Case and Commentary
Aug 2024
Peer-Reviewed

Undocumented people in the United States face innumerable legal and structural barriers to health and health care services, including for kidney failure. Their experiences vary across states and regions due to wide variation in insurance coverage and unreliable access to health-promoting resources, including medical-legal partnerships. This commentary on a case canvasses key policy about structural and legal determinants of health for undocumented persons.
In the emergency department (ED) of a large, urban academic health center near the US-Mexico border, Dr B encounters GG, who presents with severe fatigue, headache, dysuria (painful urination), and aching joints. After GG is stabilized, metabolic tests reveal that GG has kidney failure. Dr B refers GG immediately for emergency dialysis and then routine dialysis follow-up. However, due to GG’s immigration status, the state’s Medicaid program does not reimburse for routine dialysis, only for emergency dialysis.
Three weeks later, Dr B gets called back to the ED because GG is back with severe life-threatening symptoms (hyperkalemia, confusion, and hypoxia from pulmonary edema) due to lack of routine dialysis. Dr B is morally distressed and outraged that he has had to witness GG’s symptoms become life-threatening due to the state Medicaid program’s lack of coverage for optimal kidney care (eg, routine dialysis).
Dr B thinks, “My patient needs a lawyer,” and wonders what to do.
Clinicians’ moral distress stemming from their inability to provide optimal care for individuals like GG and questions regarding how to improve care for undocumented individuals have generated critical national discourse, investigation, and equity-enhancing policy reform related to caring for undocumented people with kidney disease. Over 2 decades of studies have documented the extensive, multilevel harm and financial cost associated with emergency-only dialysis for individuals with kidney failure.1,2,3,4,5,6,7 Compared to individuals receiving routine hemodialysis, those who rely on emergency dialysis experience an almost 5-fold greater hazard of 1-year mortality8 and a 14-fold greater hazard of 5-year mortality.9 Patients and their caregivers describe substantial morbidity and symptoms related to emergency dialysis treatments, including death anxiety and caregiver stress related to finances, care navigation, and emotional distress, which have multigenerational impacts.4,6,10 Primary care clinicians and emergency medicine and nephrology specialists also describe substantial moral distress related to providing emergency-only dialysis: witnessing suffering among individuals who have inadequate treatments, needing to balance ethics and laws, and experiencing discordance with principles of ethics that underlie medical training.4,9,11,12,13
Calls for evidence-based analyses to assess the cost effectiveness of and outcomes associated with a shift from emergency-only to routine dialysis for undocumented immigrants have been answered with rigorous qualitative and quantitative studies spanning a decade.14 Some studies demonstrate the morbidity, mortality, social, and economic benefits of comprehensive kidney care options, including transplantation.14 Other studies report reduction in mortality, emergency department visits, hospitalizations, and length of stay with routine dialysis compared to emergency-only dialysis.8,9 In a study of individuals who transitioned from emergency to routine dialysis in Colorado, patients reported significant improvement in quality of life and multiple symptoms, including anxiety, depression, pain, and dyspnea.15 In Colorado, emergency dialysis expenditures for undocumented immigrants averaged over $20 000 per person per month from 2017 until 2019, when a policy change that included kidney failure as a qualifying condition for emergency Medicaid (EM) went into effect, lowering routine dialysis expenditures for undocumented immigrants to an average of $5574 per person per month in 2021 and saving the state nearly $15 000 per person per month.5 A cohort study from California demonstrated that kidney transplant outcomes among undocumented immigrants were not inferior to those of US residents,16 thereby debunking myths regarding risk of kidney transplantation among undocumented individuals, who account for a substantially greater proportion of kidney donors (8% to 10%) than recipients (1%).17,18,19
In light of these findings, we provide a roadmap for clinician empowerment and action, which begins with a broadened understanding of the legal and regulatory context in which undocumented individuals like GG receive kidney care. We also describe policies that have been leveraged to ensure more comprehensive care for undocumented individuals and opportunities to enhance care through policy advocacy and structurally competent practice.
