In the Literature
Jun 2023
Peer-Reviewed

Body mass index (BMI) cutoffs are routinely used to assess eligibility for gender-affirming surgeries (GAS), yet they are not empirically based. The transgender population is disproportionately affected by overweight and obesity due to clinical and psychosocial influences on body size. Strict BMI requirements for GAS are likely to cause harm by delaying care or denying patients the benefits of GAS. A patient-centered approach to assessing GAS eligibility with respect to BMI would utilize reliable predictors of surgical outcomes specific to each gender-affirming surgery, include measures of body composition and body fat distribution rather than BMI alone, center on the patient’s desired body size, and emphasize collaboration and support if the patient genuinely desires weight loss.
The number of transgender patients seeking gender-affirming surgery (GAS) has dramatically increased in recent years.1 Body mass index (BMI) cutoffs are routinely used to assess eligibility for GAS due to concerns about adverse surgical outcomes.2,3,4 Results from the National Surgical Quality Improvement Program revealed that the effect of BMI on surgical outcomes presents the greatest risk to patients with morbid obesity (BMI ≥ 40). Commonly cited concerns include increased risk of surgical site infection; cardiovascular risks, such as cardiac arrest and myocardial infarction; and pulmonary complications, such as pneumonia, reintubation, and prolonged ventilator support.5,6
