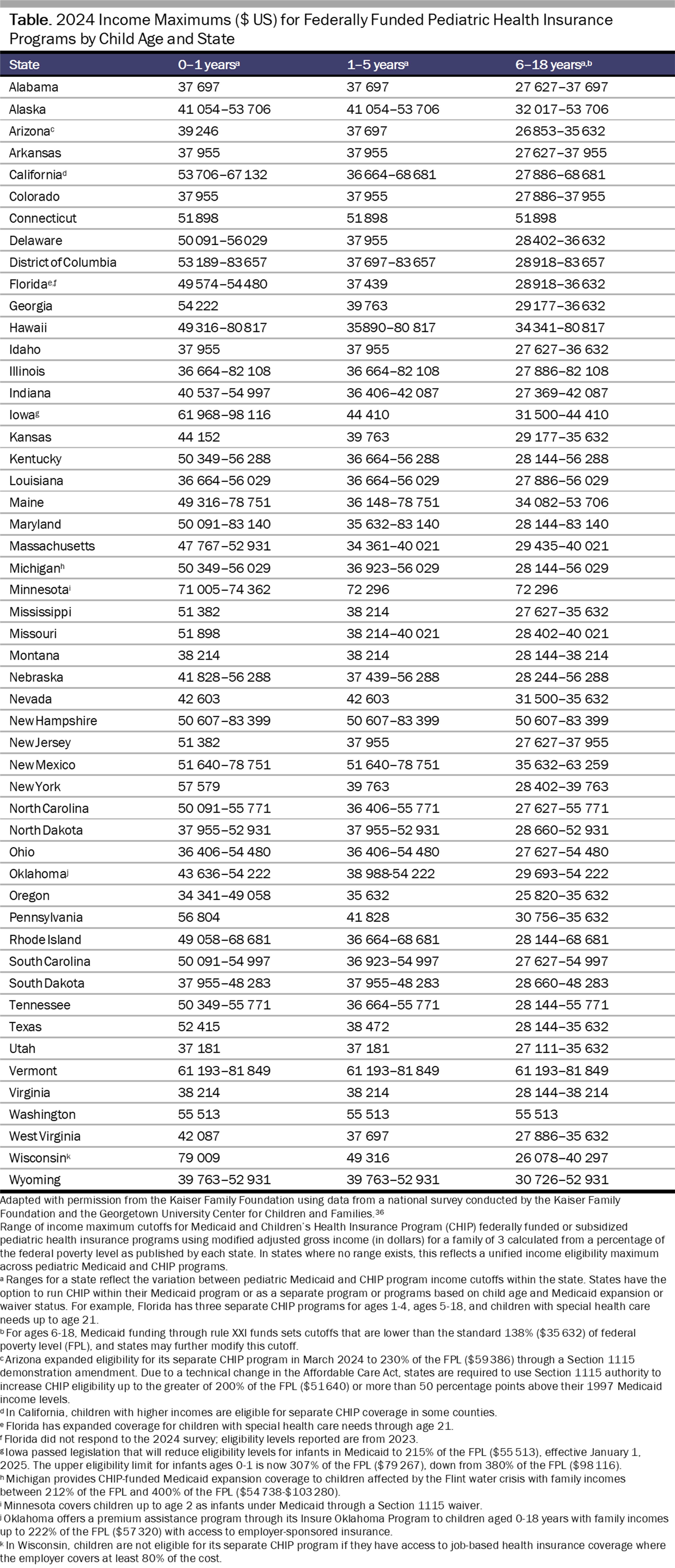
Eligibility for pediatric Medicaid and CHIP is primarily based on a child’s age, family income, family size, and insurance status. Unlike Medicare for persons at least 65 years of age, eligibility for both pediatric Medicaid and CHIP requires the child to be uninsured; CHIP and Medicaid cannot be used as secondary insurance.33 Additionally, a child cannot be on both Medicaid and CHIP in the traditional sense of primary and secondary insurance.33For both programs, modified adjusted gross income (MAGI) is used to determine eligibility expressed as a percentage of the FPL.34 For a family of 3 in the 48 contiguous states and the District of Columbia, as of 2024, the FPL is $25 820 and has increased annually with inflation.35 (The FPL is slightly higher in Hawaii and Alaska due to increased cost of living35). The percentage of FPL that is used as a cutoff varies by state.34 Recent state-specific data on pediatric Medicaid and CHIP eligibility from 2024 demonstrate a range of FPL cutoffs stratified by age—from 107% of the FPL ($27 627) in North Carolina (ages 6-18) to 324% of the FPL ($83 657) in Washington, DC (ages 0-19)36 (see Table). If Medicaid is expanded in a state, there are often higher income limits for both programs, with CHIP most often having the highest family MAGI eligibility cutoff. Finally, it should be noted that children in the foster care system may qualify for extended coverage until age 26, although the availability of this provision varies by state.23
Additionally, federal regulations on citizenship and immigration status limit Medicaid or CHIP access for noncitizens. Research shows that states without expanded eligibility for noncitizens have less overall pediatric health care utilization.37 Noncitizens are subject to a 5-year waiting period before being eligible for these services, with exceptions being made for lawful permanent residents (green card holders), Cuban or Haitian entrants, members of nationally recognized Indian Tribes, and for those who entered the United States under asylum or refugee status or immigrated due to being victims of domestic violence or trafficking.38,39 Reassurance should be offered to immigrants applying for health insurance that, as long as they are not requiring long-term nursing home care, the US Citizenship and Immigration Services does not take into account Medicaid or CHIP utilization as part of the public charge determination for immigration status.40 However, requirements can change with different presidential administrations and executive guidance on how to apply the public charge ruling—an example being a recent change in guidance for adult patients only.41 There is some evidence that changes in executive office guidance on the public charge ruling affect applicants’ decisions about enrolling or reenrolling in pediatric Medicaid and CHIP. For example, the American Community survey found a 20% drop in Medicaid and CHIP participation among noncitizens between 2016 and 2019, and another 2019 survey of health centers found that 38% reported being aware of immigrant patients declining to enroll their children in Medicaid and 28% reported being aware of immigrant patients disenrolling or declining to reenroll their children in Medicaid over the previous year.42,43 Even though a child’s use of Medicaid or CHIP does not affect immigration applications, 22% of surveyed health centers in 2019 saw a decrease in immigrant parents seeking care for their children.42
