Medicine and Society
Oct 2025
Peer-Reviewed
The Undiagnosed Diseases Network (UDN) exists at an intersection of diagnostic research and clinical care and has 2 main goals: to advance diagnostic science and to facilitate accurate diagnoses in individual patient-participants with rare conditions or so-called “medical mysteries.” The value of the UDN’s translational research and clinical application model and of the results it produces derive from whether and to what extent the UDN achieves its 2 goals. This article considers criteria currently used to assess achievement of those goals, identifies their merits and drawbacks, and offers strategies by which the UDN might further advance diagnostic science and individual patient-participants’ interests.
The Undiagnosed Diseases Network (UDN) has always been unique in its stated goals and approach to scientific inquiry. Conceived within the National Institutes of Health in 2008 in response to patient demand and expanded to a national clinical research network in 2013,1 the UDN describes its goal as “to both help individual patients and families living with the burden of undiagnosed diseases, and contribute to the understanding of how the human body works.”2 This focus drives the case-based approach utilized by the network, in which each individual patient receives a tailored evaluation based on the specific characteristics of their case, and scientific advancement comes from discoveries made through in-depth examination of each case.
Based on its stated goals, the UDN arguably offers an ideal model for ethical translational genomics research. The emphasis of the network on return of results speaks to a commitment to maximize benefits for research participants while simultaneously providing benefits to society in the form of generalizable knowledge gained for examination of rare disease manifestations. However, knowing the extent to which the UDN is achieving its goals—and maximizing its value—requires a critical examination of how the network evaluates its success. In this paper, we first examine the ways in which value has been measured within the UDN thus far. We then explore metrics that could be used to define and measure the value of the UDN. Finally, we suggest an alternative approach that would measure value both short- and long-term and discuss the implications of such an approach.
Metrics currently used to evaluate the UDN take multiple forms. The Table provides an overview of the types of metrics tracked and examples of each. The UDN Data Management and Coordinating Center (DMCC) tracks and publishes multiple metrics related to the application and evaluation process, the number of diagnoses identified, and scientific products, including manuscripts published and genetic variants and records shared in public databases.3
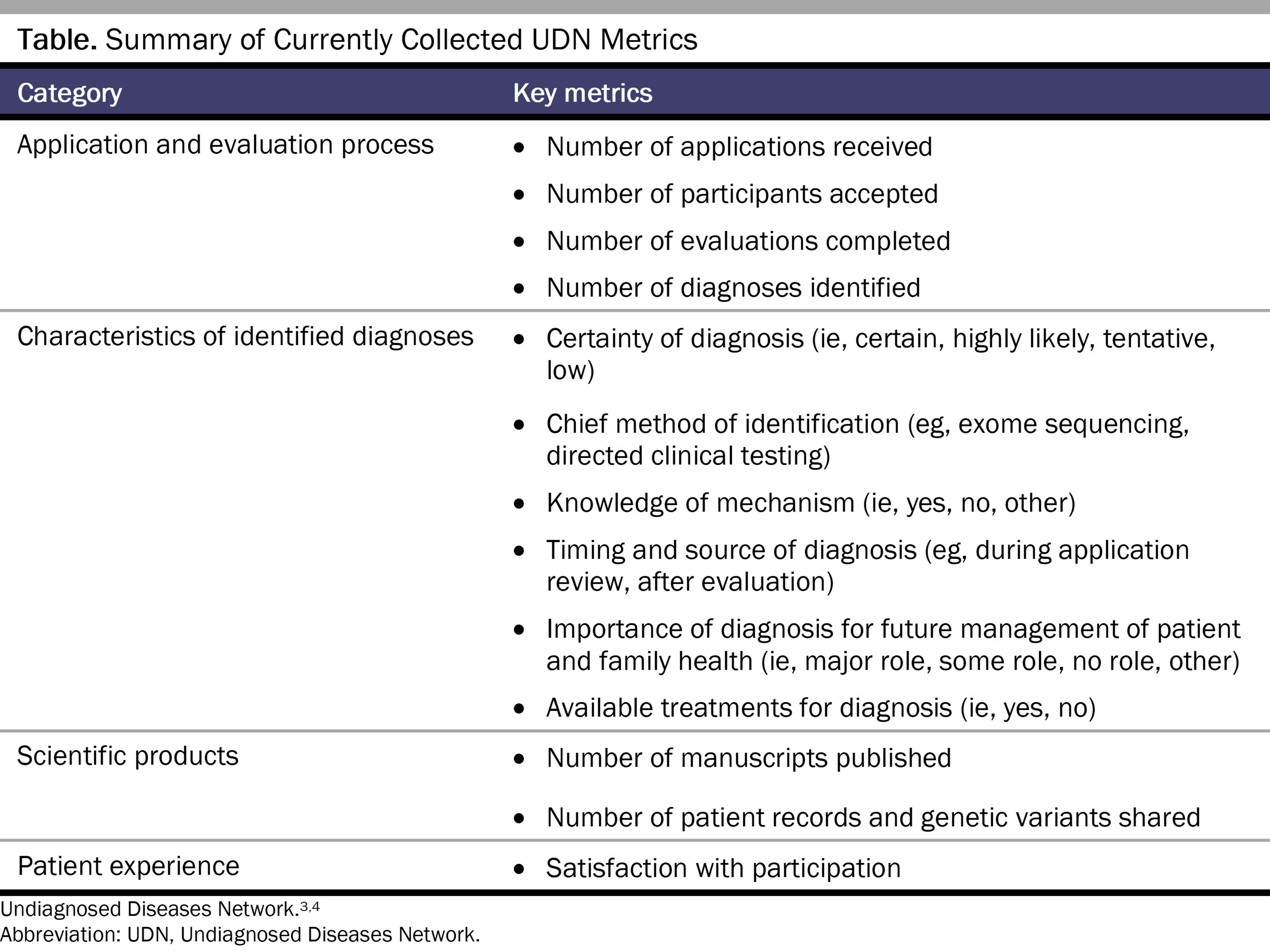