Risks associated with delaying or denying access to GAS are also salient. Gender-affirming medical interventions, including hormone therapy (HT) and GAS, are associated with improved quality of life and decreased levels of anxiety, depression, gender dysphoria, and suicidal ideation.7,8,9 The eighth version of the World Professional Association of Transgender Health guidelines characterize GAS as “medically necessary” for some patients to alleviate gender dysphoria.10 Thus, surgeons must consider not only the risks of the surgery itself, but also the risks to a patient’s health and well-being when GAS are delayed or denied.
The purposes of this article are (1) to review the existing research on BMI as a predictor of GAS outcomes using a mapping review; (2) to discuss weight disparities among the transgender population; and (3) to advance discussion of how to evaluate patients’ eligibility for GAS with particular attention to their body size in light of calls for a “multimodal, human-centered approach” to addressing risk factors for GAS.2
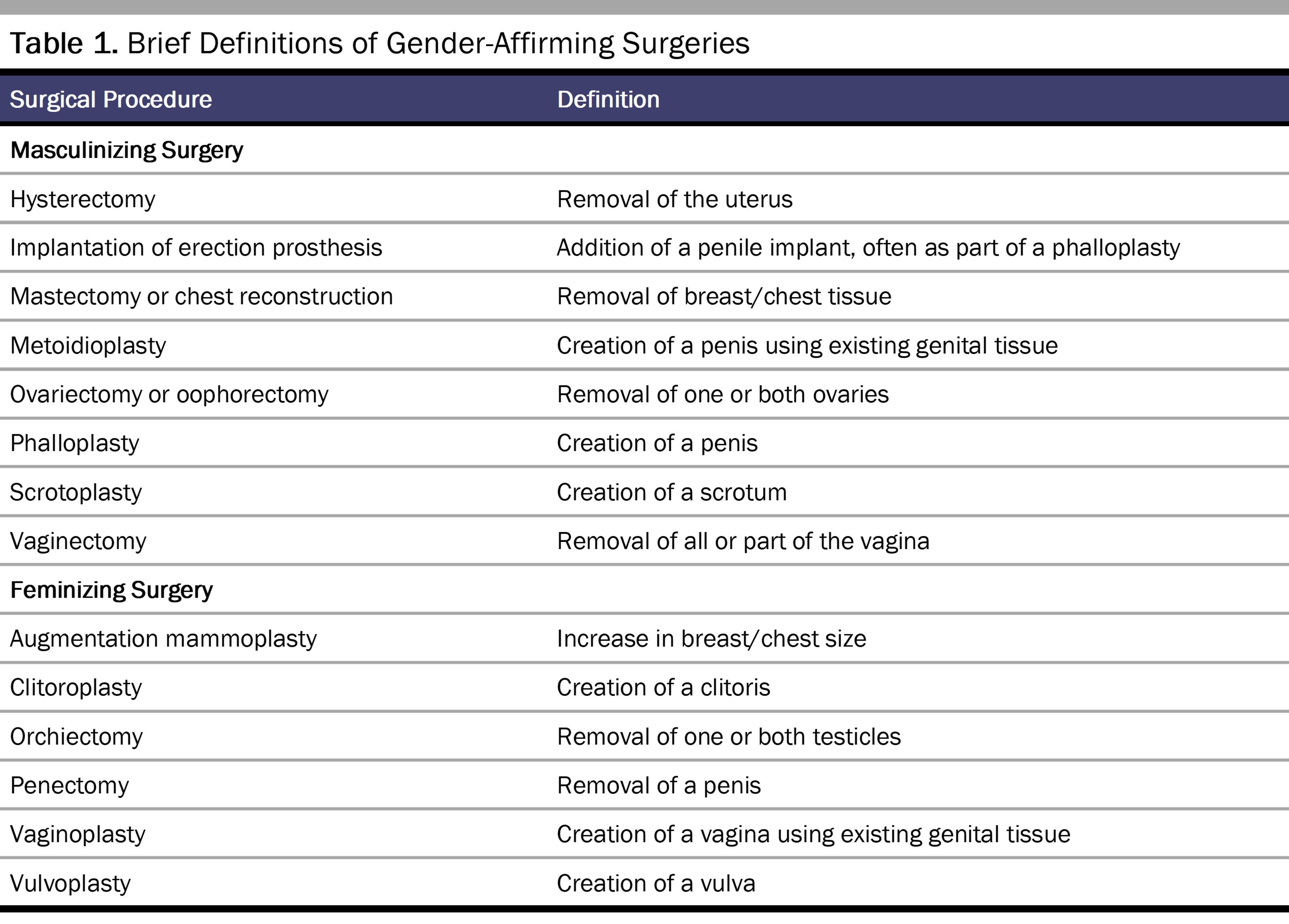
Table 1 provides brief definitions of various chest and genital GAS.
To review existing research on BMI as a predictor of GAS outcomes, we conducted a mapping review of the available literature published through July 1, 2022. A mapping review is ideal to categorize existing literature, identify gaps, and guide further research.11 We searched the Scopus database using queries with keywords: the name of the surgical procedure (eg, mastectomy) AND body mass index OR obesity OR body weight AND transgender. Studies were screened to remove those that reported BMI or weight status in the sample population but did not evaluate the role of BMI in predicting GAS outcomes.
Table 2 presents a summary of the articles retrieved from our search. In total, 11 studies explored the role of BMI in predicting chest and genital GAS outcomes.
