Medicine and Society
Jul 2024
Peer-Reviewed

Structural determinants of health frameworks must express antiracism to be effective, but racial and ethnic inequities are widely documented, even in harm reduction programs that focus on person-centered interventions. Harm reduction strategies should express social justice and health equity, resist stigma and discrimination, and mitigate marginalization experiences among people who use drugs (PWUD). To do so, government and organizational policies that promote harm reduction must acknowledge historical and ongoing patterns of racializing drug use. This article gives examples of such racialization and offers recommendations about how harm reduction programming can most easily and effectively motivate equitable, antiracist care for PWUD.
The escalating drug overdose crisis in the United States and the stark racialized inequity it has revealed—notably during the COVID-19 pandemic—underscore the urgent need to reconsider traditional health care approaches by placing greater emphasis on harm reduction and on social and structural determinants of health (SDoH)—specifically, systemic racism. The pandemic years witnessed drug-related mortality rates in the United States exceeding 100 000 annually,1 with the rate of deaths among Black individuals surpassing that of White individuals for the first time in 2020—a shift not seen since 1999 during the first wave of opioid overdose deaths.2 In particular, the drug overdose death rate for Black individuals increased from 24.7 per 100 000 in 2019 to 36.8 per 100 000 in 2020, which was 16.3% higher than the rate for White individuals (31.6 per 100 000) in 2020.2 Moreover, Black individuals have experienced higher annual percentage increases in overdose death rates than their White counterparts since 2012, much earlier than previously recognized.2
Conventional health care systems, medical education, and clinical practice have predominantly leaned on biological disease models while often sidelining the role of social causation. This oversight may contribute to the racialized disparities observed in drug-related mortality, particularly among structurally vulnerable, racially minoritized individuals with substance use disorders (SUDs). In contrast to treatment informed by biological disease models, harm reduction focuses on the impact of negative consequences of drug use rather than drug use itself as the target of intervention.3 There is a pressing need to explore alternative models, frameworks, and care systems in addressing SUDs and, in particular, to center racialized inequity and SDoH within a harm reduction framework.
In this article, we explore the interrelatedness of harm reduction and SDoH (including systemic racism) within a framework for the treatment of SUDs. We explore their potential to address health inequities faced by racially minoritized people—specifically, people who use drugs (PWUD)—and make the case that harm reduction programming must pay attention to social context in order to achieve the goal of health equity.
Health inequalities describe any observed disparities in health outcomes regardless of underlying causes, while health inequities are disparities stemming from systemic, avoidable, unjust, and frequently racialized social and economic policies and practices.4 Even though these terms are often used interchangeably, their nuanced differences in meaning hold significant implications for clinical practice, health care policy, and research. For example, while the removal of the mandatory training requirement for prescribers of buprenorphine—a major step in bridging the access gap for patients with opioid us disorder (OUD)—addresses inequality, further steps may be needed to ensure true equity, including, among others, addressing the lack of availability of buprenorphine prescribers within historically marginalized neighborhoods and communities that continue to be left behind in terms of access to medications for OUD.5,6 This distinction between inequality and inequity is essential to truly grasp the intricate relationship between harm reduction and SDoH (including racism)—especially in enhancing health outcomes for racially marginalized groups (see Figure).
