Medicine and Society
May 2024
Peer-Reviewed

Antimicrobial resistance is a global threat that inequitably affects minoritized populations, including Black, Latinx, and Indigenous people—especially in carceral settings—and is largely driven by inappropriate antimicrobial prescribing practices. People whose identities are minoritized are more likely to be incarcerated, and people who are incarcerated experience higher disease risk than people who are not incarcerated. This article draws on a case of dental infection suffered by a woman who is incarcerated to consider key ethical and clinical complexities of antimicrobial prescribing in carceral settings.
Antimicrobial-resistant (AMR) infections are an increasingly common cause of hospitalization and death, but programs preventing the development of antimicrobial resistance are incompletely implemented in low-resource health care settings.1 Examples of such settings include carceral settings like jails and prisons, which have focused for several years on improving infection control for respiratory, viral, bloodborne, and foodborne pathogens through isolation, quarantine, and testing protocols,2 but have devoted considerably less attention to preventing the emergence and decreasing the spread of AMR pathogens.
Given the intersection of poverty, mental illness, trauma, and racism, infectious disease epidemics and pandemics disproportionately take root in carceral settings where residents are already at increased risk for negative health outcomes. In one study of probationers and people recently released from prison in Connecticut, Black individuals reported a greater number of impacts of incarceration on their well-being than White individuals.3 The emergence of methicillin-resistant Staphylococcus aureus (MRSA) is a clear example of the impacts of incarceration on the dissemination of AMR pathogens in minoritized communities. The first outbreak of MRSA was reported in 1968 at Boston City Hospital4—a safety-net hospital renowned for providing care to financially disadvantaged persons in the greater Boston area—and outbreaks of MRSA infection and MRSA colonization were reported nationally in carceral settings in the early 2000s.5 As a result, incarceration is viewed as a well-recognized risk factor for MRSA infection.5,6,7,8,9,10,11
Antimicrobial stewardship programs (ASPs) are evidence-based interventions designed to optimize antimicrobial usage and to decrease the emergence of new AMR pathogens while reducing harm caused by unnecessary antimicrobial use and improving patient outcomes.12,13,14 The US Federal Bureau of Prisons, a system of 121 prisons housing about 200 000 people, developed and implemented an ASP program that led to a 26% decrease in antimicrobial use from fiscal year 2010 to fiscal year 2015.15 Outside of this publication—and despite a federal rule requiring US hospitals that participate in Medicare or Medicaid to implement ASPs16—we know of no other published reports of jail, state prison, or federal efforts to implement ASP programs. Most of the 1.8 million individuals who are incarcerated in the United States17 do not have stewardship programming to protect them against antimicrobial resistance.
Previous work by the fourth author (C.Y.) and colleagues has explicitly discussed the intersectionality of ethics and antimicrobial stewardship.18 The goal of this paper is to utilize Beauchamp and Childress’ 4 principles to assess ethical issues that arise in connection with stewardship of antibiotics in carceral settings. The 4 principles are (1) autonomy (having the ability to make one’s own decisions independently of external control), (2) nonmaleficence (avoiding harm), (3) beneficence (conferring benefit to the patient), and (4) justice (making choices that focus on fair distribution to maximize the welfare of society). In particular, we want to reflect on the complexities of the term justice, especially in discussions of ethics and carceral health.
To illustrate both the strengths and the limitations of the 4 principles framework, we will utilize a hypothetical patient scenario.
Case. Cynthia is a 45-year-old Black woman detained (pretrial) in jail who has faced barriers to routine dental cleanings and has a painful tooth. After finding that the tooth pulp is exposed and the tooth is not salvageable, the dentist in jail recommends the removal of the tooth. Cynthia is concerned because her cellmate had her teeth pulled and reported that the dentist did not give her enough pain medications. Cynthia asks for antimicrobials to treat the infection. When asked about allergies, Cynthia says that her mother told her she had a rash to penicillin as a child. She receives 14 days of clindamycin, and the pain improves with antimicrobials but returns after antimicrobial completion. Cynthia continues to decline tooth extraction and asks for a prolonged course of antimicrobials. She hopes to be out on bail soon and plans to get the tooth pulled after release. After 2 months of antimicrobial treatment, the jail clinician is conflicted as to whether to continue the antimicrobials.