Providing optimal care for GG and other undocumented immigrants requires recognizing the barriers they face in receiving high-quality care and the patchwork of legal environments and state-specific policies that shape the landscape in which health care is delivered. Each of these factors exerts a unique influence on undocumented individuals’ health and sociopolitical experiences and their health care resources—from primary care to subspecialty care, including dialysis for kidney failure.1,2,13,20,21,22,23,24,25 The Personal Responsibility and Work Opportunity Act of 1996 (PWORA) is cited along with numerous associated restrictive federal policies as a foundational structural barrier for undocumented individuals due to explicit provisions restricting such individuals from accessing federal benefits, including health care programs and assistance programs such as Medicaid and Medicare.25,26,27
Post-PWORA, several states took steps to maintain certain undocumented individuals’ eligibility for health benefits through a court-created eligibility category known as Permanently Residing Under Color of Law (PRUCOL). Those states include New York, California, Connecticut, Hawaii, Illinois, Massachusetts, and Virginia.28 Although benefits vary by state, many offer comprehensive health insurance coverage that mimics Medicaid. For instance, in New York, certain undocumented individuals may be designated as PRUCOL under the state’s health code for the purpose of health insurance eligibility.29 Not to be confused with a lawful immigration status, PRUCOL designation does, for many, confer long-term eligibility for means-tested benefits (ie, adjusted based on gross income), such as state Medicaid. In short, the patchwork of legal environments and state-specific policies provides an impetus for policy makers, advocates, and health care practitioners to consider state and federal policies that can provide overarching protections for individuals regardless of the states in which they reside.21,22,24,25
Despite challenges posed by PWORA and other restrictive policies, legal precedent exists to ensure that undocumented immigrants in the United States have access to critical emergency care.7,8,13,29 The 1986 Emergency Medical Treatment and Labor Act (EMTALA) is a key legal provision by which hospitals are required to screen, stabilize, and treat patients found to have an emergency, regardless of immigration status. EM, which reimburses treatment of emergency medical conditions for individuals who are uninsured and excluded from regular Medicaid due to immigration status, also offers a critical lever to expand coverage for undocumented individuals. However, the Centers for Medicare and Medicaid Services (CMS), as affirmed by the Office of the Inspector General, allows states to determine the level of reimbursement and qualification for emergency medical services.5,27 Therefore, CMS’ deference to states’ interpretations of emergency medical conditions and services under EM gives clinician advocates and policy makers a critical policy lever for expanding access to health care for undocumented immigrants.27 EM supplements to state budgets have been described as critical subsidies for promoting innovation in undocumented immigrant health insurance coverage and overall population and public health.27 For instance, Medicaid policy in California offers a path to kidney transplantation for undocumented immigrants via Medi-Cal, which provides immune suppression coverage for individuals who meet specific criteria.1,16 California’s passage of Senate Bill 104 in 2019 extended eligibility for full-scope Medi-Cal benefits to undocumented youth aged 19 to 25 years regardless of PRUCOL status (with a further extension to adults aged 50 years and older in 2022 and to adults of any age in 2024),23,30 and other states have similarly leveraged Medicaid as a path to expand transplant access.31 Dr B could consider the state-specific coverage restrictions that exist for GG and work with local and national organizations to advocate for state-specific Medicaid and other policy changes that would expand coverage for routine hemodialysis, potentially further supporting Colorado’s demonstration of the overall economic and health benefits of this approach.
Improving care for GG also requires organizational and individual action to recognize—and to advocate against—threats to equity-enhancing policies or programs related to immigration. One salient example is threats to the Deferred Action for Childhood Arrivals (DACA) program, created by an executive order in 2012, which protects eligible undocumented immigrants who were brought to the United States as children from deportation and grants work authorization.32 Multiple studies demonstrate positive short-term outcomes for DACA recipients, including decreased delays in health care utilization and improved self-reported mental health outcomes.32,33 However, ongoing threats to DACA (eg, Texas v United States, in which the federal Fifth Circuit Court of Appeals ruled that DACA is unlawful and barred new applicants34) and newer, evolving state-level restrictions (eg, SB 1718 in Florida, which requires Medicaid-accepting hospitals in Florida to inquire about immigration status35) are examples of policies that cause profound social, health-related, and economic harm due to delayed presentations for care and subsequent costs to individuals and health systems.
