Case and Commentary
Aug 2025
Peer-Reviewed

This commentary on a case builds on recent literature on climate change, health, and human extinction to argue in favor of a new clinical specialty: extinction medicine. If based on precise application of scientific findings about species extinction, disaster prevention and management, and health policy, such a specialty could help reduce humanity’s extinction risk. Finally, the commentary suggests extinction medicine competencies, who might become an extinction medicine clinician, and how the specialty might be launched.
Dr B is a pediatric internist considering how to care well for patients experiencing anxiety and moral trauma related to human-caused climate change. Dr B feels they and their clinician colleagues are generally unprepared to help their patients, their organizations, and their professions navigate such global health threats that many people tend to experience as overwhelming and unmanageable. Dr B organizes a meeting at their state medical association to discuss the issue.
A number of Dr B’s fellow physicians throw their hands up and leave the room when Dr B mentions some of the following facts or hypothetical threats: not including morbidity and other measures of suffering, fossil fuels have already contributed to millions of premature human deaths1,2; some academicians speculate that for every 1000 tons of CO2 emitted, one future person might die a premature death (ie, the “1000-ton rule”), potentially amounting to a billion future premature deaths over the next 1 to 2 centuries3,4; and many of the communities at most risk of dying from climate change have historically emitted relatively little greenhouse gases, such as CO2 or methane, and have access to relatively few health professionals.5,6
Although Dr B doubts that climate change would lead to human extinction, they wonder whether their finite time is better spent addressing threats to humanity as a whole rather than attending to individual patients. Dr B considers leaving medicine as currently widely practiced and wonders what to do.
Threat detection and response are key to organismal survival and well-being, which jointly constitute health. Whether it be single-cell bacteria sensing danger, plants’ activation of pattern-triggered immunity, or animals defensively freezing, acute threat processing in local settings is virtually universal in biology.7,8,9 Yet humanity’s ability to ponder our extinction is evolutionarily new.
With respect to climate change, some philosophers have indicated that something like human extinction is unlikely.10,11 However, there are advocates who think it is within the realm of possibility, even likely.12 When evaluating such claims, focus must be placed on evaluating whether there might be credible scientific mechanisms by which the human population could dwindle to zero. While outlining exact pathways by which climate change could contribute to the risk of human extinction is difficult and underexplored, there is no denying that rising global temperatures lead to increased mortality through their influence on heat waves, droughts, floods, hurricanes, and wildfires. The World Health Organization, for example, has estimated that approximately 250 000 excess deaths from malaria, diarrheal diseases, dengue, undernutrition, and excess heat will occur due to climate change every year from 2030 to 2050, over 90% of which are expected to occur in low- and middle-income countries.13 In light of one estimate in 2020 indicating that only 7 high-income areas in the Global North emitted 92% of CO2 emissions from 1850 to 2015,8 these projected deaths are also an issue of health justice. Whether and to what extent climate change-related mortality projections come true (especially highly speculative estimates such as the 1000-ton rule)3,4 is dependent on decisions made today with respect to funding mitigation and adaptation efforts.
In addition to climate change negatively affecting health, some scientists worry that it could contribute to societal collapse by reinforcing interactions among other global threats related to inequality, violence, and resource scarcity, among others.14 In light of this risk, global risk scholar Luke Kemp perhaps says it best: we simply “do not know whether climate change or anthropogenic ecological disruption could spiral into human extinction.”15 That possibility ought to concern all of us, especially with more than 200 journals agreeing that the climate and biodiversity crisis is a global health emergency.16 With CO2 emissions hitting a new high in 2023 despite decades of effort to address the issue, it is no surprise that people are experiencing climate anxiety.17
Indeed, learning about global threats may trigger several cognitive, emotional, and behavioral responses in both patients and clinicians. The climate change and pandemic literatures focus mostly on fear, anxiety, grief, and denial.18,19 In the 20th century, studies of nuclear anxiety also emphasized “psychic numbing,” a blunted emotional response to mass atrocities, such as genocide or nuclear war, among others.20,21 Ideally, global threat responses would promote human survival and welfare through straightforward consensus building, public policy, and health law; however, the outcome is too often behavioral avoidance and intergroup conflict. Significantly less attention has been given to the psychological effects of thinking about human extinction, perhaps because so few people appear to be doing it. However, when we, like Dr B, do find the time to consider humanity’s extinction, our thinking about it is often shallow, fleeting, and in relation to a single hazard, such as global warming, nuclear weapons, or asteroids, considered in isolation. The planetary health movement and advancements in the field of existential risk studies (ERS) are increasingly recognizing the need to consider global threats instead as a complex, interacting system.22,23,24,25,26 Despite this convergence of interests, medicine and ERS generally emphasize different moral theories (eg, deontology and duties to one’s patients and impartial utilitarianism,27 respectively). Regrettably, these differences have fostered an unwarranted situation: no profession has adopted a duty to prevent human extinction.