Analysis. Dental infections are common in criminal-legal involved populations.19,20 A short course (less than 5 days) of antimicrobials is recommended when treating limited odontogenic infections, although there is variation in dental prescribing patterns.21 Dental extraction is widely accepted as the necessary procedure for a necrotic tooth, as it can be a nidus for extensive, life-threatening infection. This case brings up several important points.
First, the jail clinician wanted to respect Cynthia’s autonomy by honoring her request for antimicrobials instead of tooth extraction, but how autonomous is Cynthia? Based on Beauchamp and Childress’ analysis, competence in the form of insight and capacity are essential to autonomy. Cynthia’s explanation of why she is concerned about tooth extraction (and her request for antibiotics) demonstrates a reasonable understanding of her medical choices; she does not show any signs of incapacitated decision making; and her fears are consistent with those regularly expressed by patients experiencing incarceration in similar circumstances. Yet the oppression intrinsic to carceral systems is explicitly designed to limit autonomy and liberty, as evident in investigations of reproductive and transgender health injustices,22,23 the findings of which can be extrapolated to other health care scenarios, such as the case above. In this case, Cynthia faces oppression in several ways. She has limited power to advocate for pain medications to make a necessary tooth extraction more comfortable. The stigma of her incarcerated identity has resulted in limited access to otherwise commonplace health care interventions like penicillin allergy de-labeling for optimal medical treatment. Her pretrial detainment in jail and her history of being unable to access dental care suggest that she cannot afford bail and has limited financial resources, leaving her exposed to financial exploitation. If she is housed in a for-profit facility, her ongoing detainment pretrial may even be generating revenue for those who own the jail. These kinds of oppression mean that though Cynthia may have the competence to make her own medical decisions, her range of and access to available choices is profoundly limited, as is typical of other patients experiencing incarceration.23,24 As such, a jail clinician must acknowledge and accommodate the imperfect autonomy of a patient who is incarcerated. Shared decision making about treatment—and, in this case, the clinician’s agreeing to provide Cynthia with antibiotics even if to do so is not the evidence-based course of action—is a sign that the clinician recognizes patients’ limited autonomy. Prescribing antibiotics could thus foster greater trust.
Second, the benefits of honoring Cynthia’s autonomy do come with the potential to engender harm. The clinician wants to alleviate Cynthia’s suffering and to prevent further harm from delaying tooth extraction (eg, worsening abscess formation or further involvement of bone or other teeth) by administering antimicrobial therapy. But this option risks promoting Clostridioides difficile-associated colitis (a secondary infection precipitated by antimicrobial exposure), antibiotic-associated diarrhea, and other adverse effects, including the emergence of drug-resistant strains of pathogens. People who are incarcerated receive both hidden and direct messaging that treatment for the disease should be delayed until release.24,25
Oppression intrinsic to carceral systems is explicitly designed to limit autonomy and liberty.