Clinicians’ understanding of the basic, state-specific requirements for Medicaid and CHIP eligibility, which vary based on income and legal situation, as well as of the services each covers, can help guide their recommendations to patients and families. Despite the complexities of eligibility and coverage rules, most states have a simple and unified application process for Medicaid and CHIP. Importantly, a parent being ineligible for Medicaid does not mean their child will be ineligible, because familial income cutoffs for children (see Table) are typically higher than adult cutoffs. Even if the adults in the household are insured through their employer, their children are typically still eligible for Medicaid or CHIP if they meet the income cutoffs.39 Parents, grandparents, and guardians may complete the applications for Medicaid or CHIP on behalf of their children.39 Teenagers who are emancipated are also eligible to complete their own application.39 While social workers can help families navigate the application process, they are often unable to directly file on behalf of someone. Some states have employed health insurance marketplace or Medicaid navigators44 who are familiar with eligibility rules and can help applicants find the most appropriate plan for a child and their family. Applications can be found on each state’s Medicaid or CHIP website, their health insurance marketplace, or the federal government website.28,45,46
All this information is essential to providing improved patient care for children and their families. Medical school and residency curricula tend to have limited room for additional lectures and information sessions, but we feel that more in-depth education about Medicaid and CHIP is warranted. We know that improving access to health care improves health outcomes, and students and residents should have the tools and knowledge to advocate for their patients to obtain appropriate health care coverage. Although education on Medicaid and CHIP may be covered during pediatric and family medicine rotations, we also propose that medical schools incorporate this information in the preclinical years of medical education. Social workers and other financial administrative staff who assist patients and families with Medicaid registration, as well as health insurance navigators, may be best equipped to teach this information, although physicians who care for a significant number of underinsured and uninsured patients may also be able to teach these lessons. Lectures from staff at state Medicaid offices may also be beneficial, as they can offer trainees a better understanding of the enrollment process. Moreover, content on Medicaid and CHIP could be included in lectures on public health or in general medicine courses. Students should not have to “opt in” to a class or program that offers this information. Some suggestions for improving students’ knowledge of public insurance include rotations with a social worker and spending a day with staff who assist patients in registering for Medicaid and CHIP. All students should enter clinical rotations and residency with this knowledge, and residencies should integrate training on Medicaid and CHIP into their scheduled didactic sessions. Without knowledge of insurance options and coverage for patients with low incomes, physicians cannot provide adequate care for all patients.
