Case and Commentary
Feb 2018
This essay considers the ethical problems raised by a scene of diagnosis presentation in Nate Powell’s graphic novel Swallow Me Whole, in which the patient is not only not engaged by the physician, but also effectively marginalized from the moment that her condition is named and medicalized. Put in the context of the book as a whole and in relationship to the unique affordances of the comics form, however, we see that though the physician made a correct diagnosis, the case did not end well due to the poor delivery of that diagnosis and the lack of support from members of the patient’s extended community.
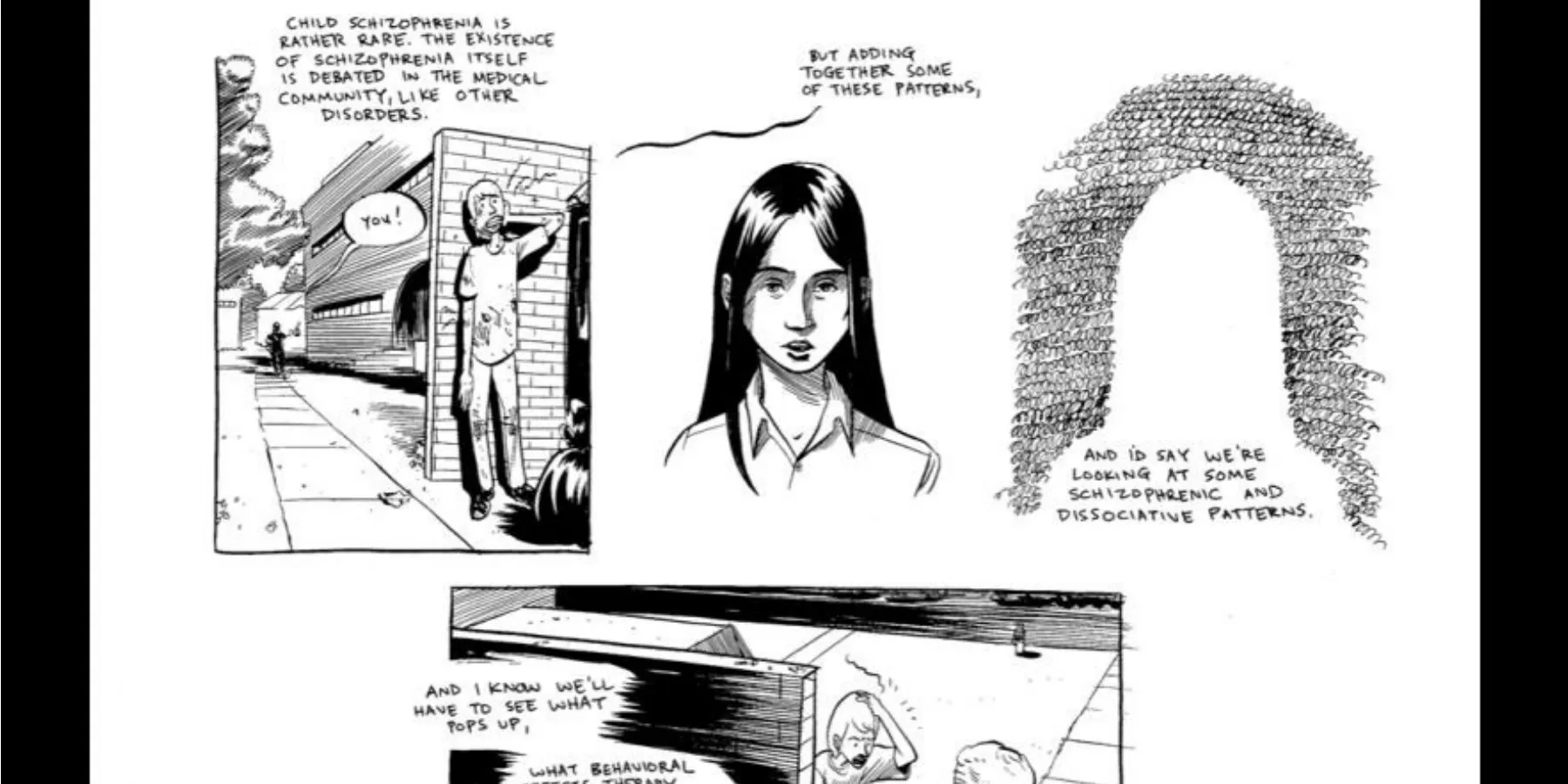
Ruth, a teenager with a family history of schizophrenia, has been seeing visions of insects. She has difficulty discerning reality from hallucinations, and her resulting inattention has been noticed by her parents. As depicted in the comic below, Ruth goes to see a psychiatrist who gives her the diagnosis of schizophrenia. The physician rambles about Ruth’s symptoms and the incidence of schizophrenia and finally provides a prescription, presumably for antipsychotics. Ruth does not engage in any discourse with her physician and ultimately disappears from the comic.
© 2008 Nate Powell. Reprinted by permission of Top Shelf Productions.