Third, Cynthia’s report of a penicillin allergy highlights the harms faced by patients experiencing incarceration who have limited access to commonplace stewardship interventions such as penicillin allergy de-labeling that promote patient safety and optimize clinical care. Incorrectly reported penicillin allergies can lead to more expensive, less effective, and broader-spectrum antimicrobial prescriptions, and, as a result, penicillin de-labeling is a key component of ASPs, although there have been barriers to such programs’ equitable implementation.26,27,28 Those with penicillin allergies are also reported to have greater morbidity and mortality for a wide variety of infectious processes, including—but not limited to—bacterial pneumonia and bacteremia.29,30 To our knowledge, penicillin allergy de-labeling is not routinely offered in carceral settings; however, there are validated systems to determine if people are at high, medium, or low risk that can assist in the evaluation of a patient with a reported drug allergy.31
In addition to facing barriers to penicillin allergy de-labeling as part of robust ASP programs, patients who are incarcerated unjustly face limited resources to maximize their outcomes because of logistical barriers of de-labeling and limited quick-return financial incentives.32 One strategy in the community is a “watch-and-wait” approach to infections, wherein antimicrobials are prescribed but patients only take the medication if they get worse or antimicrobials are not prescribed but patients are encouraged to contact the clinician if they get worse. When we use a watch-and-wait approach in the community, we do so because there is relatively easy access for certain patients to health care. Patients who are incarcerated do not enjoy such access. Clinicians have limited hours, and most jails and prisons require a “sick slip” or written application for health care,33 which is then reviewed by a nurse and potentially triaged to clinicians for evaluation. This process can take a lot of time, which can increase the risk of worsening infection. If departments of health and infectious disease organizations hope to leverage de-labeling and a watch-and-wait approach to avoid antibiotic resistance development, these programs must not continue to overlook carceral systems, which may be target areas for such programs.
A fourth point is that prescribing medications in carceral settings represents a loaded interaction between patient and clinician. Even small interactions, like an antimicrobial prescription, can feel meaningful to someone who is incarcerated. People who are incarcerated may view the prescription as a token of trust and respect. Clinicians in the carceral setting may also see prescribing antimicrobials as a beneficent act of a compassionate physician-advocate that provides not simply medical help but emotional and psychological support to marginalized patients. In Cynthia’s case, the clinician may be reluctant not to prescribe antimicrobials because of concerns that the dental infection might worsen and there would be no system for rapid evaluation. Prescribing antimicrobials in a questionable case like this is a reflective harm reduction strategy, given the prolonged period it takes for people who are incarcerated to access health care. Withholding antimicrobials can be seen by patients as a reflection of unjust practices rooted in inequitable societal, medical, and carceral practices. Further complicating the patient-clinician dynamic, some clinicians may see antimicrobial prescribing as personal protection; carceral settings are often highly litigious environments, and so prescribing antimicrobials “just in case” often represents the practice of defensive medicine. While it is a noble desire to address patient concerns with the medical tools available, having too low a threshold for prescribing antimicrobials is very often more harmful than beneficial, even while it might feel like doing something is kinder than doing nothing.
As clinicians working at the intersection of antimicrobial stewardship and health equity—with a specific interest in serving as advocates for incarcerated populations within the United States—we, the authors, ask ourselves: “Is an unnecessary antimicrobial prescription the best way to practice our advocacy and push against injustice?” The core ethical principles are helpful for dissecting and identifying how ethical issues are embedded in daily clinical interactions between clinicians working in carceral settings and their patients (see Figure). To continue to ignore conversations about antimicrobial prescribing in carceral settings violates core ethical principles of health care delivery to a vulnerable population. ASPs are needed in carceral settings to provide a best-practices framework that can balance concerns about the development of antimicrobial resistance and ensuring the highest level of evidence-based antimicrobial prescribing and ensuring that both people who are incarcerated and clinicians working in carceral settings feel supported.
