Case and Commentary
Aug 2025
Peer-Reviewed

Is there an important ethical difference between a global catastrophe that causes human extinction and one that does not? This commentary on a case introduces 3 approaches—equivalence, further-loss, and pro-extinctionist—in responding to this question. In particular, focus is placed on equivalence and further-loss views’ implications for how clinicians, health professions, and health care organizations orient themselves ethically towards managing the risk of extinction.
Consider 2 hypothetical worlds.1 World A contains 11 billion people. World B contains 10 billion. Now imagine that, in both worlds, a global catastrophe causes exactly 10 billion people to die. In World A, one billion people survive, while human extinction occurs in World B (see Figure). Is there a reason to believe that the World B scenario is worse than the World A scenario? Moreover, if someone were responsible for causing the catastrophe in each world, should they be viewed as having done something “extra” morally wrong in World B?
Figure. Illustration of the “2-Worlds” Thought Experiment
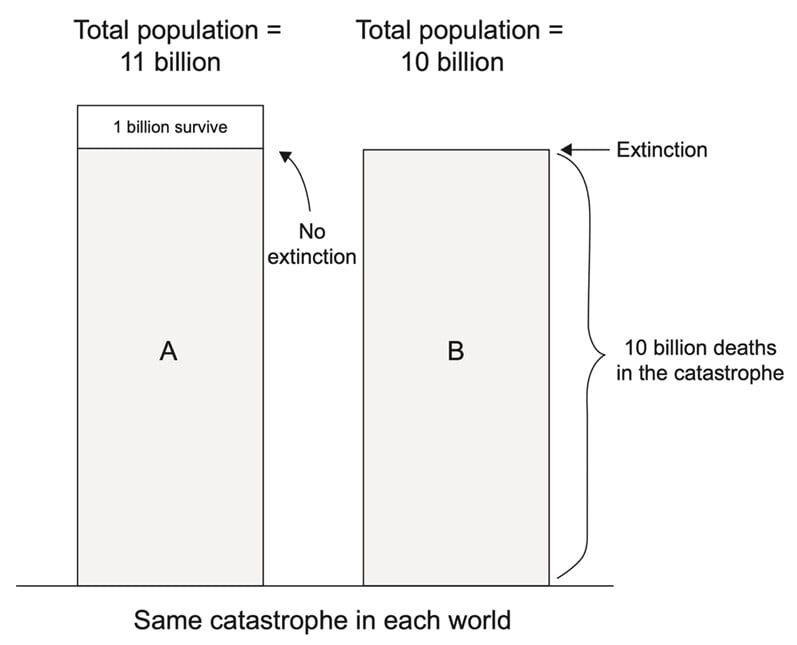
© 2023 Taylor & Francis Group. Reproduced from Torres1 with permission of the licensor through PLSclear.
In both worlds, 10 billion people die in an identical global catastrophe. However, as World A has 1 billion more people than World B, extinction occurs in World B, but not in World A.
A topic of growing interest among contemporary moral philosophers concerns the ethical and evaluative implications of human extinction. With some exceptions,2,3,4,5,6,7 however, the literature on this topic has been largely ignored by the health care community, and philosophers have said little about the role of health professionals in preventing human extinction. This disconnect is problematic for at least 2 reasons. First, some views on the ethics of human extinction suggest that health care as practiced today may be ethically misguided. Second, the practical expertise of health professionals (eg, an appreciation of the suffering caused by diseases or the concrete effects of health policy on patients’ lives) may inform whether the first point is truly the case and, if so, what can be done about it.5
We attempt to rectify this situation by outlining a theoretical framework for thinking about the ethics of human extinction, which groups various positions in the field into 3 categories: equivalence views, further-loss views, and pro-extinctionist views (see Table).1 Each view is based on a fundamental distinction between (1) the process of Going Extinct and (2) the subsequent state of Being Extinct. To address the questions posed by the “2-worlds” thought experiment above, we will focus solely on equivalence and further-loss views and define human extinction as having occurred if humanity ceases to exist forever without leaving behind any successors (sometimes called “final” human extinction).1 The following sections offer an overview of the arguments for these views and then explore their potential implications for health care.
