Case and Commentary
Aug 2025
Peer-Reviewed

Most physicians do not see, or learn to see, nuclear war threat mitigation as within the scope of their professional duties. This commentary on a case argues there are 2 reasons why physicians, in particular, should draw on their unique training and expertise in medicine to help avert nuclear war: the risk of nuclear war and therefore the risk of catastrophic community, domestic, and global health consequences is presently high; and physicians today can draw on a strong history of past physicians’ nuclear disarmament advocacy strategies. This commentary concludes by canvassing how those past strategies can best be applied today.
A long-time advocate of nuclear weapons elimination, Dr A has spent their career listening to and caring for survivors of the 1945 atomic bomb strikes on Hiroshima and Nagasaki.
One of Dr A’s talking points is that a single nuclear warhead dropped on a city could kill or injure millions of people. With more than 12 000 nuclear weapons remaining in the arsenals of 9 nuclear-armed states,1 and with the understanding that even a “small-scale” nuclear war could have indirect effects that threaten billions with starvation,2 Dr A argues that all health professions have a responsibility to address this risk because they have fiduciary and ethical duties to both domestic and international communities. Dr A’s supporters add that nuclear war could cause societal collapse or human extinction, but detractors argue that such fears are overblown and rooted in ultimately unverifiable hypotheses.
Dr A and other members of International Physicians for the Prevention of Nuclear War (IPPNW) advocate that physicians are obliged to work to eliminate any morbidity and mortality risk, including that arising from nuclear weapons proliferation. Dr A and their colleagues wonder how to model positions and responses that other health professionals could also adopt and implement.
Physicians have long recognized that health and well-being depend not only on patient care provided in clinics and hospitals, but also on broader social conditions and public policy. Rudolf Virchow, the 19th-century German pathologist and parliamentarian, is often cited as an early advocate of this concept, having said that “[m]edicine is a social science, and politics is nothing but medicine on a large scale.”3,4 This awareness that policy and social factors influence health underpins the disciplines of public health, social medicine, and global health. However, the boundaries of physician action on public policy remain contested. For example, the National Rifle Association told physicians via social media to “stay in their lane” during public discourse on US gun violence in 2018.5 Physicians who treat gunshot wounds responded, “This is our lane.”5
In the mid-20th century, the medical community began addressing the global health threat of nuclear war through advocacy and education. While nuclear disarmament and abolition remain an interest for a small but active subset of physicians, there is a need for greater physician involvement in—and coalition building to support—nuclear disarmament. Dr A and their colleagues can advance this effort by emphasizing 2 key points to other health professionals. First, there is a significant precedent of physicians effectively addressing the threat of nuclear weapons.6 Second, the risk of nuclear war and its foreseeable consequences of mass casualties and a humanitarian crisis are greater now than at any point since the end of the Cold War.7,8,9,10 These 2 facts, Dr A should argue, confer upon health professionals an ethical obligation to promote patient well-being and safety by redoubling their efforts to abolish nuclear weapons.
Physicians managed the health effects of nuclear weapons even before the use of such weapons in war. In the Manhattan Project, the US government’s top-secret program to develop atomic bombs during the Second World War, physicians conducted research—sometimes unethical—on the health effects of plutonium.11 They also issued a warning to military officials before the first atomic weapon test, predicting that weather patterns would disperse radioactive material and harm American citizens.11,12 After the atomic bombings of Hiroshima and Nagasaki, Japanese health professionals provided direct patient care to survivors.13
After the Second World War, physicians continued to issue warnings of the health effects of nuclear testing. In 1957, the Nobel Prize-winning physician Albert Schweitzer published one such warning, his Declaration of Conscience, which swayed public opinion on nuclear weapons testing in the Western world.14 Antinuclear protests and polls showing negative attitudes toward nuclear weapons testing placed moral pressure on US President Dwight D. Eisenhower, who issued a cessation of nuclear testing in 1958, although it was resumed under President John F. Kennedy in 1962.14 Subsequent advocacy by the US organization Physicians for Social Responsibility (PSR) and the findings from the St Louis Baby Tooth Survey, which revealed excessive amounts of radioactive Strontium-90 in children’s teeth, played a role in President Kennedy’s decision to sign the Partial Nuclear Test Ban Treaty on behalf of the United States in 1963, which ended above-ground nuclear testing.15,16