Figure. Applying Bioethical Principles to Antimicrobial Prescribing and Stewardship in Carceral Settings
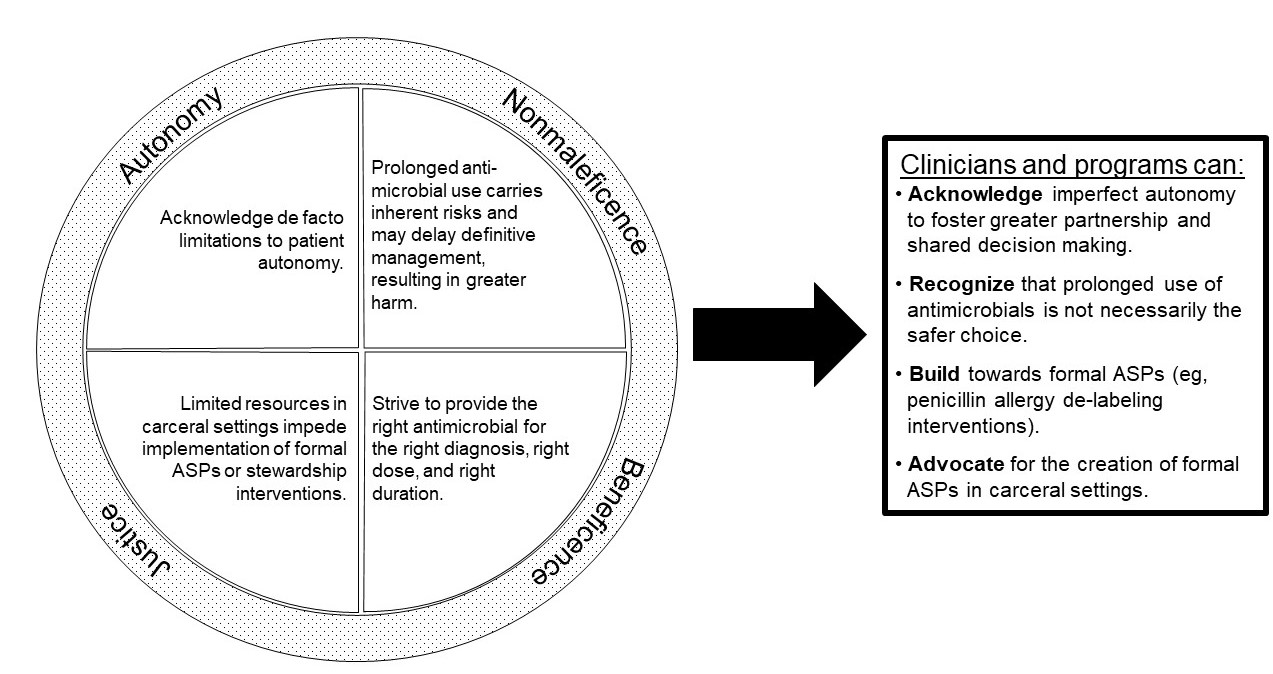
Abbreviation: ASPs, antimicrobial stewardship programs.
Lack of ASPs in jails and prisons is likely related to several intertwined factors. Health care services in carceral settings are under-resourced for increasingly complex chronic care patients whose cost of care is also rising. While individuals who are incarcerated are among the very few populations in the United States with a constitutionally guaranteed right to health care,34,35 there are no mandates for ASPs in carceral settings. Estelle v Gamble (1976)36 ruled that correctional settings that failed to provide people who are incarcerated with medical care “reasonably commensurate with modern medical science” was a violation of the Eighth Amendment and set the standard to prevent “deliberate indifference” to the harm caused by lack of provision of health care to people in jails and prisons. The prescription of unnecessary antibiotics with potential risks of side effects or multidrug-resistant infection, we believe, does not clearly qualify as “deliberate indifference.” Indeed, we maintain that these decisions are not indifferent to the patient’s goals and desires but deliberately working to address them. Yet the broader community, a group that does not have the same identified constitutional right to health care, may ultimately face the consequences of increasing antimicrobial resistance that stems from the health care challenges within carceral settings outlined above. Another reason for the lack of ASPs in carceral settings is that, without clear accreditation standards, carceral facilities do not have the same incentives as health care facilities to identify and prevent drug resistance. Moreover, political stakeholders may be unwilling to provide any investment in quality improvement in carceral health care facilities due to stigma against individuals with criminal-legal exposure, who are often stigmatized and marginalized in other ways due to mental health conditions, addiction, poverty, or being a person of color.