In the narrative case studies by which we judge the efficacy and ethicality of a clinical encounter, we often see staged clearly marked successes or failures—“good doc” versus “bad doc.” However, graphic narrative as a form of storytelling is not always well suited to such didactic lessons. One of its paradoxes is that, on the one hand, it relies on highly compressed and distilled language and images that create the illusion of transparency, while, on the other, it is so elliptical and marked by gaps that it opens up ambiguities that can only be resolved by the active engagement of the reader. All of this makes graphic narrative not only a challenging source of clinical case studies but also a potentially rich one.
Looking at this case we see evidence of a flawed scene of diagnosis in that the psychiatrist addresses himself to the mother, seemingly erasing the teenaged patient, Ruth, from her own care. However, we have every reason to believe the diagnosis and the prescribed treatment are appropriate. Further complicating our ethical engagement with this page, as we will see, is the fact that the narrative’s telling is interwoven with another scene involving Ruth’s stepbrother, Perry, whose own scene of diagnosis will further problematize attempts to draw from the text clear ethical judgments.
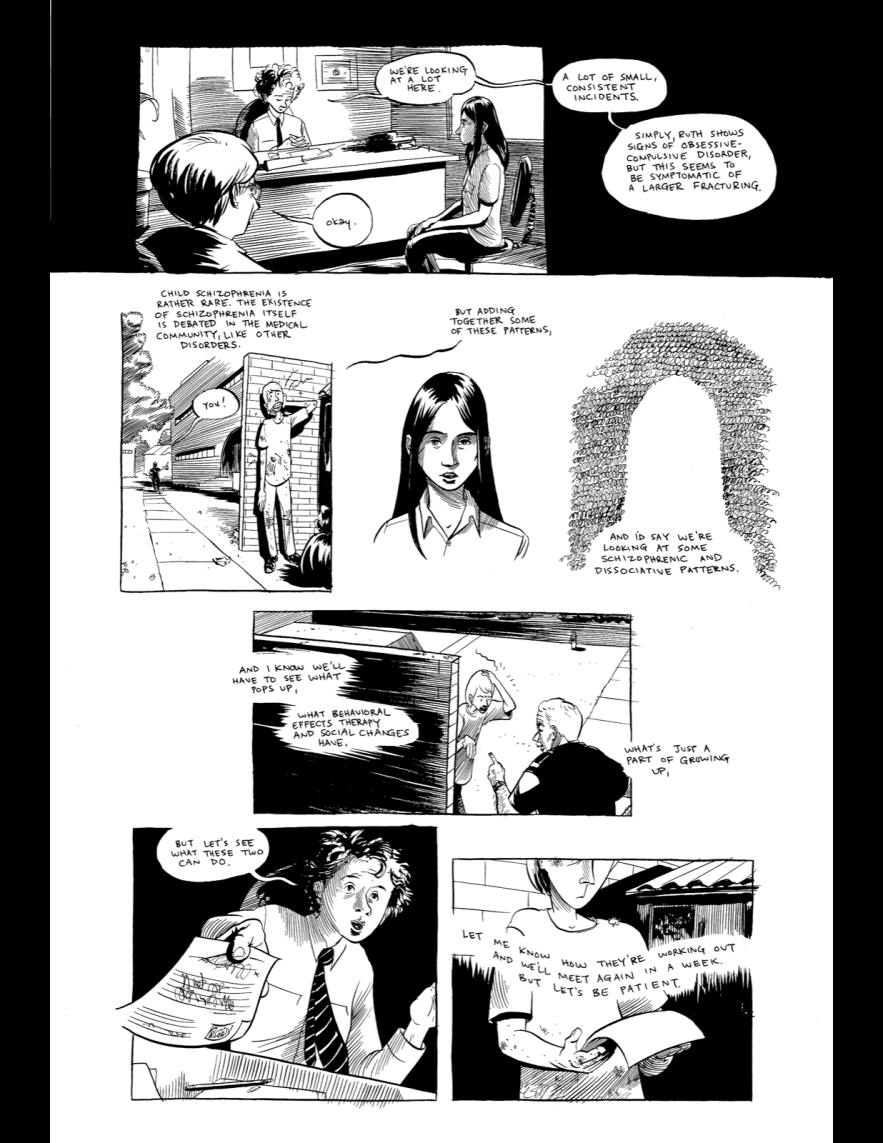
Swallow Me Whole [1] presents a case study by which to consider a scene of diagnosis that is at one and the same time a success and a failure. Here Ruth is being diagnosed by Dr. Newell following an oral history from the mother and a series of tests with Ruth herself. As readers who have had privileged subjective access to Ruth’s view of reality throughout the book, we have little reason to question the accuracy of the diagnosis of schizophrenia. Ruth has indeed been disassociating with increasing frequency, and her visions—dominated by swarms of cicadas invading interior spaces—have been getting stronger and more elaborate. We have seen, as well, evidence of her growing inability to communicate with family and peers. The diagnosis itself seems a reasonable one.
Nonetheless, we are encouraged to question the way in which the diagnosis is delivered. To begin with, Dr. Newell addresses his comments to the mother, despite the fact that Ruth is positioned appropriately in front of his desk. As he speaks of Ruth’s condition in the third person, we see a graphic representation of Ruth beginning once again to disassociate—first as the office dissolves behind her in a field of white and then as she herself dissolves into negative space while the clutter of ambient noise alone preserves the outline of her physical being. No evidence of eye contact with Ruth is visible on the page.
