Medicine and Society
May 2024
Peer-Reviewed

Antimicrobial resistance (AMR) is a looming pandemic whose poor health outcomes are unlikely to be equitably distributed. This article focuses on intersections between AMR and inequities in health care workplaces in the United States and identifies the following as key problems: lack of published data on task-specific occupational health risks related to colonization and infection with antimicrobial-resistant pathogens, limited scientific literature reporting on race and ethnicity, and poor access to infection control educational opportunities for minoritized health care workers. This article argues that an equitable approach to remediating these problems requires improving surveillance and expanding research on how AMR is likely to influence health outcomes among members of the US-based health care workforce.
Antimicrobial resistance (AMR) is a growing global threat that poses significant challenges to public health. AMR arises when bacteria or fungi undergo genetic changes that render them unresponsive to antibiotic treatments, leading to infections that are more likely to cause severe illness or death. In the United States alone, nearly 3 million infections annually are attributable to resistant pathogens.1 AMR is associated with not only increased risk of severe infections but also longer hospital stays and increased mortality.1,2
If AMR is an upcoming pandemic, it is now abundantly clear that it will not affect us all equally. Certain racial and ethnic groups in the United States are disproportionately impacted by the burden of AMR.3,4,5 As an example, Black patients have higher rates of hospital onset and community-acquired methicillin-resistant Staphylococcus aureus (MRSA) infections than White patients.6 These disparities may be due to Black patients having less access to affordable medical care, a higher likelihood of poverty and crowded living conditions, and more documented chronic medical comorbidities than White patients, all of which contribute to extended hospital stays.6 Studies have also shown that MRSA colonization and infection are more common in patients with public health insurance and those with low socioeconomic status.7,8 This trend has been documented in other antimicrobial-resistant infections, such as drug-resistant tuberculosis, penicillin-resistant streptococcus pneumoniae, and urinary tract infections with multidrug-resistant pathogens.4,9,10
Health care workers are on the front lines of the fight against AMR, as they are responsible for prescribing and administering antibiotics and implementing infection prevention and control measures. Health care workers who belong to racial or ethnic minority groups often hold the lowest-paid and most physically demanding jobs in health care.11,12 For example, Dill and Duffy showed that Black women have the highest likelihood of working in the long-term-care sector and in nurse aide positions.13 Racial and ethnic minority groups are overrepresented in health care positions that are not only underpaid but also often under-resourced, require overtime work, or involve tasks that may greatly increase occupational exposure to antimicrobial-resistant pathogens.13 This manuscript examines the intersection of AMR and health care workplace equity in the United States and proposes measures to study and combat these challenges.
Workplace inequities can impact health care workers’ occupational exposure to AMR. Workers concentrated in health care positions that do not require an advanced medical degree (nursing aides, transport staff) are often responsible for tasks that involve prolonged patient contact, such as bathing, which could increase risks of occupational exposure to AMR pathogens. These positions are often disproportionately filled by workers from racial and ethnic minority groups.14,15 A multinational study conducted in Europe from 2008 to 2011 demonstrated that personnel who feed patients had increased risk of colonization with extended-spectrum beta lactamase-producing Enterobacterales compared to other health care workers.16 We suspect that workers who handle bathing, toileting, mobilizing, and transporting patients might be similarly at higher risk. However, there are limited data on health care workers’ occupational risk of colonization or infection with multidrug-resistant organisms (MDRO) and limited reporting on race and ethnicity.17 In a meta-analysis on occupational infection risk due to MDROs in health care workers that included 22 international studies, 4 of which were conducted in the United States, only 1 reported results by participants’ nationality.16
Health care workers in long-term care facilities, acute care, and intensive care units might be especially at risk. These settings have been found to carry MDROs like multidrug-resistant Candida auris, which has become a global threat and is often transmitted nosocomially.18 MDROs like carbapenem-resistant Enterobacterales are highly prevalent among residents of long-term care facilities due to the acuity of their medical conditions, frequent antibiotic exposures, and use of gastrointestinal devices and indwelling catheters; moreover, residents tend to harbor these organisms for extended periods of time, which increases risk of transmission.19,20 Barriers to consistent infection control measure implementation in long-term care facilities were unmasked by the COVID-19 pandemic. In addition to shortages in personal protective equipment and staff, lack of organizational communication and teamwork have been highlighted as underlying causes.21
Health care workers without advanced degrees often do not receive the same level of AMR education and training.