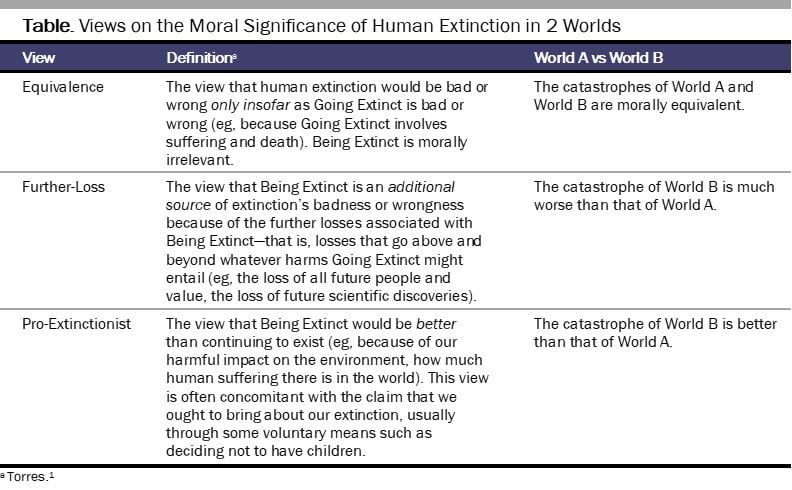
Equivalence views claim that our extinction would be bad or wrong only insofar as Going Extinct would be bad or wrong. Hence, if the event(s) that occurred while Going Extinct involved nothing bad or wrong, our extinction would also not be bad or wrong.
For example, imagine a nuclear war that causes immense suffering and kills all 8 billion people8 currently living on Earth. Equivalence theorists would say that our extinction under such circumstances would be very bad and wrong because Going Extinct in this way would be very bad and wrong. In contrast, imagine that everyone voluntarily decides not to have children, causing the worldwide population to fall to zero. Equivalence theorists would argue that, in this scenario, our extinction would be neither bad nor wrong, since (many would claim) there is nothing bad or wrong about anyone deciding, for any reason, not to procreate. For such theorists, the resulting state of Being Extinct is morally irrelevant: unlike Going Extinct, Being Extinct cannot harm anyone, since no one would exist to suffer the nonexistence of humanity. It thus cannot be bad or wrong. All that matters, ethically, are the details of Going Extinct.
Equivalence views imply that human extinction does not pose any special moral problems. The only difference between a catastrophe that kills 99% of the population and one that kills 100% is a single percentage point.9 Equivalence views follow from so-called “person-affecting” moral theories such as Scanlonian contractualism and Jan Narveson’s utilitarianism, both of which posit that an actual, existing person must be affected by an event, such as Going Extinct, in order for that event to be good or bad.10,11
Consider again the 2-worlds thought experiment. Equivalence theorists would say that the catastrophe of World B, which results in human extinction, is no worse than the catastrophe of World A, which leaves 1 billion survivors. If someone named Tom is responsible for causing both of these catastrophes, he does not do anything extra wrong in World B. The badness or wrongness of what happens in World B just is the badness or wrongness of 10 billion people being killed. This is why we call it the “equivalence” view.
From a health care perspective, equivalence theorists could argue that health professionals have no special obligation to prevent our extinction per se. Health professionals may, of course, have an obligation to prevent suffering and death and, hence, insofar as Going Extinct would cause suffering and death, they would be obligated to prevent us from Going Extinct. But, if everyone were to voluntarily decide to be childless, health professionals may be obligated to—in effect—facilitate our extinction by making contraception accessible, even if causing humanity’s extinction is not their specific intention (that is, assuming they have an obligation to provide such access in the first place). Although everyone deciding to be childless is exceedingly unlikely, the point is to highlight the implications of equivalence views for health care.
As far as we can tell, equivalence views do not prescribe significant changes to the commonly espoused goals of medicine or public health in academic literature. These goals include, for example, those outlined by Christian Munthe and Christopher Boorse, which focus on promoting the health, autonomy, and equality of individual patients and broader populations, in addition to acquiring knowledge of how to bring about those ends.12,13 These goals are only concerned with people existing here and now—ie, those who would be affected by the process of Going Extinct—but say nothing about Being Extinct, consistent with the claim that human extinction does not introduce any special moral problems.
However, the goals of health care can change radically based on how one defines concepts such as medicine or health. For example, Alex Broadbent defines health as “states that promote the survival and reproduction of the species,”14 and, hence, health care would by definition involve engaging in actions that prevent extinction.6 Further-loss views similarly suggest that traditional health care should be reconceptualized with an emphasis on future generations, as we will now discuss.