In summary, medical schools and residencies should incorporate education on Medicaid and CHIP, as insurance has a substantial impact on patient care and outcomes. Understanding what Medicaid and CHIP are, who qualifies for pediatric Medicaid and CHIP, what services each cover, and how patients and families can enroll in Medicaid or CHIP is essential to improving pediatric health outcomes and health equity.
Skochelak SE, Hammoud MM, Lomis KD, et al, eds. Health Systems Science. 2nd ed. Elsevier; 2020.
Public health pathways for medical students. Association of American Medical Colleges. Accessed March 7, 2025. https://students-residents.aamc.org/attending-medical-school/article/public-health-pathways-2
Lynn TM, D’urzo KA, Vaughan-Ogunlusi O, et al. The impact of a student-led anti-racism programme on medical students’ perceptions and awareness of racial bias in medicine and confidence to advocate against racism. Med Educ Online. 2023;28(1):2176802.
Curriculum topics in required and elective courses at medical school programs. Association of American Medical Colleges.
Federation of State Medical Boards of the United States; National Board of Medical Examiners. USMLE® content outline. Federation of State Medical Boards of the United States; National Board of Medical Examiners; 2022. Accessed March 7, 2025. https://www.usmle.org/sites/default/files/2022-01/USMLE_Content_Outline_0.pdf
American Board of Pediatrics. General pediatrics content outline: in-training, certification, and maintenance of certification exams. American Board of Pediatrics; 2024. Accessed March 7, 2025. https://www.abp.org/sites/public/files/pdf/content-outline-general-pediatrics-2024.pdf
Qualifying exam. American Board of Emergency Medicine. Accessed March 7, 2025. https://www.abem.org/get-certified/qualifying-exam/
American Board of Family Medicine. ABFM certification examination content. American Board of Family Medicine; 2019. Accessed March 7, 2025. https://www.theabfm.org/app/uploads/2024/02/Exam-Content-Outline.pdf
AMA to ensure future physicians receive health care economics training. News release. American Medical Association; November 19, 2019. Accessed March 7, 2025. https://www.ama-assn.org/press-center/press-releases/ama-ensure-future-physicians-receive-health-care-economics-training
Vankar P. Share of children aged 19 and under with Medicaid health insurance in the United States from 2017 to 2023. Statista. October 21, 2024. Accessed March 7, 2025. https://www.statista.com/statistics/1334558/children-with-medicaid-coverage-in-the-us/
Artiga S, Ubri P. Key issues in children’s health coverage. KFF. February 15, 2017. Accessed April 11, 2025. https://www.kff.org/medicaid/issue-brief/key-issues-in-childrens-health-coverage/
Osorio A. Research update: Medicaid/CHIP are critical resources for children with special health care needs. Center for Children and Families, Georgetown University McCourt School of Public Policy. October 18, 2021. Accessed June 2, 2025. https://ccf.georgetown.edu/2021/10/18/research-update-medicaid-chip-are-critical-resources-for-children-with-special-health-care-needs/
Tolbert J, Cervantes S, Bell C, Damico A. Key facts about the uninsured population. KFF. December 18, 2024. Accessed April 7, 2025. https://www.kff.org/uninsured/issue-brief/key-facts-about-the-uninsured-population/
Drake P, Rudowitz R, Tolbert J, Damico A. A closer look at the remaining uninsured population eligible for Medicaid and CHIP. KFF. March 15, 2024. Accessed April 8, 2025. https://www.kff.org/uninsured/issue-brief/a-closer-look-at-the-remaining-uninsured-population-eligible-for-medicaid-and-chip/
Paradise J. The impact of the Children’s Health Insurance Program (CHIP): what does the research tell us? KFF. July 17, 2014. Accessed March 7, 2025. https://www.kff.org/report-section/the-impact-of-the-childrens-health-insurance-program-chip-issue-brief/
Medicaid and CHIP coverage. HealthCare.gov. Accessed October 5, 2024. https://www.healthcare.gov/medicaid-chip/
Burns A, Hinton E, Rudowitz R, Mohamed M. 10 things to know about Medicaid. KFF. February 18, 2025. Accessed May 30, 2025. https://www.kff.org/medicaid/issue-brief/10-things-to-know-about-medicaid/