The legal status and categories of undocumented immigrants add complexity to the structural barriers facing undocumented individuals—including their eligibility for asylum status and other immigration status designations, which impacts their care trajectories and eligibility for state-specific benefits, including transplantation.27 Increasingly, restrictive border policies have ripple effects in immigrant communities, including by limiting an individual’s ability to seek asylum at the border or apply for asylum once inside the United States.36 Undocumented individuals also live in diverse communities with pro- or anti-immigrant climates. For instance, in some California counties, investigators found mismatches between community needs and state services and resources, as well as resistance of local law enforcement agencies and policy makers to the state’s inclusive policy goals.37 Clinicians like Dr B and organizations should remain vigilant about threats to these inclusive policies and ensure that patients, their caregivers, advocates, and community organizations are empowered with referrals to speak with attorneys if such policies are violated.
To enhance the care of GG and other undocumented immigrants, clinicians and health care systems should be empowered with information about policy advocacy and resources that enhance equitable care (see Figure). Despite broad limitations in access to care, undocumented individuals can access limited primary care and medications through federally qualified health centers in the United States, which may have established partnership agreements with medical centers for referral and consultation (eg, nephrology subspecialty care).38,39 When available, medical-legal partnerships (MLPs) may enable clinicians to tackle immigration issues and address legal determinants of health, thereby improving the health and social well-being of undocumented individuals while helping them navigate resources for transportation and housing, for example.40,41,42,43,44,45 Finally, clinicians and organizations can demonstrate support for policies that broadly provide health care coverage to all individuals residing in the United States, including those that lift exclusions of immigrants from federal policies as well as those that offer states flexibility to tailor Medicaid for expanded coverage. One example of such legislation is the Health Equity and Access Under the Law for Immigrant Families Act of 2023,46 which would remove barriers to health care insurance, including documented immigrants’ 5-year waiting period for eligibility for Medicaid, the Children’s Health Insurance Program, and access to the Affordable Care Act marketplace and Medicare.
Figure. Strategies for Leveraging Reform Roadblocks to Equitable Care for Undocumented Individuals