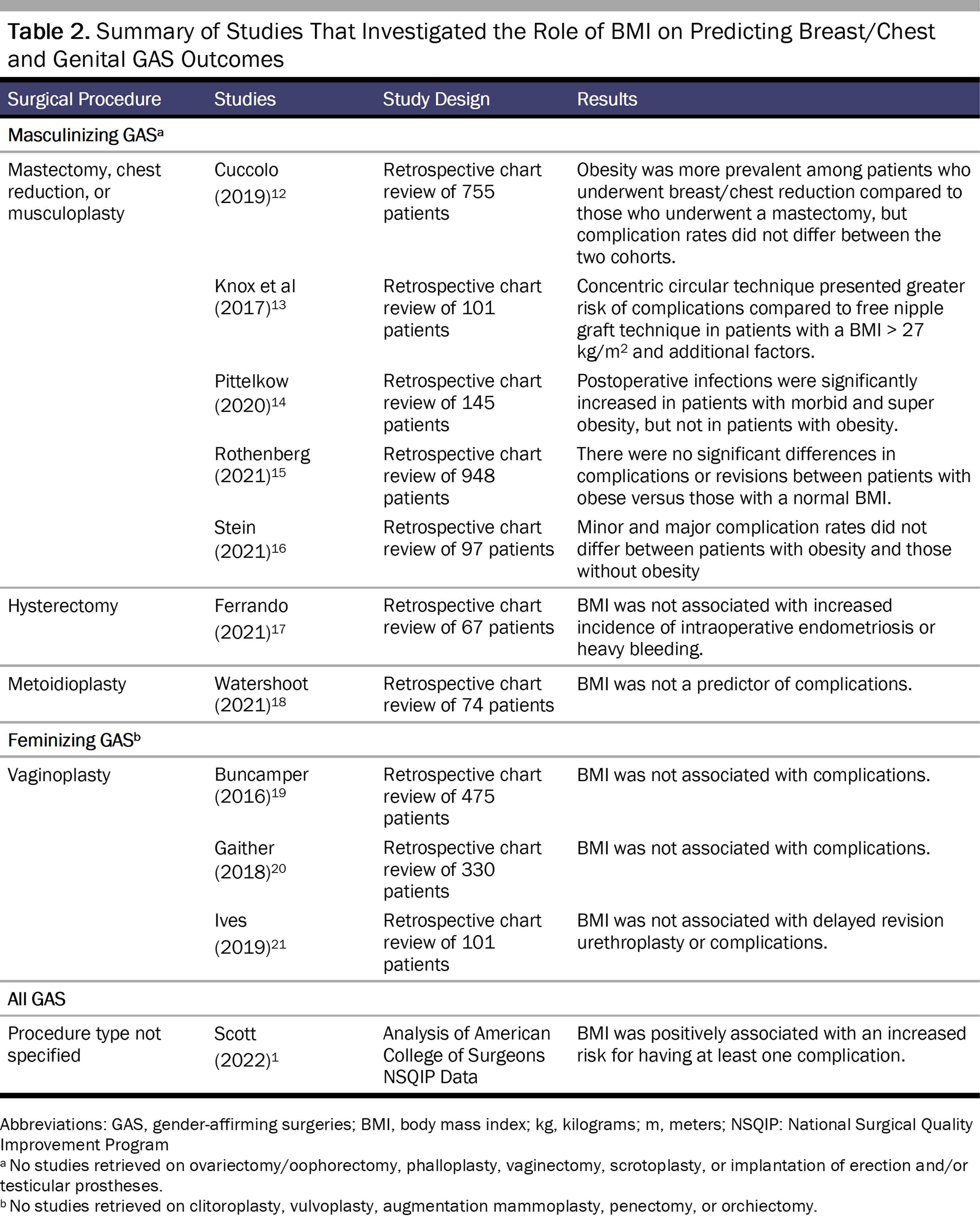
Five studies focused on masculinizing chest surgeries, such as mastectomy, breast reduction, or musculoplasty.12,13,14,15,16 An obese BMI (≥ 30) did not increase the risk of complications in 4 of the 5 chest reconstruction studies.12,14,15,16 Pittelkow et al found that postoperative infection risk was higher in mastectomy patients with morbid obesity (BMI ≥ 40) and super obesity (BMI ≥ 50).14 BMI was not associated with complications in studies of hysterectomy,17 metoidioplasty,18 and vaginoplasty.19,20,21 Among all forms of gender-affirming surgery, BMI was associated with a very slight increased risk for complications in Scott et al’s study that relied on American College of Surgeons National Surgical Quality Improvement Program data, although the findings were not reported by BMI classification, type of gender-affirming surgery, or the nature of the complication.1
The studies identified in this literature review have several limitations. Because existing research is limited to 4 common GAS, future research should address BMI as a predictor of outcomes in all forms of gender-affirming surgery. A second limitation is that because BMI cutoffs were routinely used to determine GAS eligibility when some of the studies were performed,2,4 patients with higher classes of obesity might not have been included in the study samples. Thus, further research should explore BMI as a predictor of GAS outcomes in patients with class I, II, and III obesity, similar to the work of Rothenberg et al15 and Pittelkow et al,14 and in patients with an underweight BMI (< 18.5).