As described in its Manual of Operations, the lead clinical site also assesses specific characteristics of each diagnosis it identifies.4 This information is submitted to the internal, shared network database and was last reported for the network in a manuscript published in 2018.5 The DMCC also distributes follow-up surveys to participants after their UDN evaluation to assess their satisfaction with participation, although this information has not been published or shared publicly to our knowledge.4
Currently utilized metrics have some value in helping individual patients and families and advancing knowledge of the human body, while also leaving key gaps. The number of manuscripts published by the network—307 as of July 2, 2025—suggests the extent of UDN contributions to new knowledge about causes of rare diseases, particularly their genetic underpinnings.3Manuscripts published by the network also provide some additional insight into other relevant indicators of value, such as patients’ experiences of participation,6,7 parents’ perceived utility of diagnosis,8 and impact of diagnosis on parent or patient empowerment.9 However, these indicators are not systematically collected network-wide. The submission of 939 rare variants to ClinVar (a public database) and completed genome sequencing for 2078 participants as of July 2, 2025, have further contributed to the general knowledge base.3 Metrics such as the number of new disease genes or new disease mechanisms identified by the UDN indicate that the UDN’s contributions to science extend beyond those relevant just to participants in the UDN.
However, as with any scientific achievement, the true value of the knowledge gained is difficult to evaluate. Counting scientific manuscripts can provide insight into scientific productivity but does not speak to the quality of the information generated or its importance to individual patients or patient populations. Even if the journal in which a manuscript is published serves as a proxy for quality and importance, the true measure of the scientific value of health research could be thought of as the extent to which it ultimately changes clinical care and, ultimately, improves health outcomes. But even if the number of additional patients diagnosed outside the UDN increases as a result of this knowledge, the benefits of these diagnoses to the patients and families remain difficult to assess.
One way to understand the broader scientific value of the UDN could be through an examination of the value it provides to current participants. The number of diagnoses identified—886 as of April 1, 2025—certainly suggests the potential for direct benefit to patients and families.3 Furthermore, studies conducted both in collaboration with the UDN and by other research groups have documented many challenges associated with living with an undiagnosed disease, including excess morbidity, off-target treatments, invalidation by health care practitioners, social isolation, and serious mental health consequence, among others.10,11,12 Many of these challenges could be ameliorated by diagnosis.