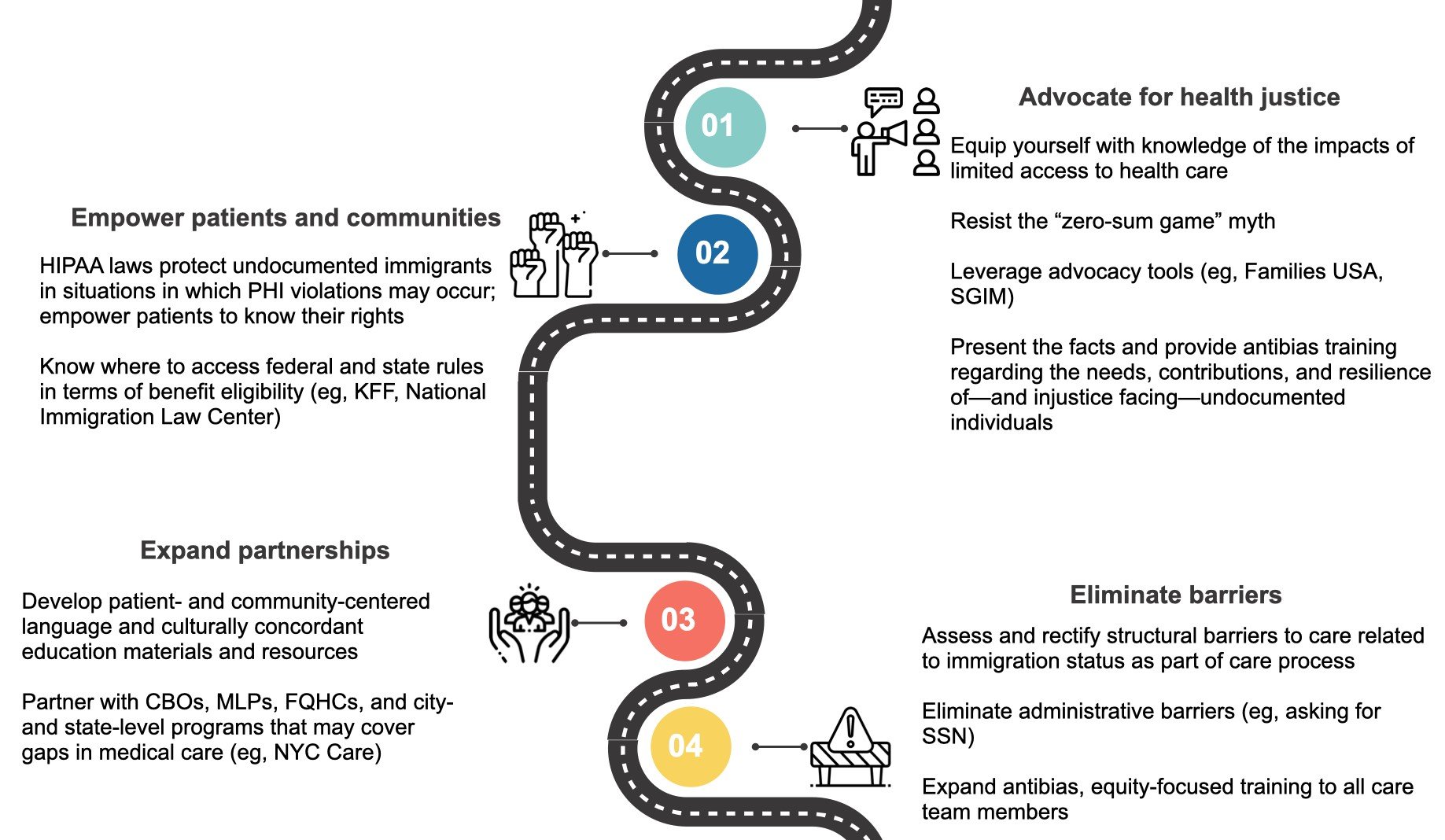
Abbreviations: CBOs, community-based organizations; HIPAA, Health Insurance Portability and Accountability Act; KFF, Kaiser Family Foundation; MLPs, medical-legal partnerships; SGIM, Society of General Internal Medicine.
One key practice that can be employed by all clinicians to improve care for GG and other undocumented immigrants is to operationalize structural competency and address structural violence, which describes social arrangements that harm individuals and populations, including their health.47 Undocumented immigrants, due to marginalization across multiple domains (eg, race, skin color, gender, religion, sexual orientation), experience structural vulnerability and violence in the form of policy constraints (eg, immigration status), which may restrict their access to health-promoting resources, including comprehensive kidney care.
Antidotes to this structural violence that can be implemented at the level of a clinical encounter include utilization of structural vulnerability assessment tools to enhance clinician capacity to screen, evaluate, and mitigate the structural barriers (eg, anti-immigration policies, xenophobia) that confer substantial health risk.48,49,50 Clinicians and multidisciplinary care teams should also receive training regarding categories of immigration status that impact care and specific resources available for advocacy. Accordingly, traditional structural vulnerability tools, which assess environments, food access, social networks, legal concerns, education, and experience of discrimination, could be expanded to encompass the unique challenges faced by many undocumented individuals in accessing care (see Figure). These challenges include legal barriers and external constraints, such as transportation barriers, lack of linguistically and culturally tailored services, discrimination due to immigration status (eg, social security number or citizenship status required as a precursor to provision of care), complex systems that prohibit access to or produce substantial barriers to care (eg, complex care navigation, digital divide), fear of deportation and presumption of deportability by clinicians due to shifting political landscapes, financial constraints and stolen or lost wages, and stigma.13,21,22,24,25,38,43,47,51 Ideally, clinicians should couple these efforts with administrative changes in their practices (see Figure), including ensuring that intake forms do not request information (eg, social security numbers) that would restrict access to care and working to establish relationships with MLPs and community-based organizations with expertise in navigating care journeys and mitigating the unique barriers facing undocumented individuals.