Figure. The Interrelation of Structural Determinants of Health and Harm Reduction Interventions
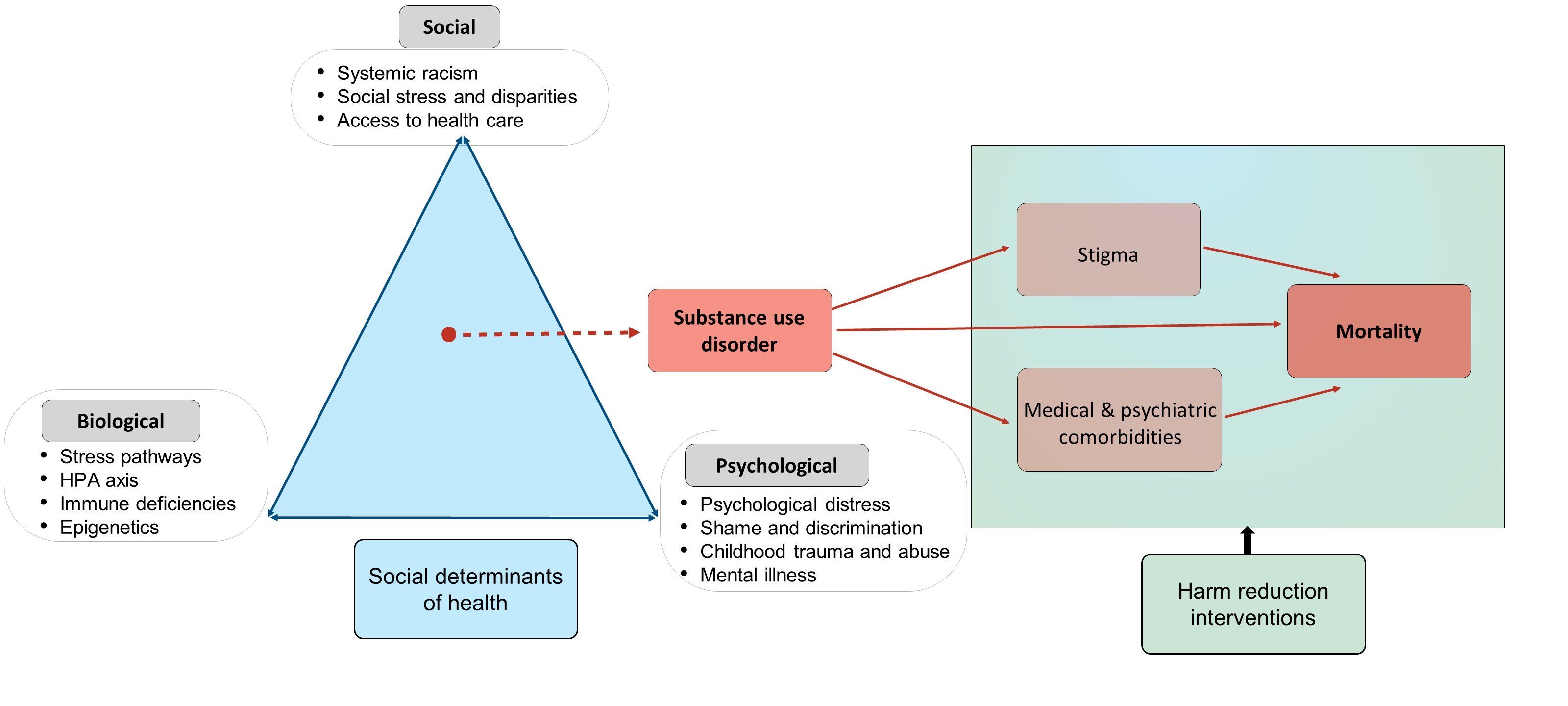
On the left, the Figure depicts the etiological and contributing factors underlying substance use disorder, which leads to stigma and to medical and psychiatric comorbidities, both of which, along with SUD itself, contribute to mortality. Harm reduction strategies intervene to mitigate drug-related harm and stigma.
Abbreviation: HPA, hypothalamic-pituitary-adrenal.
Structural determinants of SUD refer to the conditions in which PWUD are born, live, learn, work, play, worship, and age. These factors affect the health, functioning, health risks, and quality of life of PWUD in many ways through a complex set of interrelated, mutually reinforcing pathways. Notably, structural determinants interact with biological aspects in pain perception, possibly increasing activation of stress-related neural pathways,7 which could perpetuate the addiction cycle. Social influences may not only contribute to adverse health outcomes7 but also serve as primary risk factors.8
Structural determinants function synergistically, not in isolation, as shown in the Figure. For example, SDoH may limit access to evidence-based, lifesaving interventions for OUD, such as buprenorphine, particularly for members of historically racially minoritized groups. To fully understand why, it is essential to consider both downstream and upstream structural determinants.8 Downstream factors include health-related knowledge, attitudes, and beliefs,8 as well as behaviors such as frequently returning to nonmedical substance use or medication nonadherence, which are often present but unrecognized in clinical settings. These downstream factors arise from and are shaped by more remote upstream determinants that include unstable housing, racial profiling by law enforcement, overreaching policies that produce high incarceration rates, and income inequality.9 The health effects of income inequality are evident in the unequal distribution of buprenorphine that often favors more affluent, White areas whose residents have access to private insurance.10,11 Highlighting the impact of income on drug overdose deaths, one study showed that, in 2020, “overdose death rates increased with increasing county-level income inequality ratios.”12 Among Black persons, overdose death rates were highest in counties with the highest income inequality (46.5 per 100 000 population) and lowest in those with the lowest inequality (19.3 per 100 000 population).12 Curiously, among the American Indian and Alaska Native populations, overdose death rates were still very high even in counties with the lowest inequality levels (35.2 per 100 000 population),12 suggesting that structural factors other than income inequality may significantly influence overdose rates among minoritized populations.