However, the UDN does not systematically collect the data needed to assess whether the diagnoses it has provided have ameliorated any of these challenges. For one thing, it does not systematically collect information on health outcomes, and therefore it is unclear whether diagnoses have any impact on clinical outcomes for patients. Furthermore, while the network does collect limited information on the impact of diagnosis on parent or patient empowerment,4 it does not systematically collect patient-reported outcomes related to personal utility or health-related quality of life—despite the fact that families can derive various forms of intrinsic or instrumental (eg, reproductive decision-making) value from a diagnosis and that most rare diseases lack treatments.13 Beyond the post-evaluation surveys of participant satisfaction, it also is unclear whether the UDN is considering or actually measuring potential harms that might emerge from participation. Given the vulnerability of the participant population and its dependence on the research, there are risks of therapeutic—or diagnostic—misconception, which have been documented but are not currently systematically evaluated.6,14
Systematic evaluation of enrolled participants’ health outcomes and impacts of diagnosis (if received) on participant and family quality of life would increase the scientific value of the UDN by providing unique insight into the clinical and personal benefits of diagnosis for a wide range of rare diseases, particularly those that are ultra rare and lack therapies. While research has suggested the potential for significant personal utility of a rare disease diagnosis,8,15 this utility has not been systematically assessed in a large sample of ultra-rare diseases. Such analyses could also provide insights into potential mediators and moderators of benefit to guide testing recommendations and follow-up outside of the UDN. In addition, studies have only rarely examined the perceived benefits of diagnosis over time,16 and those that have done so suggest waning of perceived benefit.17 Collecting patient-reported measures of value among UDN participants at multiple time points could help to fill this key knowledge gap. In addition, collecting and comparing diagnosed and undiagnosed patients’ data on quality of life over time could provide insight into the extent to which diagnosis provides unique benefits to patients and families.
Maximizing the knowledge gained through the UDN is also consistent with the ethical practice of research. The risks participants take on through their participation, such as risks to privacy and financial risks of travel and time off work or school for assessment, are justified in part by the social value of the knowledge to be gained. Understanding the potential benefits and harms of participation from the perspectives of patients and families also is essential for ensuring true informed consent, as well as for understanding obligations to participants should UDN funding end. Current guidelines suggest that researchers have limited obligations to return results on genetic and genomic research to participants after studies end.18 However, this obligation is arguably greater, as UDN participants are unique in having almost invariably exhausted all diagnostic testing available in clinical care. The obligation to return results even after the study ends is contingent, at least in part, on the extent to which sharing the information would provide direct benefits to the patient and family.19 But without data on harms and benefits, we cannot effectively assess ethical obligations to participants enrolled in the UDN.
Clarifying how benefits and risks of UDN participation should be assessed is also central to determining the resources and infrastructure needed to maximize the UDN’s value to enrolled participants and to science. The current structure of the UDN focuses scientific inquiry on the individualized evaluation of each participant. While this structure was a logical beginning for a small program, reenvisioning the UDN as a multi-site, longitudinal cohort study could further maximize both its scientific value and the value to participants. Collection of clinical and patient-reported outcomes over time, at regular intervals, using systematic and consistent protocols across sites rather than collecting outcomes data solely at the time of evaluation using variable protocols could help fully characterize the benefits of participation for patients and families and fill key gaps in our current understanding of the value of genetic diagnoses for highly heterogenous rare diseases over time. This approach could also provide clearer evidence as to the value of the UDN evaluation itself not only for science and for the patients who are diagnosed, but also for those who remain undiagnosed, some of whom have reported benefits simply from participation.7,8 In addition, as tools for diagnostic evaluation evolve, a large cohort of rare and undiagnosed patients with well-characterized clinical, genomic, and patient-reported outcomes data could provide valuable data for evaluation of these new tools, further enhancing the value of the network to science. Finally, the UDN could follow the examples of other longitudinal cohort studies, such as the Framingham Heart Study or the Jackson Heart Study, in building lasting and collaborative, reciprocal relationships with participants and participant communities.