Beyond the clinic, addressing structural violence and achieving health equity in the United States necessitate a justice-focused approach to policy reform, including advocacy, community power-building, expanded partnerships, and the elimination of administrative barriers (see Figure). Evidence abounds on the profound harm of anti-immigration policies that restrict access to comprehensive health care, including kidney replacement therapy options.38,52 As clinicians and organizations navigate advocacy for patients like GG, they should be prepared to resist the “zero-sum game” myth, which has created innumerable barriers to health-promoting policy solutions by obscuring the collective harm of structural inequities that burden immigrant communities and by preventing coalition building across minoritized and marginalized groups who are made to perceive that “available resources” have fixed dimensions.53
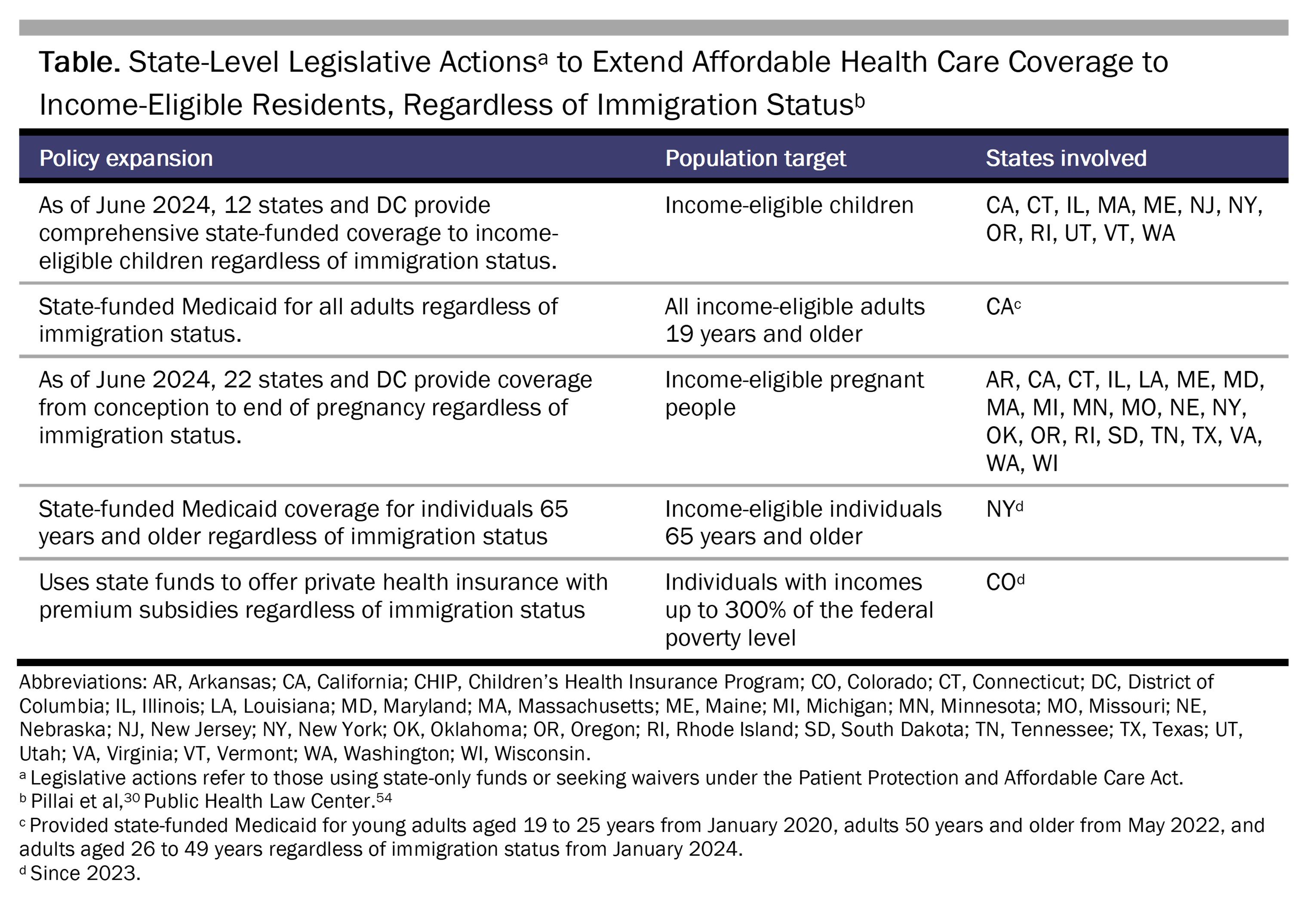
Critical to success are sustained multisector efforts (eg, community health worker, MLP, and navigator programs that aid immigrants in enrolling for benefits) to address the multilevel sociopolitical barriers facing undocumented individuals, along with resistance to policies that erode trust and harm health (eg, reversal of public charge rules) and the need for education on policy advances (see Table). Through our collective efforts as individuals and members of health care organizations, we can contribute to the ideal: a ripple effect of equity-enhancing policy advocacy and optimal health care provision for all.
