Case and Commentary
Nov 2025
Peer-Reviewed
Electronic health records are now critical in day-to-day health care operations. A drawback to using them, however, is that they tend to divert clinicians’ focus from patients to a screen. This phenomenon has generated a colloquial reference to patient-screen pairings as an “iPatient.” This commentary on a case suggests key points of ethical and clinical relevance about this trend in patient-clinician relationships and clinical encounters.
ML works in a busy, academically affiliated community clinic with daily pressure to sign patients’ charts promptly after encounters with patients. ML has always enjoyed interacting with patients, students, and trainees, but pressure to sign charts by a busy day’s end makes ML feel mechanized and that their ability to connect with students, trainees, and especially patients during visits is compromised due to the need to shorten visits to make time for demands of prompt chart review and sign-off.
Clinic administration has incentivized ML’s and other clinicians’ “efficient” chart completion with bonuses, which feels infantilizing and exacerbates ML’s feelings of being valued by their organization for perfunctory complacency and compliance.
ML and their colleagues consider how to respond to this trend.
Early goals of integrating the electronic health record (EHR) into health systems practice and performance included supporting patients and aiding clinicians’ decision-making. Since their introduction, EHRs have expanded their functions significantly, incorporating billing, prescribing, and providing virtual care, all of which shape the current landscape of clinical care.1 However, EHRs’ pervasiveness also means that more time and focus are dedicated to the EHR itself as a means of focusing on patients during clinical encounters. This commentary on a case suggests key points of ethical and clinical relevance about this trend in patient-clinician relationships and clinical encounters.
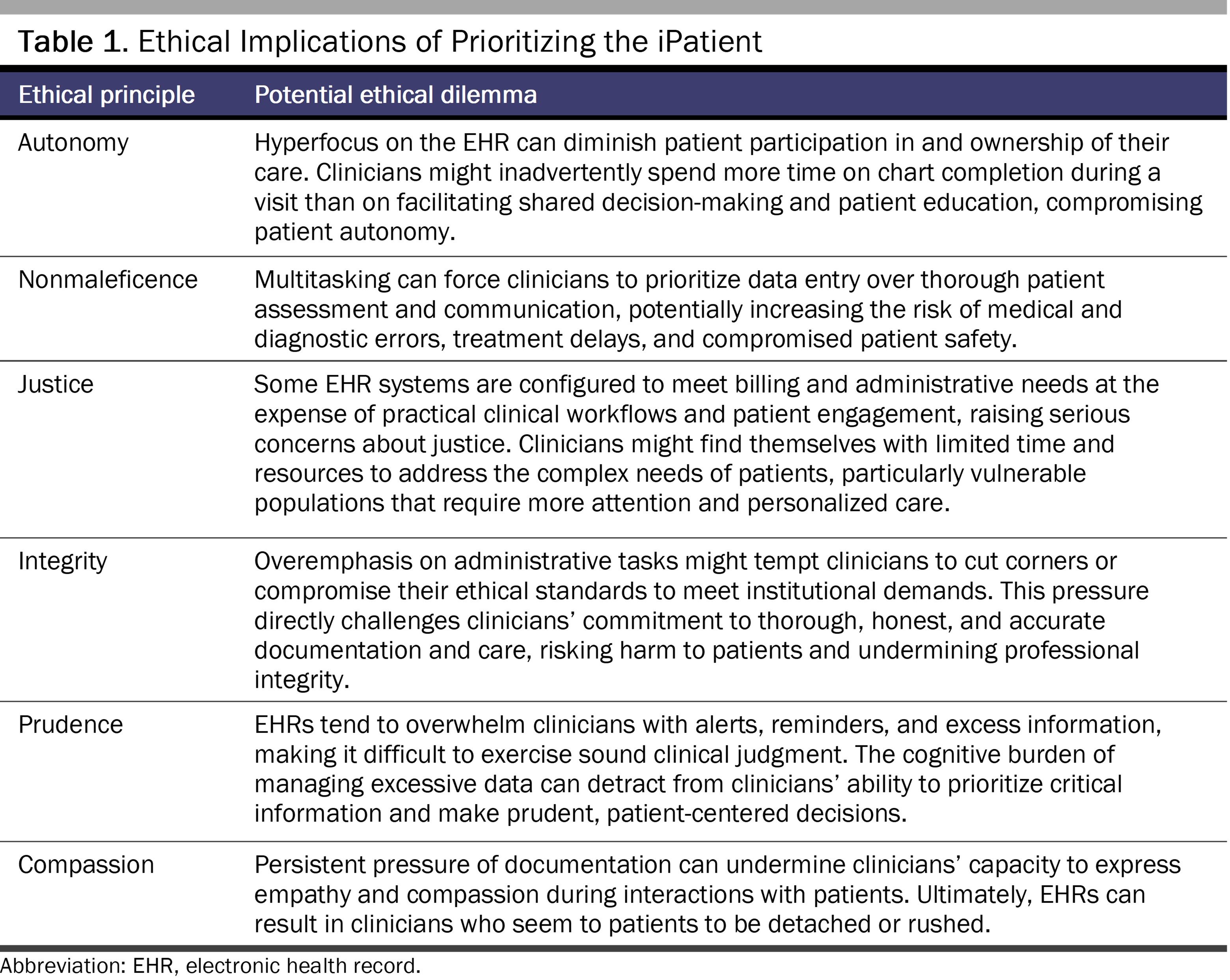
Digital consolidation of patient-specific health records has offered some benefits to patients, clinicians, and health care systems that should be acknowledged. EHRs are easily accessible and highly informative. Yet these records are so extensive and attended to that Abraham Verghese has described them as constituting an “iPatient,” an electronic representation and digital shadow of the actual living, feeling, and sometimes neglected real patient.2 In his words: “The iPatient is getting wonderful care all across America. The real patient often wonders, where is everyone? When are they going to come by and explain things to me? Who’s in charge? There’s a real disjunction between the patient’s perception and our own perceptions as clinicians of the best medical care.”3 Table 1 highlights the ethical implications of prioritizing the iPatient.