As a translational genomics study that seeks to both advance science and help patients and families, the UDN has the potential to provide unique insights regarding the value of diagnosis. However, the current criteria used to assess the UDN’s value in fact directly limit its value. Reenvisioning the UDN as a longitudinal cohort study that systematically collects clinical and patient-reported outcomes over time would ensure that the network can maximize its value to science, participants, and future patients.
Focus on the Undiagnosed Diseases Network. National Institute of Neurological Disorders and Stroke. Reviewed January 2, 2025. Accessed May 19, 2025. https://www.ninds.nih.gov/current-research/focus-disorders/focus-undiagnosed-diseases-network
About us. Undiagnosed Diseases Network. Accessed May 28, 2025. https://undiagnosed.hms.harvard.edu/about-us/
Facts and figures. Undiagnosed Diseases Network. Updated July 2, 2025. Accessed August 11, 2025. https://undiagnosed.hms.harvard.edu/about-us/facts-and-figures/
Undiagnosed Diseases Network. Undiagnosed Diseases Network Manual of Operations. Undiagnosed Diseases Network; 2025. Accessed April 8, 2025. https://undiagnosed.hms.harvard.edu/wp-content/uploads/2025/03/UDN-Manual-of-Operations_February-2025.pdf
Splinter K, Adams DR, Bacino CA, et al; Undiagnosed Diseases Network. Effect of genetic diagnosis on patients with previously undiagnosed disease. N Engl J Med. 2018;379(22):2131-2139.
Halley MC, Young JL, Tang C, et al; Undiagnosed Diseases Network. Genomics research with undiagnosed children: ethical challenges at the boundaries of research and clinical care. J Pediatr. 2023;261:113537.
Rosenfeld LE, LeBlanc K, Nagy A, Ego BK, McCray AT; Undiagnosed Diseases Network. Participation in a national diagnostic research study: assessing the patient experience. Orphanet J Rare Dis. 2023;18(1):73.
Halley MC, Young JL, Fernandez L, et al; Undiagnosed Diseases Network. Perceived utility and disutility of genomic sequencing for pediatric patients: perspectives from parents with diverse sociodemographic characteristics. Am J Med Genet A. 2022;188(4):1088-1101.
McConkie-Rosell A, Schoch K, Sullivan J, et al; Undiagnosed Diseases Network. The genome empowerment scale: an assessment of parental empowerment in families with undiagnosed disease. Clin Genet. 2019;96(6):521-531.
Rao A, Yabumoto M, Ward-Lev E, Miller EG, Naik H, Halley MC. Health-related quality of life in patients with diverse rare diseases: an online survey. Genet Med Open. 2024;2:101889.
Spillmann RC, McConkie-Rosell A, Pena L, et al; Undiagnosed Diseases Network. A window into living with an undiagnosed disease: illness narratives from the Undiagnosed Diseases Network. Orphanet J Rare Dis. 2017;12(1):71.
McConkie-Rosell A, Hooper SR, Pena LDM, et al; Undiagnosed Diseases Network. Psychosocial profiles of parents of children with undiagnosed diseases: managing well or just managing? J Genet Couns. 2018;27(4):935-946.
Dicken JE, Copeland R, Anderson KJ, et al. Rare Diseases: Although Limited, Available Evidence Suggests Medical and Other Costs Can Be Substantial. US Government Accountability Office; 2021. GAO-22-104235. Accessed October 23, 2021. https://www.gao.gov/assets/gao-22-104235.pdf
Miller EG, Young JL, Rao A, Ward-Lev E, Halley MC. Demographic characteristics associated with perceptions of personal utility in genetic and genomic testing: a systematic review. JAMA Netw Open. 2023;6(5):e2310367.
Marathe PN, Suckiel SA, Bonini KE, et al. Evaluating parental personal utility of pediatric genetic and genomic testing in a diverse, multilingual population. HGG Adv. 2024;5(3):100321.