Some argue that medicine should step in to fill this gap by creating a new medical specialty, “extinction medicine,” which would aim to translate knowledge into actions that “promote humanity’s survival while minimizing social harm.”28 The development of such a specialty would provide a solution for Dr B, as it would allow Dr B to remain in the medical profession, but more broadly construed. This paper therefore bolsters the central thesis that extinction medicine should be created as a new specialty. After evaluating reasons and justifications as to why this is the case, a picture of what extinction medicine might look like is painted more fully.
Straightforward reasons for medicine to adopt specialized consideration of human extinction have been discussed recently.28 Select rationales are reiterated here in greater detail and in tandem with others drawn from literature on the ethics of human extinction.
Extinction cannot be cured. The first reason for medicine to care about extinction can be made by analogy with disease: while we can cure diseases after they happen, final human extinction cannot be cured.29 Once extinction occurs, that’s it—there are no do-overs. As Nick Bostrom makes clear, a “reactive approach—to observe what happens, limit damages, and then implement improved mechanisms to reduce the probability of a repeat occurrence—does not work when there is no opportunity to learn from failure.”29 It is therefore critical that human extinction be well understood from a mechanistic and human biological perspective, which medicine excels at. As Physicians for Social Responsibility indicates: “we must prevent what we cannot cure.”30
Extinction compromises human values. An additional consideration was emphasized by Jonathan Schell who stated that, with respect to those things that humanity finds valuable, “none of them have any meaning or application unless one first assumes the existence of … mankind.”31 There is little use for art, infrastructure, entertainment, sports, science, or cures for medical diseases if there is no one around to appreciate or benefit from those goods.
Extinction would harm every patient (past, present, and future). With respect to health, any instantaneous extinction event would cause everyone who exists at that moment to die. These deaths would be premature if this event could otherwise have been prevented; however, an instant extinction (eg, via vacuum decay of the universe) is incredibly unlikely both to occur when humans are around and to be prevented.32 In the case of a more complex extinction event extended through time, which is more likely over the coming centuries and millennia, many premature deaths attributable to various proximate causes may occur. The amount of suffering caused may be greater than in non-extinction-causing catastrophes, a concept referred to as the no ordinary catastrophe thesis.33
If an extinction event (whether instantaneous or not) is foreseen, anticipation of it could cause great psychological despair,34 regardless of whether extinction risk is merely perceived and not real, or, if real, in the near- or very long-term future. Regardless of how human extinction comes about, if and when it does occur, there will be no more future generations after the fact. Although there would be no people around for whom this state of non-being would be harmful per se, anticipation of extinction could be bad for existing people for the duration of their remaining life prior to extinction, as it would call into question the meaning of human existence, which is an important contributor to mental health.35
Human extinction threatens what we might call the League of Patients: every patient who has been, is, and ever could be.
