State of the Art and Science
Feb 2007
Back pain costs our society $20 billion to $50 billion annually, afflicts 80 percent of the U.S. population in one form or another, and disables 1 percent completely [1,2].
Back pain can arise from any of the spinal structures, including the bone, muscle, ligaments, fascia, nerve roots and vessels [3]. The most common problems are musculoligamentous injuries or degenerative processes (disc herniation and osteoporotic fractures). But back pain can also result from spinal stenosis, infections, cancers and traumatic fractures and can be referred from visceral organs.
Unnecessary imaging leads to overdiagnosis and excessive expense [4,5]. In about 85 percent of cases, imaging reveals only nonspecific findings [6]. Judicious use of imaging can be of great value, however, in discovering the cause of pain. The choice of imaging technique should be guided by the patient's history and the physical examination. Critical to the diagnosis is the proper assessment of the type of pain experienced (e.g., is it local, referred, muscle spasm). In referred back pain, physical examination should include the rectum and palpation of visceral organs in the abdomen. Neurological and musculoskeletal examination can pinpoint specific nerve root lesions or muscle spasms [1]. Once a working diagnosis has been established based on the history and physical, the following imaging techniques can be used to confirm it or rule it out.
Radiography is useful for diagnosing skeletal lesions due to trauma, systemic disease or iatrogenic causes such as steroid use [3]. Radiographs (X-rays) can also give information about unstable or degenerating intervertebral discs by showing change in vertebral structure early in the disease [7]. Two orthogonal views are generally sufficient to characterize the nature and location of a lesion in bone, but soft tissue damage cannot be assessed [8]. Generally, X-ray is a good starting point and is best used as a screening test for misalignment or shape change of the vertebrae. The cause (osteoporotic fracture, tumor, infection, etc.) of such a finding may not be clear from the radiograph [9].
Computed tomography (CT) can take the place of more invasive imaging techniques such as myelography, epidural venography and epidurography [7]. It is more helpful than radiographs because of the fast acquisition times, high resolution, and 2-dimensional and 3-dimensional detail it provides, especially for complex vertebral fractures. It should be performed when radiography is inadequate [10]. CT is optimal for imaging of bony lesions and may catch problems that will be missed on traditional X-rays, which provide more limited views [1]. Imaging of soft tissue is better with CT than with radiography (although CT is inferior to MRI in this respect). CT may not distinguish symptomatic findings from incidental ones, however, leading to overdiagnosis. For example, herniated discs may show up on CT, but may not be the cause of pain [11]. CT subjects the patient to more radiation and is more expensive than a plain radiograph, but it gives more information than an X-ray and is a good alternative when MRI is contraindicated, as in the case of claustrophobic patients or those with pacemakers.
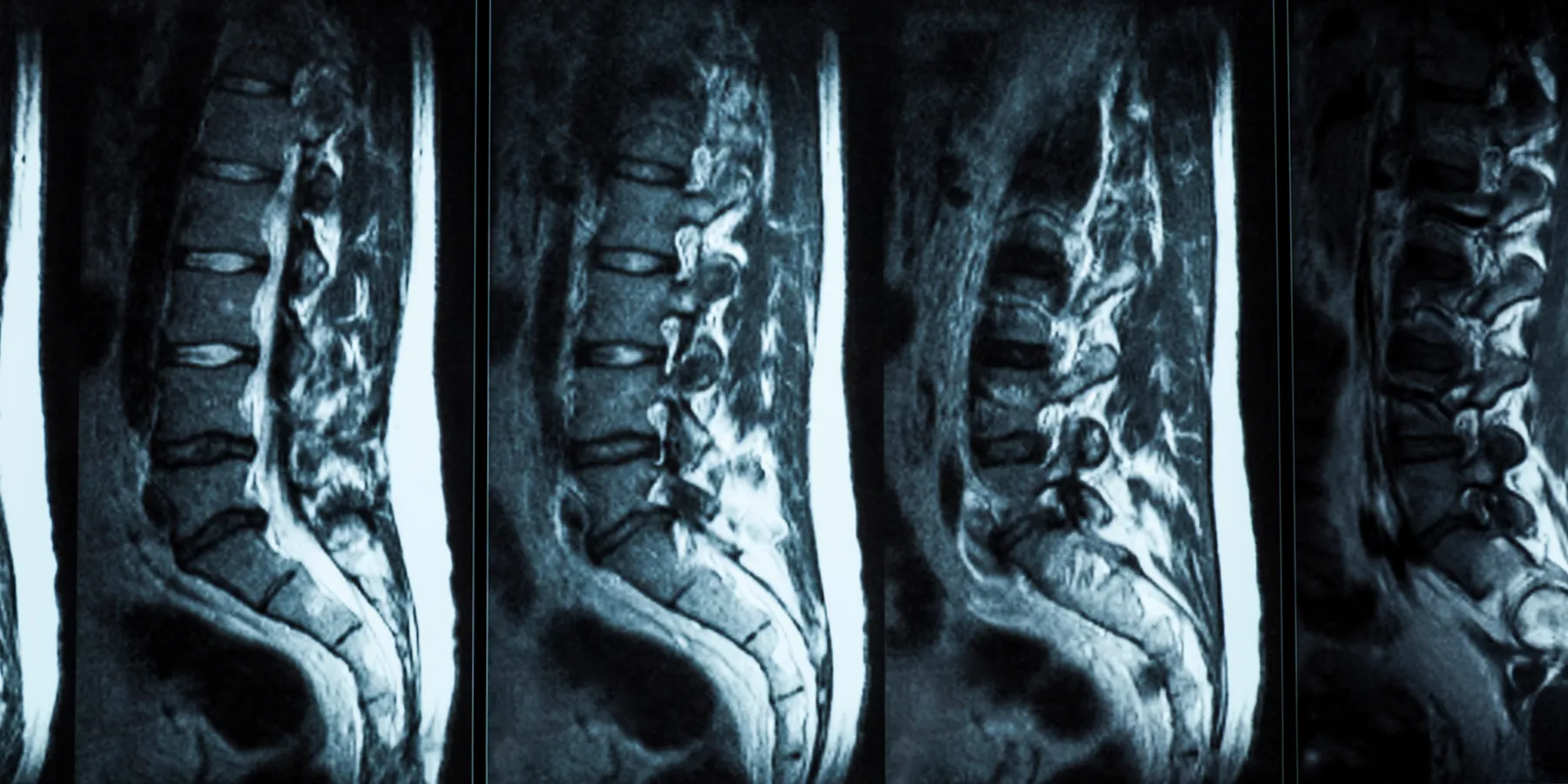