Whereas equivalence views claim that assessing the badness or wrongness of human extinction only involves examining the details of Going Extinct, further-loss views assert that a second step is required, namely, considering the various “further losses” or “opportunity costs” associated with Being Extinct. In the 2-worlds thought experiment, further-loss theorists would contend that the catastrophe in World B is far worse than that in World A, because our extinction in World B would preclude the realization of future goods that could have otherwise existed (eg, happiness, satisfied desires, the development of the arts and sciences).
Totalist utilitarianism is one type of further-loss view.15 It holds that we are morally obligated to maximize total well-being (or intrinsic value) in the universe. According to modern cosmology, the universe may remain habitable for billions or trillions of years.16 If humanity spreads beyond Earth and survives for such periods, there could be “astronomical” numbers of future people, many more than have ever existed thus far.15,17 Assuming they would have “happy” or “worthwhile” lives on average, the “loss” of these people would constitute an additional source of extinction’s badness or wrongness. Notice that this loss is unrelated to how Going Extinct unfolds: whether humanity dies out from nuclear war or because everyone voluntarily decides to stop procreating, the opportunity costs of Being Extinct would be unchanged.
For further-loss theorists who expect the long-term future to be full of immense, positive value, the difference between an extinction-causing and a non-extinction-causing catastrophe is thus one of kind rather than degree: 100% of humanity dying off would be immensely worse than “only” 99% dying off.9 This view implies that human extinction does pose special moral problems: it is the only event that would guarantee the loss of all future value, which could be many orders of magnitude larger than all the value thus far created. As 3 advocates of this view write: “One very bad thing about human extinction would be that billions of people would likely die painful deaths. In our view, this is, by far, not the worst thing about human extinction. The worst thing about human extinction is that there would be no future generations.”18 Hence, even if Going Extinct were to cause terrible suffering, the death of the 8 billion current people pales in comparison to the nonexistence of the trillions or quintillions of people who could have otherwise existed.9 This particular claim is associated with a further-loss view known as longtermism, which is closely connected to totalist utilitarianism.19,20
Whereas equivalence views may not prescribe major changes to current health care systems, longtermism likely would. It implies that preventing human extinction should take precedence over preventing billions of painful deaths, if those deaths (or the underlying causes of those deaths) pose no threats to our collective survival. Hence, we should allocate a large portion of society’s resources to ensuring our survival. The longtermist Toby Ord, for example, recommends allocating 1% of global GDP toward mitigating “existential risk.”21 That equaled $1 trillion in 2023, more than enough to end world hunger, eliminate global poverty, and provide sanitary drinking water in 140 low- and middle-income countries, if done on a per-year basis.22,23,24,25 Notably, this is not an either/or scenario. For instance, one can say that society should allocate $1 trillion to these humanitarian causes and to preventing human extinction (eg, by reallocating portions of the 2.3% and 9.1% of global GDP spent on the military and travel, respectively).26,27 Health professionals could play important roles in advocating for such resource redistribution.
While some longtermists do support humanitarian initiatives (Ord included),28 it is important to recognize what many might construe as the logical conclusion of longtermism: a large fraction of the health care workforce should stop treating patients and instead focus on the long-term fate of humanity’s descendants in the cosmos over the coming billions of years. For example, in their initial argument for a “strong” form of longtermism, philosophers Hilary Greaves and William MacAskill claimed that, “for the purposes of evaluating actions, we can in the first instance often simply ignore all the effects contained in the first 100 (or even 1000) years, focussing primarily on the further-future effects. Short-run effects act as little more than tie-breakers [italics in original].”20
If population collapse is ever perceived to threaten our species, health professionals who embrace a further-loss view might also be inclined to prevent people from accessing contraceptives. In essence, endorsing Henry Sidgwick’s view that “a universal refusal to propagate the human species would be the greatest of conceivable crimes”29 seems to imply that, if humanity’s long-term future depends on it, certain human rights might be trampled upon or at least restricted. For example, investing in longtermist projects, such as colonizing Mars or working to ensure the “safety” of building what some call “God-like AI,”30 could be prioritized instead of providing basic access to health care.
While there are certainly instances in which health professionals’ promotion of policies that prioritize the “greater good” over autonomy might be justified (eg, masking mandates during a pandemic, involuntary psychiatric treatment when a patient threatens themselves or others), health professionals can help evaluate the credibility of longtermist claims through the lens of health and warn, when appropriate, about risks of prioritizing our collective survival.