In addition to negatively affecting current and future generations, it has been argued that extinction would disrespect our ancestors and lead them to die a “second death.”36,37Altogether, then, human extinction affects not only current and future generations, but also, in some sense, past ones. To modify a phrase from the 20th century anti-nuclear activist, Günther Anders: human extinction threatens what we might call the League of Patients: every patient who has been, is, and ever could be.37
Focusing solely on treating individual patients might cause iatrogenic harm by increasing extinction risk. Consider 2 examples: medicine’s facilitation of resource extraction that impedes development of a circular economy and of climate change through resource expenditure.28 Modern health care, expenditure on which was 10% of global GDP in 2021,38 requires immense natural resources (and for good reason). Mass manufacturing of drugs and equipment (such as magnetic resonance imaging, X-ray, computed tomography, and ultrasound machines, as well as pacemakers, defibrillators, wearables, prosthetic, surgical robots, and other devices) requires rare earth elements and other critical minerals that are vulnerable to supply chain disruptions, such that medical use of these resources is now being considered from cross-sector competitive, national security, geopolitical, and systemic risk perspectives.39,40,41,42 A 2019 report also indicates that the health sector contributes 4.4% of global greenhouse gas emissions, an amount equivalent to that of the fifth largest emitter if it were a country.43 The flip side of medicine’s inadvertently increasing extinction risk is that its deliberate efforts to reduce this risk might help prevent iatrogenesis and serve as a model for reducing extinction risk arising from other social sectors.
The training of health professionals already provides transferable skills relevant to extinction prevention and harm-reduction: in-depth knowledge of pathophysiology, strong understanding of the basic sciences, communication skills, and teamwork, among others. Therapeutic approaches and future advancements in existing medical specialties, including emergency, disaster, reproductive, and space medicine, might help reduce suffering during a putative extinction event and extend the time during which humans can be born, experience life, and appreciate the world. Knowledge of other specialties, such as psychiatry or palliative care, might also have utility for clinicians if patients excessively ideate about extinction to their own or others’ detriment or if extinction becomes inevitable. In addition, extinction medicine specialists would be able to help evaluate the credibility of extinction threats, which could help guide human behavior in the context of existential anxiety.
Establishing a new specialty could also help frame human extinction as a health care issue, which might increase public support and funding for human extinction prevention and harm reduction. More specifically, establishing extinction medicine could help make evolutionary definitions of health part of the norm. As Pamela Ayo Yetunde and her colleagues say, “no one can be healthy when the community is sick.”44 Evolutionary definitions of health extend this community to humanity: being healthy requires existing in a state that nurtures the survival of our species.45 This “humanity perspective” can be illustrated with a thought experiment. Imagine that every person was set to live more than a century with faultless well-being but that the cost of this utopian state was human extinction in 200 years, significantly earlier than if emphasis were placed on extinction postponement and not merely individual life extension and well-being. Would these people truly be healthy? On an evolutionary definition, the answer is clear. No, they would not be.
While the above sections clarify the relevance of and justification for medicine’s role in extinction prevention, an additional rationale must be provided for why a new specialty in particular is needed. In this regard, new scientific and ethical knowledge informing health promotion requires deep understanding that often sparks specialization. For example, lifestyle medicine was formalized following discoveries that sedentary behavior, changes in diet and caloric intake, and social isolation negatively affect health. Additional examples of specialization include infectious disease and public health, which were fostered by discoveries linking disease to microorganisms and social structures, respectively. Research over the past 170 years has led to a number of discoveries that suggest that humanity’s extinction is possible, even inevitable (1-3, below), or that may actually unintentionally increase the probability that we will, in fact, go extinct (4-6, below), an understanding of which requires specialized knowledge.
The intent here is not to outline a near-term, direct chain of events that would cause extinction, but rather to provide an overview of issues that, in addition to climate change, are often cited as being relevant to evaluations of extinction risk. The breadth and depth of knowledge that these subjects span suggests that no single existing medical specialty provides the overall knowledge for making such assessments and, subsequently, intervening effectively.
A surgeon requires nearly a decade of training to be able to operate on patients, but, as of now, individuals working towards the explicit aim of protecting all of humanity from extinction require no training. This is unacceptable. Humanity needs specialists with knowledge vetted by experts who can dedicate themselves to extinction-related harm reduction and who can help other health professionals acquire basic skills in this domain without undue burden.