Brenner JM, Blutinger E, Ricke B, Vearrier L, Kluesner NH, Moskop JC. Ethical issues in the access to emergency care for undocumented immigrants. J Am Coll Emerg Physicians Open. 2021;2(3):e12461.
Eguchi N, Tantisattamo E, Chung D, et al. Outcomes among undocumented immigrant kidney transplant recipients in California. JAMA Netw Open. 2023;6(2):e2254660.
Gely YI, Esqueda-Medina M, Johnson TJ, et al. Experiences with kidney transplant among undocumented immigrants in Illinois: a qualitative study. Kidney Med. 2023;5(6):100644.
Fabi R, Cervantes L. Undocumented immigrants and COVID-19: a call for federally funded health care. JAMA Health Forum. 2021;2(9):e212252.
Park JK, Reyes-Becerra C, Makhlouf MD. State flexibility in emergency Medicaid to care for uninsured noncitizens. JAMA Health Forum. 2023;4(7):e231997.
Aliessa v Novello, 96 NY2d 418 (2001).
Pillai A, Pillai D, Artiga S. State health coverage for immigrants and implications for coverage and care. Kaiser Family Foundation. May 1, 2024. Updated June 20, 2024. Accessed June 24, 2024. https://www.kff.org/racial-equity-and-health-policy/issue-brief/state-health-coverage-for-immigrants-and-implications-for-health-coverage-and-care/
Giuntella O, Lonsky J. The effects of DACA on health insurance, access to care, and health outcomes. J Health Econ. 2020;72:102320.
Park JK, Yale-Loehr S, Kaur G. DACA, public health, and immigrant restrictions on healthcare in the United States. Lancet Reg Health Am. 2023;21:100493.
Immigration, S 1718, Reg Sess (Fla 2023). Accessed April 4, 2024. https://www.flsenate.gov/Session/Bill/2023/1718
Centers for Medicare and Medicaid Services. Medicare Program; End-Stage Renal Disease Prospective Payment System, payment for renal dialysis services furnished to individuals with acute kidney injury, End-Stage Renal Disease Quality Incentive Program, Durable Medical Equipment, Prosthetics, Orthotics and Supplies (DMEPOS) Competitive Bidding Program (CBP) and fee schedule amounts, and technical amendments to correct existing regulations related to the CBP for certain DMEPOS; final rule. Fed Regist. 2018;83(220):56922-57073. Accessed June 25, 2024. https://www.govinfo.gov/content/pkg/FR-2018-11-14/pdf/2018-24238.pdf
Doshi M, Lopez WD, Mesa H, et al. Barriers and facilitators to healthcare and social services among undocumented Latino(a)/Latinx immigrant clients: perspectives from frontline service providers in Southeast Michigan. PLoS One. 2020;15(6):e0233839.
Murphy C. Making the case for medical-legal partnerships: an updated review of the evidence. National Center for Medical-Legal Partnership; 2020. Accessed April 4, 2024. https://medical-legalpartnership.org/wp-content/uploads/2020/10/MLP-Literature-Review-2013-2020.pdf
HEAL for Immigrant Families Act, S 2646, 118th Cong (2023-2024). Accessed April 4, 2024. https://www.congress.gov/bill/118th-congress/senate-bill/2646/titles?s=1&r=92#:~:text=A%20bill%20to%20expand%20access,coverage%2C%20and%20for%20other%20purposes
Metzl JM, Hansen H. Structural competency: theorizing a new medical engagement with stigma and inequality. Soc Sci Med. 2014;103:126-133.
Neff J, Holmes SM, Knight KR, et al. Structural competency: curriculum for medical students, residents, and interprofessional teams on the structural factors that produce health disparities. MedEdPORTAL. 2020;16:10888.
Long S, Littlecott HJ, Eccles GL, et al. Testing the zero-sum game hypothesis: an examination of school health policy and practice and inequalities in educational outcomes. Lancet. 2017;390:S60.
Public Health Law Center. Executive summary: expanding health care access to all through state law. Public Health Law Center; 2023. Accessed March 6, 2024. https://www.publichealthlawcenter.org/sites/default/files/resources/Health-Care-For-All-Summary.pdf