Nevertheless, the number of nuclear warheads in the United States and Soviet arsenals continued to rise. To address this threat, American physician Bernard Lown, Soviet physician Yevgeniy Chazov, and several others founded the IPPNW in 1980.17 The IPPNW’s work earned it the Nobel Peace Prize in 1985.18 By promoting the movement for nuclear disarmament and engaging with policymakers, IPPNW physicians played a role in the development of the 1987 Intermediate-Range Nuclear Forces Treaty, which facilitated bilateral nuclear disarmament and helped usher in the end of the Cold War.6
In 2006, after disarmament progress had slowed, the IPPNW initiated the International Campaign to Abolish Nuclear Weapons (ICAN).19 ICAN went on to play an active role in negotiations on the Treaty on the Prohibition of Nuclear Weapons (TPNW), for which it received the Nobel Peace Prize after the treaty was adopted by the United Nations in 2017.19 One hundred twenty-two nations voted to pass the TPNW in the General Assembly.19 Since then, 94 nations have become signatories, and 73 have ratified the treaty, urging nuclear-armed nations to eliminate their nuclear weapons.20,21 However, much work remains, as none of the nuclear-armed states support the TPNW.20,21 Dr A can draw on this history to illustrate that physicians can effectively promote nuclear weapons policies that preserve human survival and prevent incurable suffering.
In January 2025, the Doomsday Clock of the Bulletin of the Atomic Scientists was set at the closest position to midnight in history, reflecting an unprecedented risk of nuclear war.7 Over 12 000 nuclear weapons exist today, some of which have 80-fold the explosive power of the bomb used in Hiroshima.22,23 Despite a long history of nuclear weapons accidents and false alarms,24 nuclear-armed states are pursuing campaigns to enhance and modernize their nuclear weapons to improve lethality and efficiency.25 In 2023, $91.4 billion was spent globally on such efforts, which was $10.8 billion more than the previous year. The US alone was responsible for 56% of the $91.4 billion.26 The estimated cost of US nuclear weapons spending alone over the next 30 years is $1.5 trillion.27 However, there is uncertainty over US nuclear policy since January 2025; the oft-cited “Project 2025” supports investment in nuclear modernization, but there have been expressions of executive branch interest in “denuclearization” and reductions in nuclear weapons spending.28,29
To illustrate why nuclear risk reduction matters to physicians, Dr A can appeal to evidence of the health effects of the bombings of Hiroshima and Nagasaki, nuclear weapons testing, nuclear reactor disasters, and health care-associated radiation, as well as to climate modeling, which indicates that a nuclear war would be catastrophic. Immediate and long-term health effects of nuclear explosions—from thermal burns and radiation sickness to cancer—are well-documented.30 Nuclear attacks in Japan in 1945 resulted not only in the acute deaths of approximately 210 000 individuals, but in leukemia, heart disease, stroke, anxiety, posttraumatic stress disorder-like symptoms, and somatization symptoms among survivors.30,31,32,33 Psychological damage can extend to those living with threats of nuclear destruction and can manifest as anxiety and a sense of helplessness.34
Communities exposed to nuclear weapons testing in locations such as the Marshall Islands, the Zhanasemey District of Kazakhstan, and Xinjiang, China, have also experienced long-term adverse health outcomes, including an elevated incidence of thyroid cancer.35,36 These findings are consistent with the health effects among survivors of the Chernobyl accident.37 In addition to external radiation exposure, these events can cause internal irradiation through contaminated air, food, and water.38
In metropolitan and industrial areas, fires from nuclear blasts would drive smoke into the atmosphere, which would reduce sunlight, temperature, and ozone; diminished ozone, specifically, would increase ultraviolet radiation exposure and exacerbate the risk of cataracts and skin cancer.39,40 Models of nuclear war between India and Pakistan or the United States and Russia suggest that these climate alterations would be substantial, prolonged, and global, leading to a nuclear winter that threatens 2 to 5 billion people, respectively, with famine.2,41 Similar models predict mass species extinction, a tragedy that would also reduce the diversity of natural products available for drug discovery.42,43
Given the destructive capacity of nuclear weapons, nuclear war poses not only significant health risks but also the potential for societal collapse. The likelihood of outright human extinction from nuclear war is more debatable, as Dr A’s detractors indicate. It is indeed impossible to precisely predict the outcome of a full-scale nuclear war. In such discussions, Dr A should, first and foremost, emphasize that the health implications of nuclear weapons alone are more than enough to merit substantial efforts to prevent nuclear war by physicians. Dr A could add that nuclear war would compromise global trade, including pharmaceutical supply chains, medical technology equipment, and commodities.44,45 Combined with infrastructural damage to research centers, sanitation systems, and governmental social services, these factors would cause further negative downstream health effects of nuclear weapons use.44,45 In the face of such disruptions, humanity’s vulnerability to other hazards, such as pandemics or natural disasters, would also increase, thereby increasing the risk of human extinction.