Given that there can be tangible human costs associated with prioritizing the iPatient, it is important that clinicians be aware of this possibility to avoid potential negative impacts. First, the sheer presence of exam room computers might also reduce the amount of interpersonal contact, as perceived by patients. Studies have noted that clinicians spend nearly 50% of an average clinic day in the EHR and only 27% in direct face time with patients.4,5,6 In a Harris Poll published in 2018, nearly 62% of primary care practitioners (PCPs) felt they had insufficient time to adequately address patient questions or concerns because of EHR time demands, and 69% felt that EHRs took valuable time away from patients.6,7
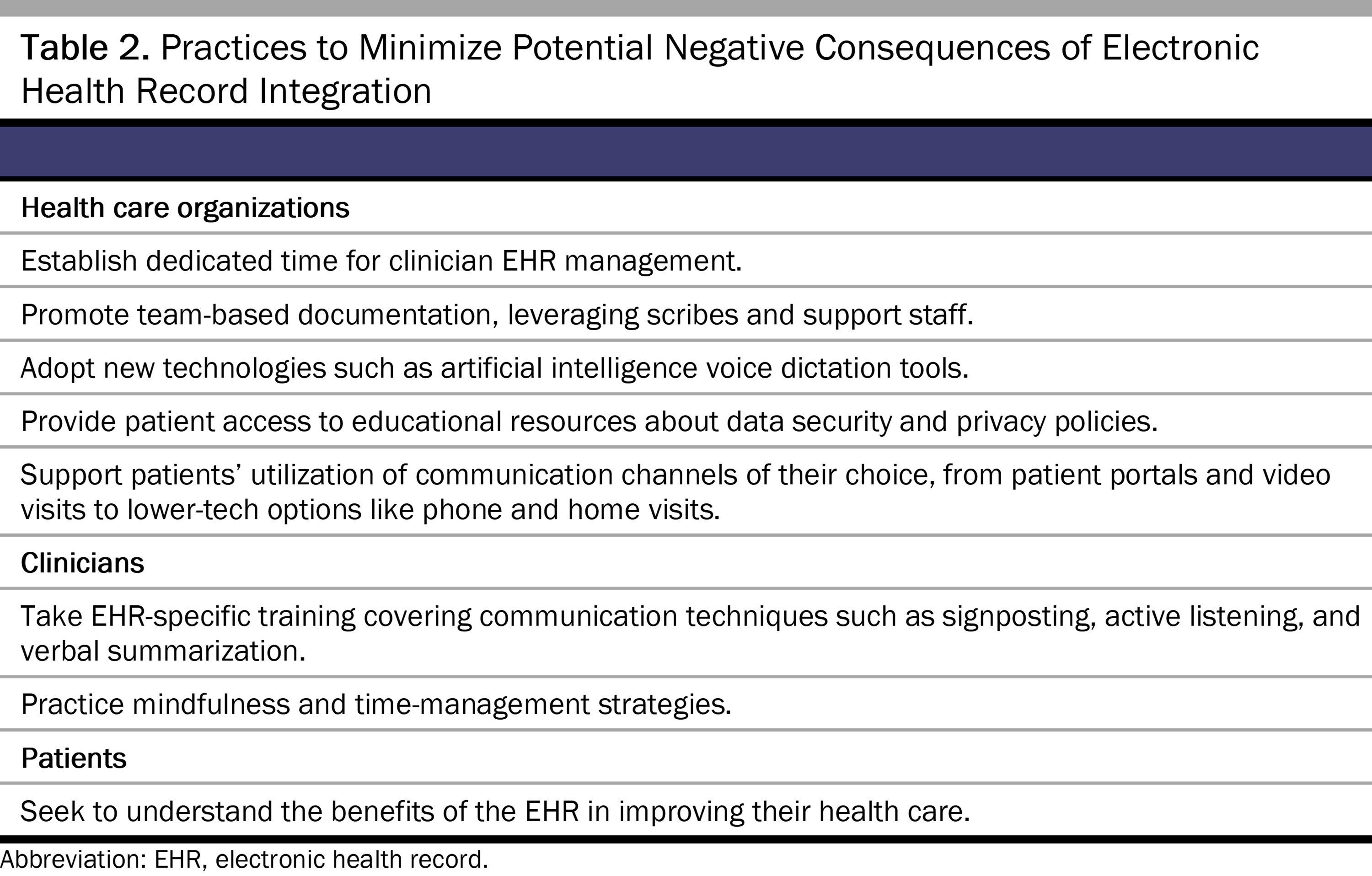
Given the limited time available for clinical interactions, prioritizing EHR use over essential elements such as touch, dialogue, and patient engagement can have significant consequences. Increased EHR use during clinical encounters has been shown to detract from rapport building, which can decrease patient satisfaction.8 From a patient’s perspective, the optimal clinic visit length varies widely but averages 15 minutes in ambulatory settings.9 If a third of this time is spent on the EHR, patients might experience the encounter as brief or rushed, which negatively affects their perception of the quality of care.10,11,12 This shift in focus toward screen gazing and EHR use also has the potential to diminish human intimacy, emotional responsiveness, and open discussion about sensitive issues.13 These personal elements serve as the foundation for a trusting and meaningful patient-centered relationship. Thus, it is critical for clinicians to leverage the EHR to educate and communicate with patients while enhancing human connectedness. Clinicians, as well as organizations and patients, can counteract or minimize potential negative consequences of EHR usage in several ways (see Table 2).
EHRs offer abundant clinical information, often in excess of what is clinically necessary or helpful for decision-making. This information overload often hinders workflows and exacerbates cognitive burden, which, in turn, can contribute to medical errors and clinician burnout due to inefficient EHR use.6,14,15