A patient-centered approach to evaluating GAS eligibility with respect to BMI requires consideration of multiple influences on body weight and obesity risk. Transgender individuals are more likely to be affected by overweight and obesity than nontransgender individuals secondary to clinical and psychosocial factors.22,23,24,25 For example, masculinizing and feminizing HT result in estimated increases in body weight of 1.7 kg and 1.8 kg, respectively,26 with case reports of up to 27.3 kg of weight gain.27 Anticipated weight gain with HT increases the likelihood that a patient’s BMI would exceed predetermined limits for GAS. In addition, the transgender population is disproportionately affected by nutrition-related conditions, such as food insecurity and eating disorders,28,29,30,31,32 both of which are associated with an increased obesity risk in certain population groups.33,34,35 The transgender population is also significantly less physically active than the cisgender population due to fear of being “outed” as transgender, “passing” as male or female, and body dissatisfaction, among other factors.36,37,38,40,41,42,43,44 Although obesity is a complex disease, physical inactivity is a known risk factor.25
Although the terms obese and obesity have been used throughout this paper when describing the results of existing research reliant on Centers for Disease Control and Prevention BMI ranges, we recognize that obesity as a medical diagnosis lacks sensitivity to body size diversity. Strict BMI requirements for GAS and routine weight loss recommendations also neglect a fundamental consideration: the patient’s own desire for their body size. The hegemonic assumption is that all patients desire a body size that is within the “healthy” BMI range of 18.5-24.9 as defined by the Centers for Disease Control and Prevention,39 despite the known limitations of BMI as a predictor of adiposity and health outcomes.45 Whether the patient with a BMI classified as overweight or obese genuinely desires a smaller body size, however, is not routinely considered. Notably, the patient’s desire for their own body size does not change the risks associated with GAS, but it is relevant to the provision of patient-centered care.
Body size and shape may be an expression of a patient’s authentic gender identity. The first author (W.L.) and a colleague have related the narrative of a transgender man who genuinely desired a larger body size—which he described as “having more of a presence,” “filling out my space,” and “going from invisible to visible”—when he decided to transition.46 Although clinicians would label his body as obese, his larger body size was an expression of his masculinity.46 Importantly, emerging research suggests that prescribing weight loss for patients seeking GAS is not only ineffective but also may cause harm by propagating weight cycling and weight stigma.2,47 Thus, while many patients with overweight or obesity may genuinely desire a smaller body size, the reflexive assumption that all patients are dissatisfied with their body size lacks sensitivity to patients’ goals and gender expression.
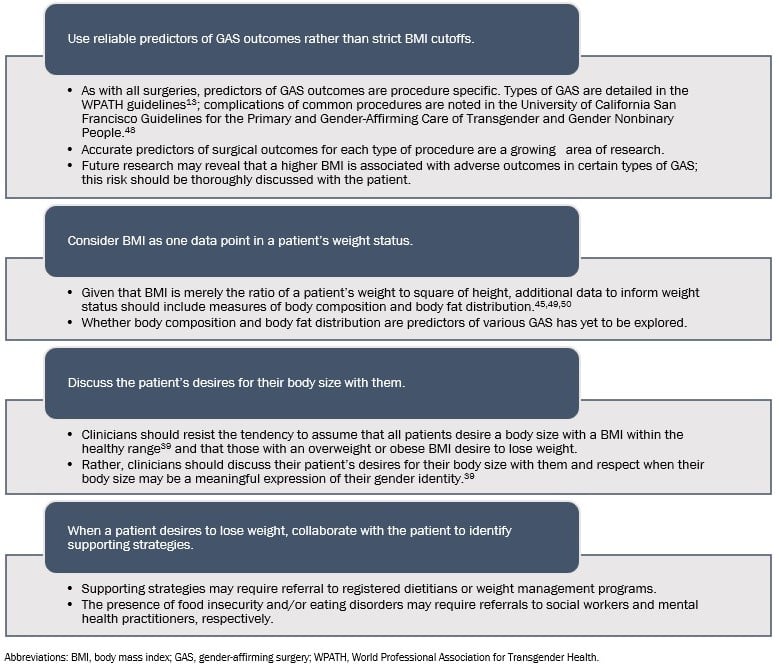
A patient-centered approach to assessing GAS eligibility with respect to BMI would be empirically driven and center on the patient’s goals for their body. Toward this end, clinicians can employ the strategies depicted in the Figure.