Critical next steps include cross-disciplinary participation in creating ASP programs in carceral settings. Stakeholders can include specialists in ASP implementation, carceral health care professionals, jail or prison administrators, and national health care accreditation organizations. As ASPs are implemented, it behooves the interdisciplinary team to proactively consider how such programs can help guide ethically challenging patient conversations in ways that ensure minimizing development of antimicrobial resistance while also ensuring that patients feel supported. Given the porous nature of jails and prisons, ASPs have the potential to decrease community transmission of AMR pathogens. They may also offer the potential to provide higher-quality, more cost-effective care to vulnerable patients, similar to ASP programs in other health care settings.37,38
Implementation of ASPs in jails and prisons, however, is a short-term solution to help improve the conditions of confinement. In parallel, we support legislative and policy reforms that seek to address and reverse the harms of incarceration. Preventing people from being incarcerated through improved access to housing, food, job opportunities, and mental health treatment without involving the carceral or judicial system should be the ultimate goal.
Implementing ASPs in carceral systems would be not only an impetus for greater equity and access to care in the carceral system, but also an act to fight the injustice of disproportionate harm to patients in carceral settings from inappropriate prescribing, to decrease the spread of AMR organisms, and to work around the dearth of advocates within carceral health care fighting for change. To best support patients like Cynthia, prevent community spread of resistant infections, and ensure high-quality care to a vulnerable population, ASP programs must go to jail.
National infection and death estimates for antimicrobial resistance. Centers for Disease Control and Prevention. Reviewed December 13, 2021. Accessed October 5, 2023. https://www.cdc.gov/drugresistance/national-estimates.html
Blankenship KM, Del Rio Gonzalez AM, Keene DE, Groves AK, Rosenberg AP. Mass incarceration, race inequality, and health: expanding concepts and assessing impacts on well-being. Soc Sci Med. 2018;215:45-52.
Popovich KJ, Thiede SN, Zawitz C, et al. Genomic analysis of community transmission networks for MRSA among females entering a large inner-city jail. Open Forum Infect Dis. 2022;9(3):ofac049.
National Center for Emerging and Zoonotic Infectious Diseases. Get smart for healthcare: know when antibiotics work. Centers for Disease Control and Prevention; 2010. Accessed October 5, 2023. https://www.cdc.gov/antibiotic-use/healthcare/pdfs/getsmart-healthcare.pdf
Core elements of antimicrobial stewardship. Centers for Disease Control and Prevention. Reviewed September 7, 2023. Accessed October 5, 2023. https://www.cdc.gov/antibiotic-use/core-elements/index.html
Medicare and Medicaid Programs; Regulatory Provisions to Promote Program Efficiency, Transparency, and Burden Reduction; Fire Safety Requirements for Certain Dialysis Facilities; Hospital and Critical Access Hospital (CAH) Changes to Promote Innovation, Flexibility, and Improvement in Patient Care; final rule. Fed Regist. 2019;84(189):51732-51834.
Kang-Brown J, Montagnet C, Heiss J. People in jail and prison in spring 2021. Vera. June 2021. Accessed November 20, 2023. https://www.vera.org/publications/people-in-jail-and-prison-in-spring-2021
Yen CF, Cutrell JB. Antimicrobial ethicists: making ethics explicit in antimicrobial stewardship. Antimicrob Steward Healthc Epidemiol. 2021;1(1):e17.
Maruschak LM; Office of Justice Programs. Bureau of Justice Statistics special report: medical problems of jail inmates. US Department of Justice; 2006. Accessed January 26, 2024. https://bjs.ojp.gov/content/pub/pdf/mpji.pdf
Cooper L, Stankiewicz N, Sneddon J, Smith A, Seaton RA. Optimum length of treatment with systemic antibiotics in adults with dental infections: a systematic review. Evid Based Dent. Published online September 7, 2022.
Turner NA, Moehring R, Sarubbi C, et al. Influence of reported penicillin allergy on mortality in MSSA bacteremia. Open Forum Infect Dis. 2018;5(3):ofy042.
Mabilat C, Gros M-F, Van Belkum A, et al. Improving antimicrobial stewardship with penicillin allergy testing: a review of current practices and unmet needs. Antimicrob Resist. 2022;4(6):dlac116.
Friedman E, Burr E, Sufrin C. Seeking recognition through carceral health care bureaucracy: analysis of medical care request forms in a county jail. Soc Sci Med. 2021;291:114485.
Estellle v Gamble, 429 US 97 (1976).