PCPs, in particular, have increased workloads due to EHR tasks before, during, and after patient encounters.6 For every hour they spend with patients, they spend almost twice that amount of time on EHR-related tasks during the workday, plus an additional 1 to 2 hours at home.3,5 Increasingly complex EHR billing and documentation are primary reasons clinicians spend more time with their computers than with their patients.16 In fact, a study that logged user event data in the EHR for PCPs found that they spent 44.2% of their time in the EHR performing administrative tasks such as documentation and order entry.15 Once given as a quick verbal instruction, order entry has evolved into a complex and time-consuming electronic task, taking an average of 12.1% of a clinician’s daily EHR time.15 Furthermore, system security tasks, such as 2-factor authentication to protect patient data and reduce unauthorized prescribing incidents, can further increase EHR-task time.17 Given that 2-factor authentication is not federally mandated for noncontrolled substances, these additional keystrokes and time spent in the EHR might not always be necessary.17
Cognitive burden is also a consequence of many EHRs being designed with minimal input from the users themselves—clinicians and patients—which is why they might be cumbersome and user unfriendly. Despite receiving a System Usability score in the bottom 9th percentile (“not acceptable”) of all industries surveyed,18 EHR vendors are largely unaffected by the criticism. In 2009, the Health Information Technology for Economic and Clinical Health Act catalyzed EHR adoption through financial incentives, whereby market saturation was achieved without major technical innovations.19 Market share for the top 2 EHR vendors nearly doubled from 2012 to 2021, increasing from 34% to 56%, as overall adoption surged from 7% to 81% between 2009 and 2019.20,21 Large health care systems continue to endorse solutions from the top few vendors without offering agency to employees in build customization.22,23
Many clinicians find multitasking a stressful and demanding aspect of their jobs. True multitasking, or concentrating on complicated computer interactions while simultaneously holding a conversation with and attending to the patient, is difficult, if not impossible, and can impede the quality of patient-centered communication and care.24,25 It is one of the reasons for high rates of prescribing errors.26 Clinicians might also miss important test results and ignore best practice reminders because of the overabundance of information in the EHR, a phenomenon known as “alert fatigue.”27,28