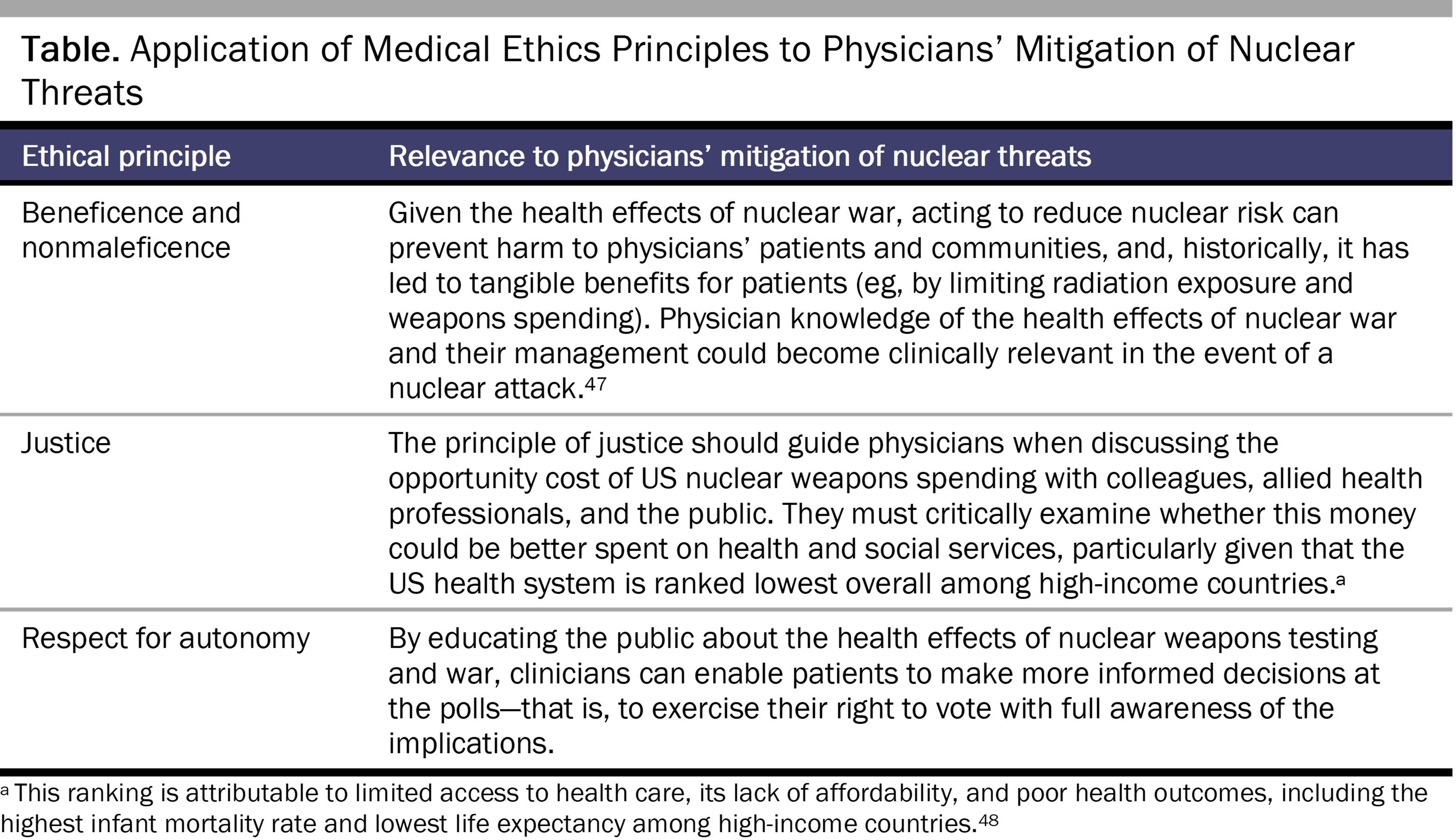
Dr A could call upon the 4 foundational principles of medical ethics—beneficence, nonmaleficence, justice, and autonomy—to emphasize the role of physicians in discussions about the nuclear threat (see Table).46
Efforts to address nuclear weapons by physicians may be viewed as supererogatory (ie, as an additional, but not necessary, moral obligation that goes “above the call of duty”), in which case physician autonomy to not engage in such advocacy is warranted.49 However, taking this view could not only endanger public safety, but potentially lead to shaming physicians who disagree about the need to address the nuclear threat. A case can be made that using moral shame or stigmatization to protect millions or billions of lives, given the catastrophic nature of nuclear weapons, is worthwhile.50,51 Indeed, it is not unusual for physicians who minimize or neglect the risks posed by other global health issues that broadly apply to all medical specialties, such as pandemics, to be morally shamed by other members of the health profession. While respectful debate about public health measures is important, it is critical to build a medical consensus and norm that nuclear weapons are an unacceptable threat to public health that must be “cured.”
By appealing to the history of physician activism and the predictable health risks of nuclear war, Dr A and their colleagues could help reorient physicians and other health professionals to nuclear weapons as a public health threat. It is time for every health professional to treat nuclear war as a tangible, imminent threat, just as we do pandemics, climate change, and natural disasters. How can we address the threat of nuclear war? We suggest that physicians can take the following actions.
First, physicians can urge their congressional representatives to support legislation that reduces the risk posed by nuclear weapons. Several bills under consideration propose additional funding for research on the health effects of nuclear weapons52,53 or encourage a “no first use” nuclear weapons policy (ie, a commitment not to initiate a nuclear attack) by the US government.54,55 Additional proposals include formal US recognition of the TPNW and reductions in spending on nuclear weapons.56,57
It is time for every health professional to treat nuclear war as a tangible, imminent threat, just as we do pandemics, climate change, and natural disasters.
Second, they can oppose bills that increase the risk of nuclear war, such as the Sentinel Nuclear Deterrence Act of 2023, which calls for additional nuclear modernization in the name of deterrence.58