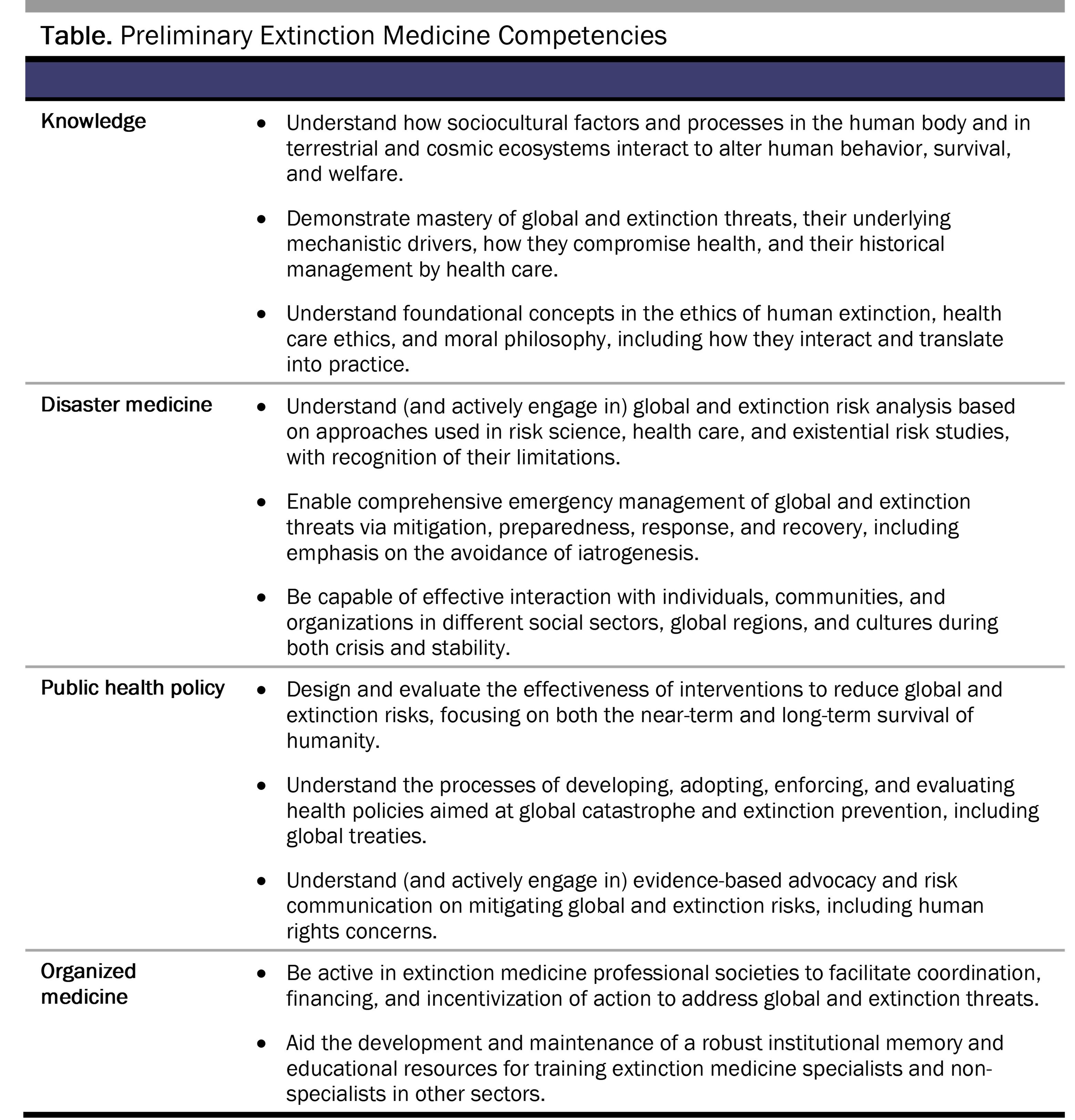
To benefit humanity, extinction medicine needs effective ways to translate knowledge into goal-directed action that would promote humanity’s survival while minimizing social harm. The table below lists competencies key to extinction medicine practice.
As a professional practice, extinction medicine’s core mission is to identify and execute actions that help all of humanity overcome environmental and moral challenges of collective survival. The need for this specialty, and what some of its actions might be, has briefly been explored above. But who, exactly, should become an extinction medicine specialist?
All health professionals, especially physician leaders, need to receive training in extinction medicine to some degree. For many physicians, it should be their “second specialty,” similar to disaster medicine.56 Interprofessional education (eg, in moral philosophy, social services, law, business, science, and engineering) would aid the success of extinction medicine and help embed it in society like other clinical specialties are today.