Usability and interoperability challenges within and between EHR systems can also create an excessive burden for clinicians and pose safety risks for patients.29,30,31,32,33Some organizations utilize multiple EHR systems to allow for more specialized functionalities for scheduling and department-specific tasks.34 However, patient safety can be compromised if clinical data, such as a patient’s newly prescribed medication, is not exchanged appropriately between systems.34 This lack of interoperability might also lead to order duplication, causing an unnecessary strain on the hospital system and frustration among clinicians.31,34 An excessive workload, coupled with high message volumes and perceptions of poor EHR usability, can lead to emotional fatigue, depersonalization, and burnout among clinicians.6,18,35,36,37
It is easy to see why clinicians might want to make up for time lost to the EHR by focusing on the iPatient and clinician-centric data rather than involving the patient in the diagnostic and treatment process.38,39,40 This tendency has become increasingly evident in hospital settings, with teams rounding either outside patient rooms or in workrooms far removed from the patient’s bedside rather than engaging with the actual patient and their families.41,42 As a result, opportunities can be missed to include patients in their care and to promote shared decision-making and patient education opportunities.
Empathy is crucial for building a trusting relationship and is associated with improved patient satisfaction and outcomes.43,44 However, the burden of miscellaneous EHR tasks contributes significantly to clinician burnout, which can, in turn, decrease empathy, jeopardizing the trusting relationships crucial for optimal patient care and outcomes.6,18,35,36,45,46,47 The annual prevalence of clinician burnout has been above 45% in the 2020s, and the EHR is frequently reported as an important stressor in patient care, with nearly 71% of PCPs in 2018 identifying the EHR as a contributor.6,7,48 While many clinicians might not meet the formal definition of burnout, they increasingly suffer from EHR moral injury. It should be a top priority of the health care system to address clinicians’ conflicts about their personal values and the competing demands imposed upon them in the current practice of medicine in order to foster a health care system that prioritizes both patient well-being and clinician fulfillment.49
Medicine is a noble profession rooted in humanism, human touch, dialogue, and engagement. Forming meaningful relationships with patients is one of the most important and rewarding parts of clinicians’ daily work, along with nurturing trainees, helping them achieve their highest potential, and witnessing them develop into clinically excellent clinicians. However, the EHR has altered clinician workflows and responsibilities, clinicians’ core relationships with patients, the hidden curriculum, and education delivered to trainees.