Another category of health care workers who might be more impacted by AMR are those providing care in low-resource settings, such as rural areas or low-income neighborhoods. These settings often have limited financial resources and may have shortages of personal protective equipment.22 Furthermore, due to staff shortages, rural health care staff are more likely than their urban counterparts to have multiple job responsibilities in addition to direct patient care, which might include infection control and AMR education.23
Adequate knowledge of AMR and AMR prevention is essential to combat the threat of resistance. Health care workers who have not received advanced degrees in medicine, such as nursing aides or transport staff, often do not receive the same level of AMR education and training. In the United States, health care workers in nursing homes have reported lack of knowledge, training, and continued medical education opportunities as key barriers to effectively implementing infection control measures.24 Nursing home staff who lack advanced medical degrees have also reported less frequent training and orientation on infection control measures than their medically trained counterparts.25 For example, a multicenter study conducted in the French health care system that evaluated the knowledge and attitudes of health care workers regarding MDROs found that those who lacked advanced medical degrees (eg, nursing assistants) scored significantly lower on knowledge of AMR and infection control measures than health care workers with advanced medical degrees (eg, physicians).26 Educational interventions targeted to different staff members, such as environmental services members, have been shown to be effective in improving overall knowledge of risk of pathogen transmission and necessary cleaning practices in addition to preventing the transmission of MDRO.27,28 Moreover, workers’ compliance with infection control measures has been found to be influenced by their knowledge of infection control practices and modes of MDRO transmission.25,29
Education on AMR and safe antibiotic use for health care workers who lack advanced medical degrees could have added benefits for certain minority communities. Low-income and Latinx communities commonly report self-medication with nonprescription antibiotics, the use of “left-over” antibiotics, and the purchase of foreign-made products, all of which could exacerbate the risk of AMR.30,31,32 Providing health care workers with education on AMR not only would improve adherence to infection control measures but also could lead to dissemination of this knowledge to their communities. However, it is important to acknowledge that the drivers of antibiotic misuse are complex and therefore may not be mitigated solely by improved knowledge about antibiotic resistance.
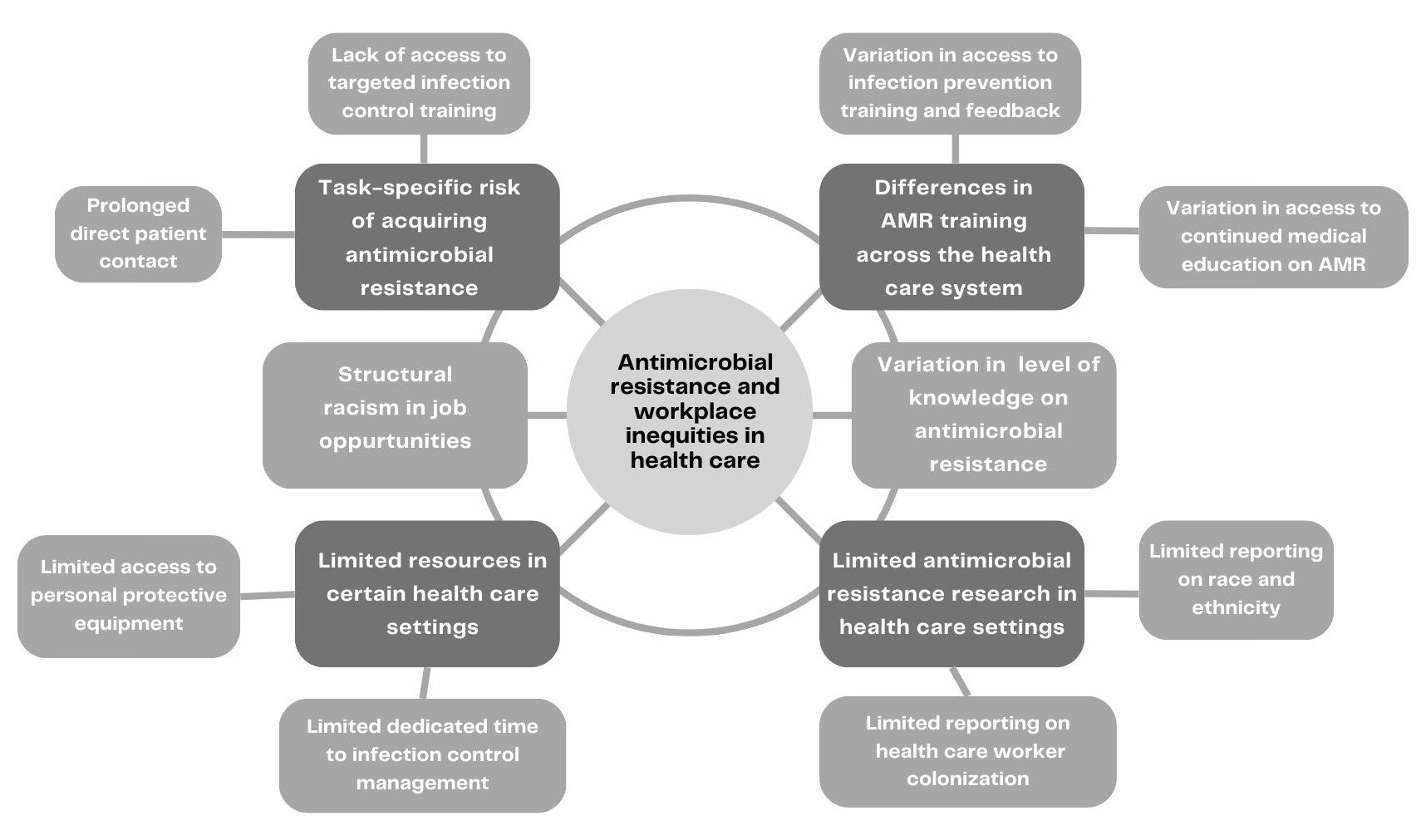
As health care workers and scientists, all of us have a responsibility to prioritize understanding the impact of health care workplace inequities and to acknowledge the intersectionality of workplace disparities, race, ethnicity, and AMR risk (see Figure). Currently, there is a clear gap in AMR research evaluating health care worker exposures and occupational risk. For instance, to our knowledge, there are no large longitudinal or multicenter US studies evaluating health care workers’ occupational risks of exposure to MDROs. Future research should include tracking and surveillance of MDROs among health care workers across the spectrum of health care settings to identify populations at the greatest risk. In addition, the medical profession needs to advocate for policies and practices for consistent data collection on race and ethnicity in AMR research on a national scale to better understand the impact of AMR on vulnerable communities and racial and