Williams E, Mudumala A, Rudowitz R, Burns A. Medicaid financing: the basics. KFF. January 29, 2025. Accessed October 11, 2024. https://www.kff.org/medicaid/issue-brief/medicaid-financing-the-basics/
Federal requirements and state options: how states exercise flexibility under a Medicaid state plan. Medicaid and CHIP Payment and Access Commission. August 2018. Accessed March 7, 2025. https://www.macpac.gov/publication/federal-requirements-and-state-options/
Medicaid and CHIP Payment and Access Commission. Federal requirements and state options: benefits. Medicaid and CHIP Payment and Access Commission; 2017. Accessed April 8, 2025. https://www.macpac.gov/wp-content/uploads/2017/03/Federal-Requirements-and-State-Options-Benefits.pdf
History and impact of CHIP. Medicaid and CHIP Payment and Access Commission. February 5, 2018. Accessed April 9, 2025. https://www.macpac.gov/subtopic/history-and-impact-of-chip/
Financing. Medicaid.gov. Accessed October 5, 2024. https://www.medicaid.gov/chip/financing/index.html
CHIP benefits. Medicaid.gov. Accessed April 8, 2025. https://www.medicaid.gov/chip/benefits
Early and periodic screening, diagnostic, and treatment. Medicaid.gov. Accessed March 7, 2025. https://www.medicaid.gov/medicaid/benefits/early-and-periodic-screening-diagnostic-and-treatment/index.html
Key CHIP design features. Medicaid and CHIP Payment and Access Commission. January 11, 2021. Accessed March 7, 2025. https://www.macpac.gov/subtopic/key-design-features/
CHIP eligibility and enrollment. Medicaid.gov. Accessed March 7, 2025. https://www.medicaid.gov/chip/chip-eligibility-enrollment/index.html
Medicaid, Children’s Health Insurance Program, and basic health program eligibility levels. Medicaid.gov. Accessed September 10, 2024. https://www.medicaid.gov/medicaid/national-medicaid-chip-program-information/medicaid-childrens-health-insurance-program-basic-health-program-eligibility-levels/index.html
Medicaid and CHIP income eligibility limits for children as a percent of the federal poverty level. KFF. May 1, 2024. Accessed September 10, 2024. https://www.kff.org/affordable-care-act/state-indicator/medicaid-and-chip-income-eligibility-limits-for-children-as-a-percent-of-the-federal-poverty-level/
Rosenberg J, Shabanova V, McCollum S, Sharifi M. Insurance and health care outcomes in regions where undocumented children are Medicaid-eligible. Pediatrics. 2022;150(3):e2022057034.
Coverage for lawfully present immigrants. HealthCare.gov. Accessed March 7, 2025. https://www.healthcare.gov/immigrants/lawfully-present-immigrants/
Frequently asked questions. InsureKidsNow.gov. Accessed March 7, 2025. https://www.insurekidsnow.gov/find-coverage-your-family/frequently-asked-questions
Public charge resources. US Citizenship and Immigration Services. Updated April 8, 2025. Accessed April 11, 2025. https://www.uscis.gov/green-card/green-card-processes-and-procedures/public-charge/public-charge-resources
Tolbert J, Artiga S, Pham O. Impact of shifting immigration policy on Medicaid enrollment and utilization of care among health center patients. KFF. October 15, 2019. Accessed March 7, 2025. https://www.kff.org/report-section/impact-of-shifting-immigration-policy-on-medicaid-enrollment-and-utilization-of-care-among-health-center-patients-issue-brief/
Capps R, Fix M, Batalova J. Anticipated “chilling effects” of the public-charge rule are real: census data reflect steep decline in benefits use by immigrant families. Migration Policy Institute. December 2020. Accessed March 7, 2025. https://www.migrationpolicy.org/news/anticipated-chilling-effects-public-charge-rule-are-real
In-person assistance in the health insurance marketplaces. Centers for Medicare and Medicaid Services. Updated April 11, 2025. Accessed May 30, 2025. https://www.cms.gov/marketplace/in-person-assisters/programs-procedures/in-person-assistance
Find out if you can get health coverage now. HealthCare.gov. Accessed March 7, 2025. https://www.healthcare.gov/screener/
Where can people get help with Medicaid and CHIP? Medicaid.gov. Accessed March 7, 2025. https://www.medicaid.gov/about-us/where-can-people-get-help-medicaid-chip/index.html