Third, physicians can join grassroots social movements such as IPPNW, PSR, and Back from the Brink. These campaigns advocate for several actionable policies: (a) an end to presidential sole authority to launch nuclear weapons, (b) the adoption of an unconditional nuclear “no first use” policy, (c) the removal of intercontinental ballistic missiles from high alert status, (d) a funding reduction for nuclear weapons, and (e) the initiation of negotiations for a multilateral, verifiable, and time-bound agreement to abolish nuclear weapons.59
Fourth, physicians can call on institutions and other health care professionals to support social movements and policies that reduce nuclear risk. Specifically, physicians-in-training could engage the profession through advocacy and research.60 Those in allied health professions could take similar actions at their respective institutions. Ideally, this work would happen cooperatively with military leaders, either retired or in their civilian capacities, and academics, given that these professionals are perceived as highly trusted sources of information about nuclear weapons.61
Fifth, physicians can raise awareness of the opportunity cost of US nuclear weapons spending among colleagues, other health care professionals, and the American public by organizing or participating in town hall meetings and discussions focused on health care funding. Physicians can also leverage social media platforms to spread information and engage a broader audience.
Sixth, physicians can communicate with the American public and promote informed voting, as many citizens do not understand nuclear policy or its financial costs. Only 30% and 20% of the US public are somewhat familiar with US nuclear weapons policy and the cost of nuclear weapons, respectively.61 However, 60% of the public is “at least somewhat interested” in learning more about these topics, suggesting opportunities for advocacy and education.61
Although the potential benefits for public health are clear, physician advocacy to reduce nuclear risk may take time away from clinical care, self-care, and research.62 Coalition building through conference attendance, lobbying sessions, and campaign events may require travel and transportation expenses, although video conferencing can help mitigate some logistical and financial challenges to collaborating with colleagues in distant locations. Moreover, mentoring the next generation of physicians on nuclear issues demands the attention and effort of current thought leaders.
