Art of Medicine
Jun 2013

Although health care practitioners rely upon all of their senses—give or take taste, perhaps—to engage with patients and gather information, sight holds a special place above the rest. Medicine is a highly visual field. Caregivers at all levels and scopes of practice rely upon their sight to perform their work, not only to observe patients and render care, but also to engage with technologies and colleagues. Because of the growth of clinics and hospitals from individual and small-group practices to large networks with legions of providers, it has become more likely for doctors, nurses, and other members of care teams not to recognize one another in their working environments. Thus, many hospitals and other care systems institute uniforms to help visually distinguish employees. The color of a person’s scrubs, for example, might indicate a nurse or an imaging technician.
Such distinctions are not entirely recent inventions. Physicians have been distinguished by their long white lab coats since the nineteenth century, when such attire was adopted by the medical profession in keeping with the paradigm of the physician-as-scientist. It is no accident that the ceremony that most often serves to mark the beginning of medical training is referred to by many institutions as the “white coat ceremony,” during which students receive their first lab coats. These coats are cropped to the waist; students do not receive the longer lab coats worn by physicians until they earn their medical degrees.
Patients, for their part, have their own responses to medical garb. In fact, some instances of hypertension during office visits that are not reproduced by at-home measurements are chalked up to “white coat syndrome”—a visceral response to the presence of clinical practitioners that is quantifiable in vital signs and often brought on by anxiety. Even so, many patients still enter clinics and hospitals with the expectation that they will see a doctor in a lab coat. Today, many nurse practitioners and physician assistants choose to wear a long white coat while seeing patients as well. Few patients recognize that other caregivers might wear such coats, or that doctors might eschew them.
Without medical garb specific to role and position, the burden falls on individual practitioners to introduce themselves clearly to their patients and ensure that their place in the care team is understood. Patients’ right to know who is rendering their care and treatment stems naturally from their right to self-determination, much like their right to informed consent. Ensuring that patients understand these caregivers’ scope of practice further honors that right.
Likewise, clinicians should be made aware of their colleagues’ roles in patient care. In care settings where medical garb is not differentiated, communicating this information may present challenges to the expediency and efficiency of action, particularly when critical or urgent care is being administered. However, visual distinctions between health care professionals have their own drawbacks, insofar as reinforcing the differences between team members can easily reinforce overly rigid role divisions and hierarchical inequities that undermine true teamwork.
A tension has developed between the garment’s role as a sign of status and profession and its use in denoting the separation between physicians and their patients and among different health professionals. In figure A, a scene from a nineteenth-century operating theater establishes contrasts between the garments of the doctor, nurse, student, and patient. Students and observers sit in darkness, clad in black. Light is cast over the main event, the operation on the patient, whose breast is exposed for the surgery, conveying the vulnerability of her condition. The professor stands aside, garbed in white along with his surgical assistants, directing the proceedings. The nurse is distinct in her bonnet and apron, wearing both white and black. In addition to the statement this image makes about the historically gendered place of nurses in medicine, the nurse’s clothing in this painting uniquely situates her in a liminal space, possessing the visual cues of both the learned and the learners. Roles are clearly defined and represented here, and a classical hierarchy is established in this scene.
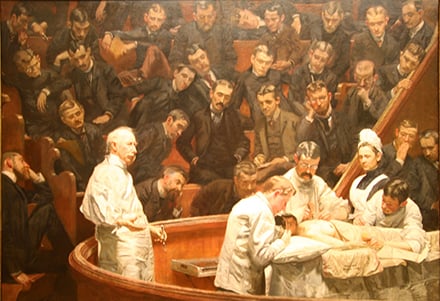
Figure A.
Thomas C. Eakins (1844-1916)
The Agnew Clinic, Portrait of David Hayes Agnew
1889
Oil on canvas, 74 1/2 x 130 1/2 inches
The University of Pennsylvania School of Medicine, Philadelphia, PA (Click the magnifier to enlarge image.)
Figure B shows a nurse tending to the wounds of soldiers in an English military hospital. This portrait feels far more intimate, an expression of the closeness between nurse and patient. Once again, the nurse is wearing the bonnet and apron as she carefully bandages the young man’s arm. In this painting, physicians are not visible, but another type of uniformed caregiver is: the priest at the left hand side of the painting. The entire mood of the work is informal—no bedside rounds, patients walking along the hallway, a family member reading the paper—and makes a statement on the role of the nurse as a comforting presence more than an imposing figure, closer to patients than to physicians in the hierarchical structure.