ethnic minorities. With regard to institutional and policy changes, we recommend that health care institutions strive to provide equitable educational opportunities for all health care employees by using targeted AMR education and infection control training in order to promote effective infection prevention and responsible antibiotic use. Because nursing homes and long-term care facilities play a crucial role in providing essential health care services to communities and vulnerable populations, fostering partnerships with these facilities to establish opportunities for continued education on AMR and infection prevention is an important goal that will benefit minoritized health care workers as well.
Figure. Contributors to Antimicrobial Resistance and Heath Care Workplace Inequity
However, implementing new policies and expanding educational programs require funding support and allocation of resources to the most vulnerable sectors in health care. Expanding budgets dedicated to combating AMR requires action from health care systems and, on a larger scale, from governments. This manuscript calls for collaborative efforts among policy makers, employers, workers, and other stakeholders to safeguard workplace equity in the face of AMR.
US Department of Health and Human Services. Antibiotic Resistance Threats in the United States, 2019. Centers for Disease Control and Prevention; 2019. Accessed October 25, 2023. https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf
Ali F, Immergluck LC, Leong T, et al. A spatial analysis of health disparities associated with antibiotic resistant infections in children living in Atlanta (2002-2010). EGEMS (Wash DC). 2019;7(1):50.
Casey JA, Rudolph KE, Robinson SC, et al. Sociodemographic inequalities in urinary tract infection in 2 large California health systems. Open Forum Infect Dis. 2021;8(6):ofab276.
About the American Community Survey. US Census Bureau. June 27, 2023. Acessed October 25, 2023. https://www.census.gov/programs-surveys/acs/about.html
Adler A, Baraniak A, Izdebski R, et al; MOSAR team. A multinational study of colonization with extended spectrum β-lactamase-producing Enterobacteriaceae in healthcare personnel and family members of carrier patients hospitalized in rehabilitation centres. Clin Microbiol Infect. 2014;20(8)O516-O523.
Peters C, Dulon M, Nienhaus A, Schablon A. Occupational infection risk with multidrug-resistant organisms in health personnel—a systematic review. Int J Environ Res Public Health. 2019;16(11):1983.
Chen HY, Jean SS, Lee YL, et al. Carbapenem-resistant Enterobacterales in long-term care facilities: a global and narrative review. Front Cell Infect Microbiol. 2021;11:601968.
Stevenson KB, Searle K, Curry G, et al. Infection control interventions in small rural hospitals with limited resources: results of a cluster-randomized feasibility trial. Antimicrob Resist Infect Control. 2014;3(1):10.
Vaillant L, Birgand G, Esposito-Farese M, et al; PerceptR Study Group. Awareness among French healthcare workers of the transmission of multidrug resistant organisms: a large cross-sectional survey. Antimicrob Resist Infect Control. 2019;8(1):173.
Magiorakos AP. Systematic review of the effectiveness of infection control measures to prevent the transmission of carbapenemase-producing Enterobacteriaceae through cross-border transfer of patients. European Centre for Disease Prevention and Control; 2014. Accessed October 25, 2023. https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/CPE-systematic-review-effectiveness-infection-control-measures-to-prevent-transmission-2014.pdf
McCracken CM, Tucker KJ, Tallman GB, Holmer HK, Noble BN, McGregor JC. General perceptions and knowledge of antibiotic resistance and antibiotic use behavior: a cross-sectional survey of US adults. Antibiotics (Basel). 2023;12(4):672.