Physicians in academic centers may struggle to secure financial support for the time they dedicate to nuclear advocacy, as this type of work is not compensated63 or traditionally funded by research grants. While other grant-making organizations related to nuclear risk exist and might be avenues for funding,64,65,66 physician-advocates seeking funding must carefully consider issues such as bias, transparency, and conflicts of interest. With some creativity, advocates could design scholarly projects to advance knowledge about the dangers of nuclear weapons and grow the evidence base for relevant advocacy approaches. An ideal solution might be to seek endowments to create new research centers or departments at medical schools dedicated to managing nuclear and other extinction threats, perhaps under the heading of a new medical specialty.67
While serving the greater good of humanity, nuclear weapons advocacy could introduce political tensions that challenge professional relationships or affect career advancement opportunities. In this regard, it is notable that our 6 proposed actions for reducing nuclear risk are designed with a representative democracy in mind (particularly, the United States); they may not be applicable to other nuclear-armed states with differing political systems and security priorities. While some of the strategies described are only applicable in liberal democracies, the diplomacy of physicians and scientists involved in IPPNW in the 1980s was effective in changing nuclear weapons policy in both the United States and the former Soviet Union.68 These physicians adapted their advocacy to the political context in which they operated, suggesting that such work is possible, if difficult, in authoritarian nuclear-armed states today. Further knowledge of non-democracies is needed to understand why nuclear weapons are favored under some regimes and how physicians might help advance nuclear disarmament or abolition under such regimes.69 Ultimately, effective global collaboration can be achieved through careful diplomatic efforts, as demonstrated by American and Soviet physicians’ work through IPPNW.
Dr Bernard Lown, a co-founder of IPPNW, once said: “We physicians who shepherd human life from birth to death have a moral imperative to resist with all our being the drift toward the brink.”70 We are, once again, at the brink of a preventable nuclear arms race.71 The threat of nuclear war today is real, historically high, and growing. Physicians take an oath to promote the health of their patients and communities. Reducing the risk of nuclear war is fulfilling that oath. Given their past effectiveness in helping prevent nuclear war, physicians must act now against one of the greatest threats, if not the greatest threat, to public health.
Which countries have nuclear weapons? International Campaign to Abolish Nuclear Weapons. Accessed March 15, 2025. https://www.icanw.org/nuclear_arsenals
Virchow R. Der Armenarzt. Med Reform. 1848;(18):126-127.
Wamsley L. After NRA mocks doctors, physicians reply: “this is our lane.” NPR. November 11, 2018. Accessed January 27, 2025. https://www.npr.org/2018/11/11/666762890/after-nra-mocks-doctors-physicians-reply-this-is-our-lane
Mecklin J, ed; Science and Security Board. Closer than ever: it is now 89 seconds to midnight. Bulletin of the Atomic Scientists. January 28, 2025. Accessed March 18, 2025. https://thebulletin.org/doomsday-clock/current-time/
Risk of nuclear weapons use higher than at any time since Cold War, disarmament affairs chief warns Security Council. United Nations. March 31, 2023. Accessed March 15, 2025. https://press.un.org/en/2023/sc15250.doc.htm
Andrus J. A new era in nuclear arms reduction. New York State Bar Association. February 3, 2025. Accessed March 16, 2025. https://nysba.org/a-new-era-in-nuclear-arms-reduction/
Remarks from UN Secretary-General António Guterres. Arms Control Association. June 7, 2024. Accessed March 16, 2025. https://www.armscontrol.org/2024AnnualMeeting/UNSG-Remarks