Figure B.
Sir John Lavery (1856-1941)
The First Wounded
1914-19
litho
Dundee Art Gallery and Museum (Click the magnifier to enlarge image.)
Figure C presents a more formally composed, haunting style and atmosphere when compared with the warmth of the previous image. It appears that the condition of the patient in this painting is more serious. Once again, the doctors in white are presiding over the scene while the nurses, in blue dress, are actually touching the patient, in both the fore- and background. Nurses’ and physicians’ garb is starkly differentiated and immediately identifiable, while their roles within the context of the work seem to be delineated such that doctors ruminate over care that nurses subsequently deliver. The closeness of nurses to the patients in all three of these images helps to illustrate how caregivers may be subject to hierarchical inequity in their professional relations.
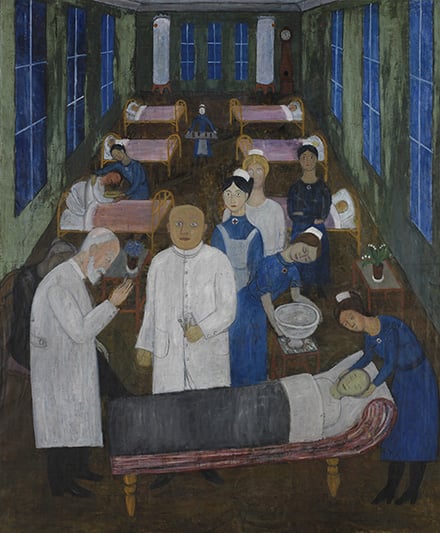
Figure C.
Hilding Linnqvist
Hospital Ward II
1920
Moderna Museet, Stockholm
Photograph © Moderna Museet, Stockholm (Click the magnifier to enlarge image.)
The resolution of this tension between the utility of medical garb and its potential consequences for workplace dynamics lies not in the reduction of visual distinctions between caregiver roles, but rather in the establishment of better interprofessional understanding and respect through new forms of training and educational interventions. The World Health Organization has advocated for improved interprofessional teamwork in health care since 1978, and multiple reports have been issued since that time to reaffirm the importance of interprofessionalism with evidence of its efficacy for patient benefit [1-3]. A review of the literature indicates that the delivery of patient care improves among those who complete interprofessional training [4], most likely because of the impact of subtle prejudices and preconceptions on teamwork and collaboration among professionals who have not had such training [5]. Although students’ professional identities may be well established before training in a medical profession even begins [3], educational interventions demonstrably reduce the formation of negative stereotypes between student groups [6].
The Liaison Committee on Medical Education has recommended for more than a decade that medical students receive training in professional communication [7], but recent analysis of curricula prepared for accreditation indicates that change has been slow with respect to the adoption of interprofessional training methods with measures of student performance [8]. Until more students are encouraged to build effective strategies for teamwork and communication across disciplinary divides, the sense will remain that elements of the care setting like medical garb that differentiates between practitioners reinforces inequitable hierarchies rather than facilitating collaboration.
By allowing care providers to readily recognize one another in the clinical setting, visual codes of medical garb solve more problems than they generate. If medical garb currently reinforces a hierarchical barrier in the clinic, then it is a failure of interprofessional training in collaborative medical practice, not an indictment of the utility of role differentiation. Effective teamwork relies as much upon a foundation of understanding team members’ roles as it does on mutual respect and open communication.
World Health Organization. Learning to Work Together for Health: Report of a WHO Study Group on Multiprofessional Education Of Health Personnel: The Team Approach. Geneva: World Health Organization; 1988: 769.
World Health Organization. Primary Health Care: Report of the International Conference on Primary Health Care. Geneva: World Health Organization; 1978.
Zwarenstein M, Reeves S, Perrier L. Effectiveness of pre-licensure interprofessional education and post-licensure collaborative interventions. J Interprof Care. 2005;19 Suppl 1:148-165.
Pirie P. Evaluating community health promotion programs. In: Bracht N, ed. Health Promotion at the Community Level: New Advances. London: Sage Publications; 1999.
Liaison Committee on Medical Education. Functions and Structure of a Medical School. Washington, DC: Liaison Committee on Medical Education; 1998.