Figure. Patient-Centered Approach to Use of Body Mass Index in Evaluating Gender-Affirming Surgery Eligibility
The use of BMI cutoffs to determine GAS eligibility is an oversimplified and unsubstantiated practice. Given that transgender individuals are disproportionately affected by obesity, strict BMI requirements for GAS are likely to harm a significant number of patients by delaying or denying the benefits of GAS. A patient-centered approach to assessing GAS eligibility with respect to BMI would utilize reliable predictors of surgical outcomes specific to each gender-affirming surgery, include measures of body composition and body fat distribution rather than BMI alone, center on the patient’s desires for their body size, and emphasize collaboration and support if the patient genuinely desires weight loss. Further research is needed to determine reliable predictors of various GAS.
Rothenberg KA, Gologorsky RC, Hojilla JC, Cohan CM, Beattie G, Yokoo KM. Gender-affirming mastectomy in transmasculine patients: does obesity increase complications or revisions? Ann Plast Surg. 2021;87(1):24-30.
Stein JM, Grigor E, Hardy J, Jarmuske M. Surgical and patient-reported outcomes following double incision and free nipple grafting for female to male gender affirmation: does obesity make a difference? J Plast Reconstr Aesthet Surg. 2021;74(8):1743-1751.
Ives GC, Rein LA, Finch L, et al. Evaluation of BMI as a risk factor for complications following gender-affirming penile inversion vaginoplasty. Plast Reconstr Surg Glob Open. 2019;13(7):e2097.
Causes of obesity. Centers for Disease Control and Prevention. Updated March 21, 2022. Accessed July 5, 2022. https://www.cdc.gov/obesity/basics/causes.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fobesity%2Fadult%2Fcauses.html
Conron KJ, O’Neill KK. Food insufficiency among transgender adults during the COVID-19 pandemic. Williams Institute, UCLA School of Law; 2022. Accessed July 5, 2022. https://williamsinstitute.law.ucla.edu/wp-content/uploads/Trans-Food-Insufficiency-Update-Apr-2022.pdf
Parker LL, Harriger JA. Eating disorders and disordered eating behaviors in the LGBT population: a review of the literature. J Eat Disord. 2020;8:1-20.
Simone M, Hazzard VM, Askew AJ, Tebbe EA, Lipson SK, Pisetsky EM. Variability in eating disorder risk and diagnosis in transgender and gender diverse college students. Ann Epidemiol. 2022;70:53-60.
Hernandez DC, Reesor LM, Murillo R. Food insecurity and adult overweight/obesity: gender and race/ethnic disparities. Appetite. 2017;117:373-378.
About adult BMI. Centers for Disease Control and Prevention. Reviewed June 3, 2022. Accessed June 30, 2022. https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html#Used
Linsenmeyer W, Coffey M. “Going from invisible to visible”: challenging the “normal” ranges, cut-offs and labels used to describe the sizes and shapes of transgender and gender diverse bodies. In: Joy P, Aston M, eds. Queering Dietetics. Routledge. Forthcoming 2022.
Deutsch MB, ed. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People. 2nd ed. University of California San Francisco Gender Affirming Health Program; 2016. Accessed July 5, 2022. https://transcare.ucsf.edu/guidelines