Equivalence and further-loss views thus have quite different implications for health care. The former does not, it seems, prescribe an overhaul of our health care systems. In contrast, the latter, especially longtermism, might imply to some that health professionals, policies, and institutions must strongly prioritize addressing threats to humanity’s long-term future, during which many trillions of not-yet-born people could live “happy” lives. Both views would agree that we should avoid human extinction if caused by a catastrophe, although for quite different reasons. For equivalence theorists, extinction-causing catastrophes are among the worst-possible type of catastrophe, given the enormous magnitude of suffering and premature death they could cause. However, there is no ethical difference between extinction-causing and non-extinction-causing catastrophes on the equivalence view (ie, in the 2-worlds thought experiment, the catastrophes of World A and B are equally bad or wrong). Therefore, we have no reason to strongly prioritize avoiding our extinction. This view is opposed to further-loss views that contend that, because World B involves astronomical amounts of “impersonal” harm (ie, all the future value that could have otherwise existed), World B is much worse than World A, and hence we must strongly prioritize preventing extinction, whether caused by asteroid impacts, nuclear war, or people around the world voluntarily deciding not to have children.
We have presented these views as stark dichotomies for emphasis. In our view, a long lifespan for humanity would be good (assuming that future lives are worthwhile); health care should thus help ensure that there are future people, although not at any cost. Another approach would be to say that, insofar as we have reasons to believe that not-yet-born future people will in fact exist—and we do have such reasons at present—health care should work to ensure that their lives are sufficiently well-off without wholly neglecting the needs of current patients. However, like equivalence theorists, we are not convinced that Being Extinct itself would be bad or wrong, although we believe that Going Extinct would likely involve enormous suffering and premature death (ie, the most probable scenarios of Going Extinct would be violent and involuntary). In light of health professionals’ responsibility to act in the interests of their patients’ health, they should therefore help prevent such catastrophes to a greater degree than they do at present. In other words, an extinction-causing catastrophe would likely entail such terrible harms to billions of people that focusing on preventing or responding to such catastrophes does justify, to some extent, more attention than it currently receives from health professionals.
The World Medical Association claims that physicians hold responsibilities to future generations.31 This stipulation adds urgency to the project of fostering an inclusive, global consensus regarding how, to what extent, and under which conditions society should prevent our extinction. We argue that, given the substantially different implications of the equivalence and further-loss views, such a project should be pursued, and health professionals should contribute to it. This effort would require a global collaboration to better understand the current existential threat environment and the drafting of an unbiased overview of positions in the ethics of human extinction, among other things, akin to a recent proposal and US governmental report.32,33 Health professionals could help, for example, by outlining the detailed proximate biological mechanisms by which human extinction could occur. We have also argued that a new medical specialty could focus on these issues, which one of us (D.M.K) proposes calling “extinction medicine.”7,34
Lastly, this article does not present an exhaustive analysis of the issue—far from it. We have said nothing about, for example, the third major position within the ethics of human extinction: pro-extinctionism, versions of which are advocated for by some philosophical pessimists, radical environmentalists, and contemporary technologists who endorse near-term replacement of our species with “intelligent machines.” Nonetheless, we hope this overview provides a useful point of departure for future discussions on the (potentially very important) role of health professionals in ensuring the just perpetuation of humanity.
Torres ÉP. Human Extinction: A History of the Science and Ethics of Annihilation. Routledge/Taylor & Francis Group; 2023.
Razis DV. Modern Cassandras and our survival as a species—a new role for medicine? J R Soc Med. 1989;82(10):575-576.
Bryan CS, Kellis DM, Sokol D. Osler’s valediction: how might physicians contribute to the effort to postpone human extinction? BMJ. 2024;384:q499.
Bryan CS, Kellis DM. Osler’s gravest prognosis: extinction. Pharos Alpha Omega Alpha Honor Med Soc. 2024;2:19-23. Accessed March 26, 2025. https://www.alphaomegaalpha.org/wp-content/uploads/2024/02/pp19-23-Bryan_Osler_WIN24.pdf
Kellis DM, Torres ÉP. Extinction medicine: the case for a new medical specialty. SSRN. January 23, 2025. Accessed February 3, 2025. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5109482
World population by year. Worldometer. Accessed April 28, 2025. https://www.worldometers.info/world-population/world-population-by-year/
Parfit D. Reasons and Persons. Oxford University Press; 1986.
Finneron-Burns E. What’s wrong with human extinction? Can J Philos. 2017;47(2-3):327-343.