Blume LMM. Collateral damage: American civilian survivors of the 1945 Trinity test. Bulletin of the Atomic Scientists. July 17, 2023. Accessed January 27, 2025. https://thebulletin.org/premium/2023-07/collateral-damage-american-civilian-survivors-of-the-1945-trinity-test/
History. Physicians for Social Responsibility. Accessed January 27, 2025. https://psr.org/about/history/
International Physicians for the Prevention of Nuclear War. The Nobel Prize. Accessed March 15, 2025. https://www.nobelprize.org/prizes/peace/1985/physicians/facts/
The road to a world free of nuclear weapons. International Campaign to Abolish Nuclear Weapons. Accessed January 27, 2025. https://www.icanw.org/ican_history
IPPNW World Congresses. International Physicians for the Prevention of Nuclear War. Accessed January 27, 2025. https://www.ippnw.org/news/ippnw-world-congresses
TPNW signature and ratification status. International Campaign to Abolish Nuclear Weapons. Accessed January 27, 2025. https://www.icanw.org/signature_and_ratification_status
Stockholm International Peace Research Institute. SIPRI yearbook 2024: armaments, disarmament and international security summary. Stockholm International Peace Research Institute; 2024. Accessed January 27, 2025. https://www.sipri.org/sites/default/files/2024-06/yb24_summary_en_2_1.pdf
Walsh B. Understanding the true scale of a nuclear bomb. Axios. August 5, 2020. Accessed January 27, 2025. https://www.axios.com/2020/08/05/beirut-nuclear-bomb-lebanon
Union of Concerned Scientists. Close calls with nuclear weapons. Union of Concerned Scientists; 2015. Accessed May 1, 2025. https://www.ucs.org/sites/default/files/attach/2015/04/Close%2520Calls%2520with%2520Nuclear%2520Weapons.pdf
Sanders-Zakre A, Snyder S. Surge: 2023 global nuclear weapons spending. International Campaign to Abolish Nuclear Weapons; 2024. Accessed January 27, 2025. https://assets.nationbuilder.com/ican/pages/4079/attachments/original/1718371132/Spending_Report_2024_Singles_Digital.pdf?1718371132
Cameron D. US nuclear missile silos need modernizing, but fixes aren’t coming soon. Wall Street Journal. August 26, 2024. Accessed January 27, 2025. https://www.wsj.com/politics/national-security/u-s-nuclear-missile-silos-need-modernizing-but-fixes-arent-coming-soon-7985e1ba
Whisnant G, Mesa J. Donald Trump wants to “get rid” of nuclear weapons. Newsweek. March 6, 2025. Accessed March 16, 2025. https://www.newsweek.com/donald-trump-wants-get-rid-nuclear-weapons-2040867
Trump regains control over nuclear policy: what’s next? Arms Control Association blog. February 21, 2025. Accessed March 15, 2025. https://www.armscontrol.org/blog/2025-02-21/trump-regains-control-over-nuclear-policy-whats-next
Dyer J. Psychopathology of nuclear war. Bull R Coll Psychiatrists. 1986;10(10):281.
Becker C, Hill JT, Muratov S. Brighter than a million suns: contemporary health consequences of atomic testing in the Semipalatinsk nuclear polygon. University of Central Asia; 2022. Working paper 70.
Scientific Committee on the Effects of Atomic Radiation. Sources and Effects of Ionizing Radiation, Volume 2: Effects: Scientific Annexes C, D and E. United Nations; 2011. Accessed January 27, 2025. https://www.unscear.org/unscear/uploads/documents/unscear-reports/UNSCEAR_2008_Report_Vol.II.pdf
Jehn FU. Anthropocene under dark skies: the compounding effects of nuclear winter and overstepped planetary boundaries. In: Proceedings of the Stanford Existential Risks Conference. Stanford University; 2023:119-132. Accessed May 1, 2025. https://stacks.stanford.edu/file/zb109mz2513/Jehn_Anthropocene%20Under%20Dark%20Skies.pdf
Bardeen CG, Kinnison DE, Toon OB, et al. Extreme ozone loss following nuclear war results in enhanced surface ultraviolet radiation. J Geophys Res Atmos. 2021;126(18):e2021JD035079.
Diaz-Maurin F. Nowhere to hide: how a nuclear war would kill you—and almost everyone else. Bulletin of the Atomic Scientists. October 20, 2022. Accessed January 27, 2025. https://thebulletin.org/2022/10/nowhere-to-hide-how-a-nuclear-war-would-kill-you-and-almost-everyone-else/#top
Kaiho K. An animal crisis caused by pollution, deforestation, and warming in the late 21st century and exacerbation by nuclear war. Heliyon. 2023;9(4):e15221.