Magnetic resonance imaging (MRI) and CT myelography are comparable in diagnosing spinal stenosis or herniated discs. MRI may be somewhat more sensitive to and specific for herniated discs [10,12]. It is superior in detecting infections like osteomyelitis and bone or soft tissue tumors, in terms of both sensitivity and specificity [3,12]. It is also best for soft tissue imaging. In general, MRI is the best tool for diagnosing patients with lower back pain because it picks up a greater number of abnormalities than radiograph or CT [13]. MRI is the only imaging technique that allows direct visualization of the spinal cord and is therefore the best means for diagnosing congenital spinal lesions, myelopathies and metastatic cancers [10]. Because MRI does not use radiation, it is safer than X-ray and CT, but it is more expensive than they are, which may be a concern for some patients.
Ultrasound is noninvasive, inexpensive and able to image soft tissues. Moreover, there are no contraindications for ultrasound as there are for MRI. Ultrasound scans have been able to provide structural information about intervertebral discs that can be related to their pathology [14].This is not a common technique though, and while sensitivity in finding painful and degenerative discs is high, specificity is low [15]. More studies must be conducted to determine its value in diagnosing disc pathology. It is very helpful in determining whether pain may be due to visceral organs. For example, ovarian cysts are easily diagnosed this way and may be the cause of back pain.
Bone scans (skeletal scintigraphy) are informative in excluding tumor, fracture, metabolic or degenerative changes in the bone, necrosis or infection. Bone scans are more sensitive than radiographs and are able to determine various pathologies with high specificity by identifying areas of new bone growth or breakdown [16]. Positron emission tomography (PET) is also revealing, especially for finding cancers. While PET scans do not offer as much detail as CT or MRI, they can detect changes in metabolic activity and are highly sensitive for early detection of cancers that may be causing pain. It may even pick up on a cancer earlier than CT or MRI and therefore may be the best imaging option if cancer is suspected [12] . Nuclear scans expose the patient to about the same amount of radiation as a radiograph.
Excessive imaging is costly and ineffective. Therefore, the imaging modality should be chosen based on the patient's history and physical. Generally, the best imaging option for determining a cause for back pain is MRI. Other imaging modalities can be advantageous in the specific situations outlined above.
Engstrom JW. Back and neck pain. In: Kasper DL, Harrison TR. Harrison's Principles of Internal Medicine. 16th ed. New York, NY: McGraw-Hill Medical Publishing Division; 2005. Available at: http://www.accessmedicine.com/resourceTOC.aspx?resourceID=4. Accessed December 5, 2006.
Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344:363-370.
Ackerman SJ, Steinberg EP, Bryan RN, BenDebba M, Long DM. Trends in diagnostic imaging for low back pain: has MR imaging been a substitute or add-on? Radiology. 1997;203(2):533-538.
Hampton T. Back pain is a money drain. JAMA. 2004;291(4):415.
Carragee EJ. Clinical practice. Persistent low back pain. N Engl J Med. 2005;352:1891-1898.
Sonin AH, Boles CA, Rogers LF. The skeletal system: skeletal trauma. In: Grainger RG, Allison DJ, Adam A, Dixon AK, eds. Grainger and Allison's Diagnostic Radiology: A Textbook of Medical Imaging. 4th ed. London, New York: Churchill Livingstone; 2001. Accessed December 5, 2006.
Simmons ED, Guyer RD, Graham-Smith A, Herzog R, for the North American Spine Society. Radiograph assessment for patients with low back pain. Spine J. 2003;3(3 Suppl):3S-5S.
Haygood TM, Auringer ST. Muskuloskeletal Imaging. In: Chen MYM, Pope TL, Ott DJ, et al. Basic Radiology. New York, NY: McGraw-Hill Companies; 2004. Available at: http://www.accessmedicine.com/resourceTOC.aspx?resourceID=75. Accessed December 5, 2006.