Extinction medicine, of course, does not exist. That needs to change. We must work together to raise awareness of the need for and concept of extinction medicine, to nurture an interest group, and to develop educational materials. Forming a specialty society, a code of ethics, a fellowship program, and an academic journal are examples of other important next steps. Through this work, health professionals can help prevent, delay, and promote a peaceful transition to humanity’s final sepulture: a universe without us—or even no universe at all.
Wyns A, Maiero M, Egorova A, Campbell-Lendrum D. COP26 Special Report on Climate Change and Health: The Health Argument for Climate Action. World Health Organization; 2021. Accessed April 28, 2025. https://iris.who.int/bitstream/handle/10665/346168/9789240036727-eng.pdf?sequence=1
Vohra K, Vodonos A, Schwartz J, Marais EA, Sulprizio MP, Mickley LJ. Global mortality from outdoor fine particle pollution generated by fossil fuel combustion: results from GEOS-Chem. Environ Res. 2021;195:110754.
Parncutt R. The human cost of anthropogenic global warming: semi-quantitative prediction and the 1,000-tonne rule. Front Psychol. 2019;10:2323.
Pearce JM, Parncutt R. Quantifying global greenhouse gas emissions in human deaths to guide energy policy. Energies. 2023;16(16):6074.
Tietjen B. Many of the world’s poorest countries are the least polluting but the most climate-vulnerable. Here’s what they want at COP27. PBS News. November 2, 2022. Accessed March 19, 2025. https://www.pbs.org/newshour/science/many-of-worlds-poorest-countries-are-the-least-polluting-but-the-most-climate-vulnerable-heres-what-they-want-at-cop27
Roelofs K. Freeze for action: neurobiological mechanisms in animal and human freezing. Philos Trans R Soc Lond B Biol Sci. 2017;372(1718):20160206.
Ord T. The Precipice: Existential Risk and the Future of Humanity. Hachette Books; 2020.
MacAskill W. What We Owe the Future. Basic Books; 2022.
Hallam R. Common Sense for the 21st Century: Only Nonviolent Rebellion Can Now Stop Climate Breakdown and Social Collapse. Chelsea Green Publishing; 2019.
Hales S, Kovats S, Lloyd S, Campbell-Lendrum D, eds. Quantitative Risk Assessment of the Effects of Climate Change on Selected Causes of Death, 2030s and 2050s. World Health Organization; 2014. Accessed February 3, 2025. https://iris.who.int/bitstream/handle/10665/134014/9789241507691_eng.pdf?sequence=1
Kemp L, Xu C, Depledge J, et al. Climate endgame: exploring catastrophic climate change scenarios. Proc Natl Acad Sci U S A. 2022;119(34):e2108146119.
Kemp L. Ecological breakdown and human extinction. In: Beard SJ, Rees MJ, Rios-Rojas C, Richards CE, eds. The Era of Global Risk: An Introduction to Existential Risk Studies. Open Book Publishers; 2024:147-172.
CO2 emissions in 2023. International Energy Agency. March 2024. Accessed April 29, 2025. https://www.iea.org/reports/co2-emissions-in-2023
Ágoston C, Csaba B, Nagy B, et al. Identifying types of eco-anxiety, eco-guilt, eco-grief, and eco-coping in a climate-sensitive population: a qualitative study. Int J Environ Res Public Health. 2022;19(4):2461.
Slovic P, Zionts D, Woods AK, Goodman R, Jinks D. Psychic numbing and mass atrocity. In: Shafir E, ed. The Behavioral Foundations of Public Policy. Princeton University Press; 2013:126-142.
Horton R, Beaglehole R, Bonita R, Raeburn J, McKee M, Wall S. From public to planetary health: a manifesto. Lancet. 2014;383(9920):847.
Futerman G. Beyond simple existential risk: survival in a complex interconnected world. Effective Altruism Forum. November 21, 2022. Accessed September 24, 2024. https://forum.effectivealtruism.org/posts/cXH2sG3taM5hKbiva/beyond-simple-existential-risk-survival-in-a-complex
Sepasspour R. A new “all-hazards” approach for reducing multiple catastrophic threats. Bulletin of the Atomic Scientists. November 24, 2023. Accessed February 3, 2025. https://thebulletin.org/2023/11/a-new-all-hazards-approach-for-reducing-multiple-catastrophic-threats/
Undheim TA. An interdisciplinary review of systemic risk factors leading up to existential risks. Prog Disaster Sci. 2024;22:100326.