Despite these challenges, there are ways to enhance patient engagement with the EHR to prioritize patient-centered care. Strategies such as showing patients the computer screen can harness the EHR as a communication and engagement tool (see Figure).38,50,51
Figure. Patient EHR Self-Advocacy Comic
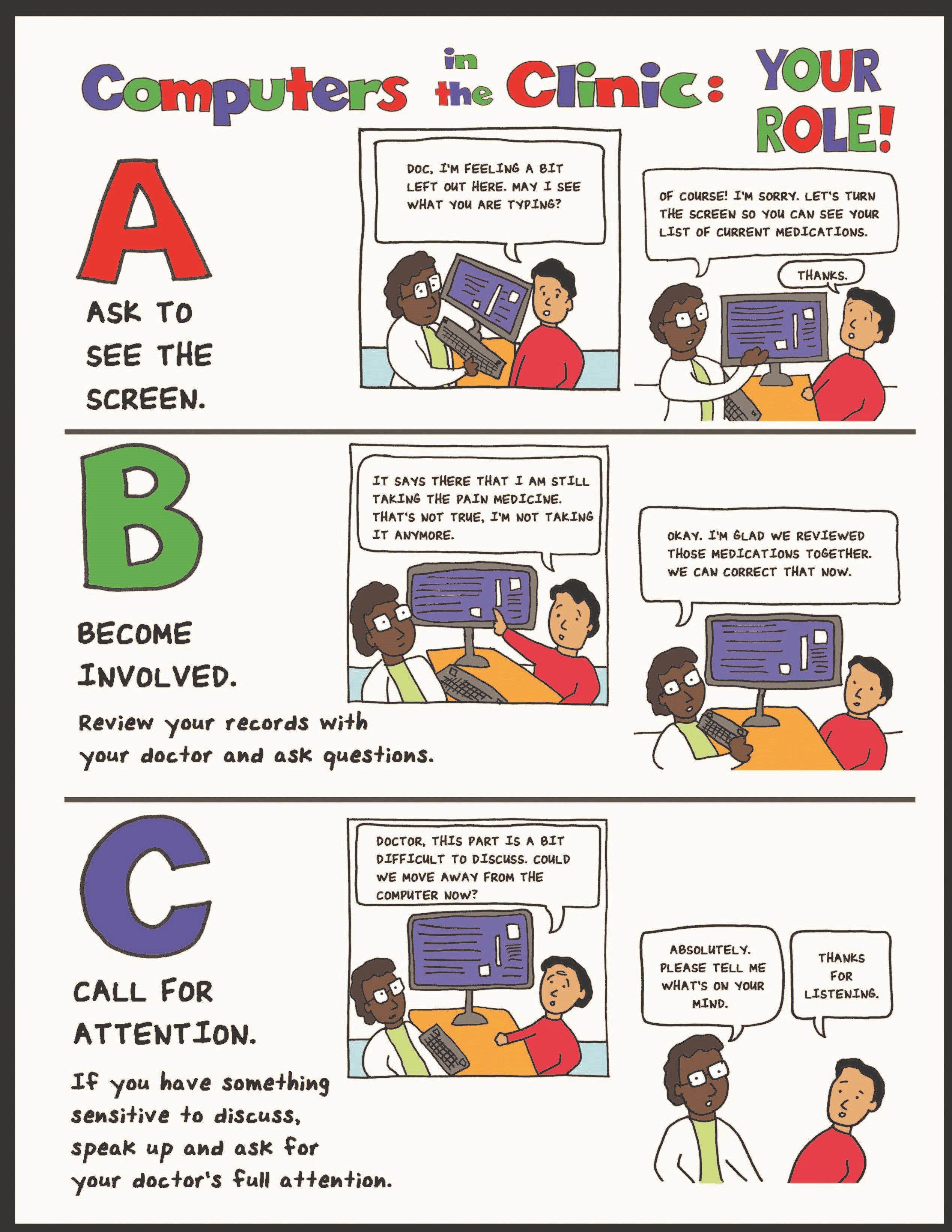
Reproduced with permission of Maria Alcocer Alkureishi. © Alkureishi MA, Czerwiec MK, Arora V, Lee WW, and the Arnold P. Gold Foundation.51
An example of an educational comic to encourage EHR self-advocacy behaviors and engagement given to adult patients and parents of pediatric patients when registering for their clinic visits.
Abbreviation: EHR, electronic health record.