Cotterlaz P, Gaulier G, Sztulman A, Ünal D. Pioneering a new classification: a comprehensive study of healthcare products in global trade. Banque de France. September 19, 2024. Working paper series 963. Accessed January 27, 2025. https://www.banque-france.fr/en/publications-and-statistics/publications/pioneering-new-classification-comprehensive-study-healthcare-products-global-trade
Al-Ibraheem A, Moghrabi S, Abdlkadir A, et al. An overview of appropriate medical practice and preparedness in radiation emergency response. Cureus. 2024;16(6):e61627.
Kuehn BM. US health system ranks last among high-income countries. JAMA. 2021;326(11):999.
Heyd D. Supererogation. Cambridge University Press; 1982.
Strydom C. Stigmatisation as a road to denuclearisation—the stigmatising effect of the TPNW. In: Black-Branch JL, Fleck D, eds. Nuclear Disarmament and Security at Risk—Legal Challenges in a Shifting Nuclear World. Springer Nature; 2021:453-478. Nuclear Non-Proliferation in International Law; vol 6.
Health Impacts of Nuclear War Act of 2023, S 2398, 118th Cong (2023-2024). Accessed March 19, 2025. https://www.congress.gov/bill/118th-congress/senate-bill/2398/text
Health Impacts of Nuclear War Act of 2023, HR 4703, 118th Cong (2023-2024). Accessed March 19, 2025. https://www.congress.gov/bill/118th-congress/house-bill/4703/text
Restricting First Use of Nuclear Weapons Act of 2023, HR 669, 118th Cong (2023-2024). Accessed March 19, 2025. https://www.congress.gov/bill/118th-congress/house-bill/669/text
Restricting First Use of Nuclear Weapons Act of 2023, S 1186, 118th Cong (2023-2024). Accessed March 19, 2025. https://www.congress.gov/bill/118th-congress/senate-bill/1186/text
Embracing the Goals and Provisions of the Treaty on the Prohibition of Nuclear Weapons, HR 77, 118th Cong (2023-2024). Accessed March 19, 2025. https://www.congress.gov/bill/118th-congress/house-resolution/77/text
Nuclear Weapons Abolition and Conversion Act of 2023, HR 2775, 118th Cong (2023-2024). Accessed March 19, 2025. https://www.congress.gov/bill/118th-congress/house-bill/2775/text
Sentinel Nuclear Deterrence Act of 2023, S 2017, 118th Cong (2023-2024). Accessed March 19, 2025. https://www.congress.gov/bill/118th-congress/senate-bill/2017/text
Our five policy solutions. Back from the Brink. Accessed January 27, 2025. https://preventnuclearwar.org/our-five-policy-solutions/
Smeltz D, Kafura C, Weiner S. Majority in the US interested in boosting their nuclear knowledge. Lester Crown Center on US Foreign Policy; Carnegie Corporation of New York; Chicago Council on Foreign Affairs; 2023. Accessed March 18, 2025. https://media.carnegie.org/filer_public/f1/65/f1652f81-0d93-442e-9f77-37954dc505dc/majority_in_the_us_interested_in_boosting_their_nuclear_knowledge.pdf
Louisias M, Hicks R, Jacobs S, Foggs MB. The role of physician advocacy in achieving health equity: where is the allergist-immunologist? J Allergy Clin Immunol Pract. 2022;10(4):910-917.
International peace and security. Carnegie Corporation of New York. Accessed March 16, 2025. https://www.carnegie.org/programs/international-peace-and-security/
Global Catastrophic Risks Fund. Founders Pledge. Accessed March 16, 2025. https://www.founderspledge.com/funds/global-catastrophic-risks-fund
Grantmaking work. Future of Life Institute. Accessed March 16, 2025. https://futureoflife.org/our-work/grantmaking-work/
Kellis DM, Torres ÉP. Extinction medicine: the case for a new medical specialty. SSRN. March 25, 2025. Accessed May 8, 2025. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5109482
IPPNW: a brief history. International Physicians for the Prevention of Nuclear War. Accessed March 15, 2025. https://www.ippnw.org/about/ippnw-a-brief-history
Chazov Y. International Physicians for the Prevention of Nuclear War acceptance speech. The Nobel Prize. December 10, 1985. Accessed January 27, 2025. https://www.nobelprize.org/prizes/peace/1985/physicians/acceptance-speech/
Klare MT. The nuclear arms race is back and more terrifying than ever. The Nation. September 17, 2024. Accessed January 27, 2025. https://www.thenation.com/article/world/nuclear-war-new-start/