Arnscheidt CW, Beard SJ, Hobson T, et al. Systemic contributions to global catastrophic risk. SocArXiv. July 8, 2024. Updated July 16, 2024. Accessed February 3, 2025. https://osf.io/preprints/socarxiv/wcj9e_v1
Sundaram L, Maas MM, Beard SJ. Seven questions for existential risk studies. SSRN. June 7, 2022. Accessed March 20, 2025. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4118618
Kellis DM, Torres ÉP. Extinction medicine: the case for a new medical specialty. SSRN. March 25, 2025. Accessed June 11, 2025. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5109482
Physicians for Social Responsibility. Accessed January 30, 2024. https://psr.org/
Schell J. The Fate of the Earth. Knopf; 1982.
von Hippel M. Vacuum of space to decay sooner than expected (but still not soon). Quanta Magazine. July 22, 2024. Accessed March 20, 2025. https://www.quantamagazine.org/vacuum-of-space-to-decay-sooner-than-expected-but-still-not-soon-20240722
Torres ÉP. Human Extinction: A History of the Science and Ethics of Annihilation. Routledge/Taylor & Francis Group; 2023.
Finneron-Burns E. What’s wrong with human extinction? Can J Philos. 2017;47(2-3):327-343.
Scheffler S. Why Worry About Future Generations? Oxford University Press; 2018.
Current health expenditure (% of GDP). World Bank Group. Accessed March 19, 2025. https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS
Minerals in the medical supply chain. National Mining Association. Accessed March 19, 2025. https://nma.org/minerals-in-the-medical-supply-chain/
Health-ISAC. The global risks of systemic reliance on critical mineral imports. Health-ISAC; 2024. Accessed March 19, 2025. https://www.aha.org/system/files/media/file/2024/10/tlp-white-the-global-risks-of-systemic-reliance-on-critical-mineral-imports-hisac-report-10-2024.pdf
H Rept 118-710: Recognizing the Importance of Critical Minerals in Healthcare Act of 2023, HR 6395, 118th Cong, 2d Sess (2023-2024). Accessed March 19, 2025. https://www.congress.gov/congressional-report/118th-congress/house-report/710/1
Karliner J, Slotterback S, Boyd R, Ashby B, Steele K. Health care’s climate footprint: how the health sector contributes to the global climate crisis and opportunities for action. Health Care Without Harm; ARUP; 2019. Accessed January 30, 2025. https://global.noharm.org/sites/default/files/documents-files/5961/HealthCaresClimateFootprint_092319.pdf
Yetunde PA, Harilall R, Mpotulo N, Robinson-Morris DW, Dibia YO. Ubuntu: I am because we are. Lion’s Roar. Accessed September 30, 2024. https://www.lionsroar.com/ubuntu-i-am-because-we-are/
Broadbent A. Philosophy of Medicine. Oxford University Press; 2019.
Mello FS, Friaça ACS. The end of life on Earth is not the end of the world: converging to an estimate of life span of the biosphere? Int J Astrobiol. 2020;19(1):25-42.
Mack K. The End of Everything (Astrophysically Speaking). Scribner; 2021.
Ord T. The edges of our universe. ArXiv. April 2, 2021. Updated May 5, 2021. Accessed March 20, 2205. https://arxiv.org/abs/2104.01191
Federspiel F, Mitchell R, Asokan A, Umana C, McCoy D. Threats by artificial intelligence to human health and human existence. BMJ Glob Health. 2023;8(5):e010435.
Sandbrink JB. Artificial intelligence and biological misuse: differentiating risks of language models and biological design tools. ArXiv. July 24, 2023. Updated December 23, 2023. Accessed February 3, 2025. https://arxiv.org/abs/2306.13952
What is the ABODM? American Board of Disaster Medicine. Accessed September 30, 2024. https://www.abpsus.org/american-board-of-disaster-medicine/