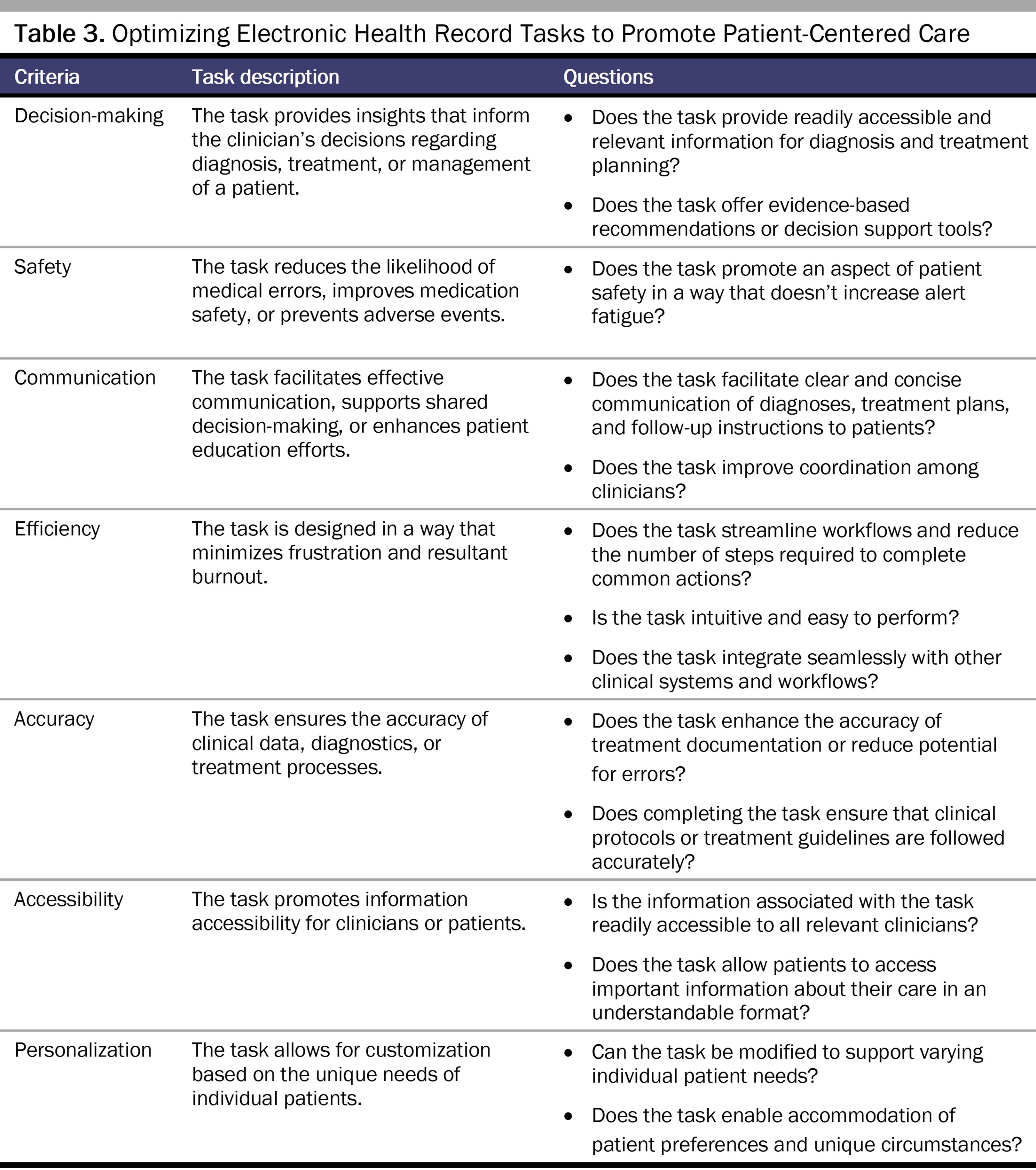
EHR efficiency training and tools, such as artificial intelligence dictation, can help mitigate clinician burnout, optimize health care efficiency, and increase clinician satisfaction with the EHR.52,53 Furthermore, increased patient and clinician participation during the EHR design process is needed to improve EHR capabilities and better serve clinician and patient needs (see Table 3).53,54,55,56 Lastly, administrative support and time to attend to EHR demands are critical in avoiding burnout and allowing clinicians to work in an effective and productive manner.55,56
As the integration of technology and its advancement in medicine continues, it is crucial to reduce the daily cognitive load of clinicians and their multitasking burden while they are caring for patients. Since PCPs notably spend a significant amount of time performing tasks in the EHR, tools, resources, and improved design of the EHR to support clinician usage are essential.
It is essential to be cognizant of the potential negative influences of EHRs to avoid them proactively. We look forward to optimizing EHR usage and development via enhanced EHR education, continued quality improvement, and systems-based research. By doing so, it is possible to leverage the EHR to promote humanistic, patient-centered care and to allow clinicians to return to the joy of connecting with patients and practicing meaningfully in the digital age.49
Verghese A. A doctor’s touch. TED. July 2011. Accessed October 28, 2024. https://www.ted.com/talks/abraham_verghese_a_doctor_s_touch?utm_campaign=tedspread&utm_medium=referral&utm_source=tedcomshare
Budd J. Burnout related to electronic health record use in primary care. J Prim Care Community Health. 2023;14:21501319231166921.
The Harris Poll. How doctors feel about electronic health records. Stanford Medicine; 2018. Accessed October 28, 2024. https://med.stanford.edu/content/dam/sm/ehr/documents/EHR-Poll-Presentation.pdf
Neprash HT, Mulcahy JF, Cross DA, Gaugler JE, Golberstein E, Ganguli I. Association of primary care visit length with potentially inappropriate prescribing. JAMA Health Forum. 2023;4(3):e230052.