From this page alone, one might assume that Ruth has been completely noncommunicative, thus potentially justifying the behavior of the doctor. However, readers of the graphic novel will have seen Ruth regularly engage with adults even as the severity of her condition worsens, and she cooperated with Dr. Newell’s “performance tests,” answering all questions asked of her. There is in truth no explanation for the doctor’s failure to engage with the patient save that, in having made up his mind as to her condition, he has already written her off as an agent in her own recovery, turning all of his attention instead to the mother. The scene of naming—“some schizophrenic and dissociative patterns”—thus also becomes a scene of erasure.
It is also important to note that, even as the diagnosis continues to be delivered uninterrupted in the text of the page, three of the seven panels visually narrate a different space entirely, with actions playing out at the same time involving the second of the book’s protagonists, Ruth’s stepbrother Perry. We encounter Perry here after he has just escaped from a violent encounter with a school bully, only to now find himself challenged by a security guard. Like Ruth, Perry has experienced visions—in his case, of a small wizard who compels him to draw. When, a few pages later, Perry brings his concerns about his visions to his doctor, however, the scene plays out very differently than it had for Ruth. Here, the father is asked to leave and the physician, Dr. Connoly, addresses Perry directly, asking questions and making eye contact throughout. When Perry explains the compulsions brought on by his wizard, the doctor asks to see the drawings themselves and praises them. All of this seems to point towards the kind of effective and humanizing clinical interview we recognize as preferable to that performed by Dr. Newell.
In the end, however, the diagnostic encounter is not satisfactory for Perry. Dr. Connoly does take Perry’s art seriously, but he is dismissive of the concerns that brought him to the office in the first place, lightly suggesting that Perry himself is “clearly a wizard” and that “a few problems are always normal.” Dr. Newell had ceased to see Ruth as a human agent the minute he made up his mind regarding her diagnosis; conversely, Dr. Connoly’s confidence in Perry’s agency and the evidence of his artistic talent makes him unable to take seriously Perry’s concerns that he might be suffering from mental illness.
One last thing worth pointing out on the page of our case study: the “parallel editing” (to borrow film terminology)—by which we see Perry’s conflict with the bully interwoven with the narration of Ruth’s diagnosis—is not typical of Powell’s narrative approach elsewhere in the book. This is in fact the most extended example of such narration across two (presumably) simultaneously-occurring events in two (clearly) different spaces, extending over the full four pages from Ruth’s first meeting with Dr. Newell to the end of the page we have before us. When Perry is diagnosed (or fails to be diagnosed) a few pages later, there is no similar parallel editing, and the scene itself is laid out in a conventional nine-panel comics page grid. So why does Powell tell the story of Ruth’s diagnosis in a way that imbricates it from beginning to end with Perry’s fight with the bully (who originally targeted the siblings following one of Ruth’s first public psychotic episodes)?
I would argue that Powell wishes us to recognize the degree to which Ruth’s understanding of her illness is inextricable from her relationship with her stepbrother. As the biographical note to the book tells us, Powell worked with adults with developmental disabilities [1], and from that experience he knows well that no illness is ever just between doctor and patient. The collaborative nature of graphic narrative discussed earlier—in which readers must actively participate in the process of meaning making—makes the form well-suited to modeling “networked” narrative medicine—an approach to caring for a patient that extends beyond the patient-physicians relationship to include family, teachers, employers, authority figures (like the security guard), and so on. And, in these terms, we might understand that while Dr. Newell’s failure to address Ruth during her diagnosis is far from ideal, his inclusion of the mother in the scene of the diagnosis is appropriate both because of Ruth’s status as a minor and because the illness itself will require active collaboration and education on the part of family, teachers, employers, and so on. When things go wrong for Ruth at the book’s end, it is because parents, teachers, and employers failed in their responsibilities as informed caretakers, not because of Dr. Newell’s delivery of the diagnosis.
The fact that we see the events befalling Perry—his encounter with a bully and a security guard—simultaneously with Ruth’s diagnosis, in fact, could be read as suggesting the ways in which their conditions are interwoven in ways Ruth recognizes but her family will not. In these terms, it is worth noting that while Dr. Newell erases Ruth by focusing all of his responses entirely on the mother, Dr. Connoly pushes the father out of the room and focuses all of his attention on Perry in isolation. In the end, neither of these extremes proves effective. A differently staged diagnosis would not necessarily have led to a better outcome for Ruth, as long as parents, teachers, employers, and classmates misread and misjudged her behavior and silenced her more effectively than Dr. Newell ever could. In the end, Dr. Newell might well have been right (even if for entirely wrong reasons) to focus his energies on the mother as opposed to Ruth, given that the adults in Ruth’s life needed the education more urgently than she did. Unfortunately, the lessons did not take, and Ruth ends up erased once and for all from her own experience.
Powell N. Swallow Me Whole. Marietta, GA: Top Shelf Productions; 2008.