Boorse C. Goals of medicine. In: Giroux E, ed. Naturalism in the Philosophy of Health: Issues and Implications. Springer; 2016:145-177.
Broadbent A. Health and disease. In: Philosophy of Medicine. Oxford University Press; 2019:93-126.
Mack K. The End of Everything (Astrophysically Speaking). Scribner; 2021.
Newberry T. How many lives does the future hold? Global Priorities Institute, University of Oxford; 2021. GPI technical report T2-2021. Accessed September 29, 2024. https://globalprioritiesinstitute.org/wp-content/uploads/Toby-Newberry_How-many-lives-does-the-future-hold.pdf
Singer P, Beckstead N, Wage M. Preventing human extinction. Effective Altruism Forum. August 19, 2013. Accessed February 7, 2025. https://forum.effectivealtruism.org/posts/tXoE6wrEQv7GoDivb/preventing-human-extinction
MacAskill W. “Longtermism.” Effective Altruism Forum. July 25, 2019. Accessed February 7, 2025. https://forum.effectivealtruism.org/posts/qZyshHCNkjs3TvSem/longtermismMacAskill
Greaves H, MacAskill W. The case for strong longtermism. Global Priorities Institute, University of Oxford; 2021. GPI working paper 5-2021. Accessed November 19, 2024. https://globalprioritiesinstitute.org/wp-content/uploads/The-Case-for-Strong-Longtermism-GPI-Working-Paper-June-2021-2-2.pdf
Ord T. The Precipice: Existential Risks and the Future of Humanity. Hachette Books; 2020.
GDP, current prices: billions of US dollars. International Monetary Fund. 2025. Accessed July 15, 2025. https://www.imf.org/external/datamapper/NGDPD@WEO/OEMDC/ADVEC/WEOWORLD
Summer A, Yusuf AA. New estimates of the cost of ending poverty and its global distribution. World Institute for Development Economics Research, United Nations University; 2024. WIDER working paper 2024/46.
How much money would it take to end world hunger? Oxfam. December 9, 2022. Accessed September 13, 2024. https://www.oxfamamerica.org/explore/stories/how-much-money-would-it-take-to-end-world-hunger/
World Water Assessment Programme. The United Nations World Water Development Report 2021: Valuing Water. UNESCO; 2021. Accessed September 9, 2024. https://unesdoc.unesco.org/ark:/48223/pf0000375724
Tian N, da Silva DL, Liang X, Scarazzato L. Trends in world military expenditure, 2023. SIPRI; 2024. Accessed February 7, 2025. https://www.sipri.org/sites/default/files/2024-04/2404_fs_milex_2023.pdf
Total contribution of travel and tourism to gross domestic product (GDP) worldwide in 2019 and 2023, with a forecast for 2024 and 2034. Statistica. July 15, 2024. Accessed February 7, 2025. https://www.statista.com/statistics/233223/travel-and-tourism-total-economic-contribution-worldwide/
Matthews D. This man has donated at least 10% of his salary to charity for 11 years running. Vox. November 30, 2020. Accessed March 22, 2025. https://www.vox.com/future-perfect/21728925/charity-10-percent-tithe-giving-what-we-can-toby-ord
Sidgwick H. The Methods of Ethics. DigiCat; 2022.
Tangermann V. Sam Altman seems to imply that OpenAI is building God. Futurism. November 15, 2023. Accessed March 22, 2025. https://futurism.com/sam-altman-imply-openai-building-god
WMA international code of medical ethics. World Medical Association. Adopted October 1949. Revised October 2022. Accessed March 1, 2024. https://www.wma.net/policies-post/wma-international-code-of-medical-ethics/
Bressler RD, Alstott J. The International Panel on Global Catastrophic Risks (IPGCR). In: Zimmer D, Undheim TA, Edwards PN, eds. Intersections, Reinforcements, Cascades: Proceedings of the 2023 Stanford Existential Risks Conference. Stanford Existential Risks Initiative, Stanford University; 2023:233-247. Accessed March 26, 2025. https://stacks.stanford.edu/file/druid:pn116pv4512/Intersections,%20Reinforcements,%20Cascades_Proceedings%20of%20the%202023%20Stanford%20Existential%20Risks%20Conference.pdf
Willis HH, Narayanan A, Boudreaux B, et al. Global catastrophic risk assessment. RAND; 2024. Accessed July 9, 2025. https://www.fie.undef.edu.ar/ceptm/wp-content/uploads/2024/11/RAND_RRA2981-1.pdf