Ratanawongsa N, Matta GY, Bohsali FB, Chisolm MS. Reducing misses and near misses related to multitasking on the electronic health record: observational study and qualitative analysis. JMIR Hum Factors. 2018;5(1):e4.
Sah S. Investigations before examinations: “this is how we practice medicine here.” JAMA Intern Med. 2015;175(3):342-343.
Is two-factor authentication required for all prescriptions? American Medical Association. July 14, 2023. Accessed October 28, 2024. https://www.ama-assn.org/practice-management/sustainability/two-factor-authentication-required-all-prescriptions
Colicchio TK, Cimino JJ, Del Fiol G. Unintended consequences of nationwide electronic health record adoption: challenges and opportunities in the post-meaningful use era. J Med Internet Res. 2019;21(6):e13313.
Jiang JX, Qi K, Bai G, Schulman K. Pre-pandemic assessment: a decade of progress in electronic health record adoption among US hospitals. Health Aff Sch. 2023;1(5):qxad056.
Bosic-Reiniger J, Martin JL, Brown KE, et al. Barriers and facilitators of the use of clinical informatics resources to facilitate pharmacogenomic implementation in resource-limited settings. JAMIA Open. 2024;7(4):ooae101.
Anderson E, Moldestad M, Brunner J, et al. User experiences of transitioning from a homegrown electronic health record to a vendor-based product in the Department of Veterans Affairs: qualitative findings from a mixed methods evaluation. JMIR Form Res. 2024;8:e46901.
Greatbatch D, Heath C, Campion P, Luff P. How do desk-top computers affect the doctor-patient interaction? Fam Pract. 1995;12(1):32-36.
Booth N, Robinson P. Interference with the patient-doctor relationship—the cultural gap? Lessons from observation. Stud Health Technol Inform. 2002;87:6-9.
Ancker JS, Edwards A, Nosal S, Hauser D, Mauer E, Kaushal R; HITEC Investigators. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inform Decis Mak. 2017;17:36.
Kruse CS, Mileski M, Dray G, Johnson Z, Shaw C, Shirodkar H. Physician burnout and the electronic health record leading up to and during the first year of COVID-19: systematic review. J Med Internet Res. 2022;24(3):e36200.
Delgado N, Delgado J, Betancort M, Bonache H, Harris LT. What is the link between different components of empathy and burnout in healthcare professionals? A systematic review and meta-analysis. Psychol Res Behav Manag. 2023;16:447-463.
Ward DR, Ghali WA, Graham A, Lemaire JB. A real-time locating system observes physician time-motion patterns during walk-rounds: a pilot study. BMC Med Educ. 2014;14:37.
Wilkinson H, Whittington R, Perry L, Eames C. Examining the relationship between burnout and empathy in healthcare professionals: a systematic review. Burn Res. 2017;6:18-29.
Wu Y, Wu M, Wang C, Lin J, Liu J, Liu S. Evaluating the prevalence of burnout among health care professionals related to electronic health record use: systematic review and meta-analysis. J JMIR Med Inform. 2024;12:e54811.
Alkureishi MA, Lee WW, Lyons M, et al. Impact of electronic medical record use on the patient-doctor relationship and communication: a systematic review. J Gen Intern Med. 2016;31(5):548-560.
Alkureishi MA, Johnson T, Nichols J, et al. Impact of an educational comic to enhance patient-physician-electronic health record engagement: prospective observational study. JMIR Hum Factors. 2021;8(2):e25054.
Fogleman BM, Goldman M, Holland AB, Dyess G, Patel A. Charting tomorrow’s healthcare: a traditional literature review for an artificial intelligence-driven future. Cureus. 2024;16(4):e58032.
Busse TS, Jux C, Laser J, et al. Involving health care professionals in the development of electronic health records: scoping review. JMIR Hum Factors. 2023;10:e45598.
Kroth PJ, Morioka-Douglas N, Veres S, et al. Association of electronic health record design and use factors with clinician stress and burnout. JAMA Netw Open. 2019;2(8):e199609.
American Medical Association Advisory Committee on EHR Physician Usability. Improving care: priorities to improve electronic health record usability. American Medical Association; 2014. Accessed October 28, 2024. https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/member/about-ama/ehr-priorities.pdf