Harm reduction is a practical and transformative approach that incorporates community-driven public health strategies to empower PWUD (and their families) with the choice to live healthy, self-directed, and purpose-filled lives.13 Central to harm reduction are health promotion and substance use risk mitigation. Harm reduction is based on grassroots, patient-centric approaches championed by people who use drugs themselves rather than on conventional top-down health care models. Its commitment to equity is evident in several key aspects: (1) reducing the stigma of substance use by providing an alternative to the moral failure and disease model approaches to substance use treatment14; (2) respecting the human rights and personhood of PWUD; (3) elevating and affirming the autonomy of PWUD and their right to be included in their own treatment by providing a choice for safer use, managed use, or abstinence; and (4) adopting a community-oriented approach by ensuring the overall safety of the community.13
Harm reduction principles were embraced and adapted by civil rights groups fighting anti-Black racism in the United States. For example, some of the early practitioners and proponents of harm reduction were the Black Panthers, who provided free breakfasts for children, and the Young Lords, who provided acupuncture for PWUD in the South Bronx.15 When harm reduction was championed by people with a deep understanding of systemic racial minoritization, practices were holistically attuned to combating racialized and ethnic disparities by ensuring resources for and attention to individuals who otherwise would be excluded.
While minoritized communities have adapted harm reduction models to better serve their unique needs, there are indications that some contemporary harm reduction programs may inadvertently perpetuate racial disparities.16 A thematic analysis of harm reduction practices in Toronto revealed the prevalence of structural and institutional racism in harm reduction services, highlighting “colour-blind policies and practices that fail to address the intersectional nature of the drug policy crisis.”16 Other studies have echoed this concerning trend. For example, the adoption of Good Samaritan laws, which ostensibly confer criminal immunity to individuals who offer assistance during an overdose, may inadvertently exacerbate preexisting racialized inequities because public education campaigns have failed to offer minoritized individuals with SUD the same level of awareness of these laws as privileged populations, thereby fostering misinformation about the protections these laws offer and lack of willingness among minoritized individuals to offer assistance.17 Similarly, emerging evidence has also shown deficiencies in naloxone training and distribution among minoritized PWUD.18,19 For example, drawing on Medicare claims data from 2016 to 2019, Barnett and colleagues observed that within 180 days of an index event, only 14.4% of Black/African Americans with OUD were prescribed naloxone compared to 22.9% of their White peers.19
Taken as a whole, harm reduction practices cannot offer social justice without explicitly naming and intentionally targeting racialized injustice within current drug policies and practices. This sentiment is echoed by Lopez et al, who concluded that the assessment of social and structural dynamics is needed to ensure harm reduction protections for racially minoritized Black and Brown people.20
To address SDoH in treatment of SUDs, interventions must operate on multiple levels. Single-level strategies, while valuable, offer a limited perspective. Comprehensive interventions intersect various socioecological levels, including individual, interpersonal, organizational, community, and policy levels.21 But for such interventions to yield tangible change, clinicians must avoid reductionist leanings and embed SDoH indices in their routine practice without oversimplifying complex socioecological elements. Without accurate measurement of social determinant indices, we lack insight into their influence on harm reduction and broader health interventions. Several tools have emerged to assess facets of social and economic stability that range from individual characteristics to overarching societal contexts.22
Some of the tools with potential utility in clinical settings include (1) the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE); (2) the Social Needs Screening Tool; (3) the Health-Related Social Needs Screening Tool; and (4) the Structural Vulnerability Assessment Tool. PRAPARE is an evidence-based and standardized patient risk assessment protocol designed to assess SDoH. It has 4 core domains: personal characteristics, family and home, money and resources, and social and emotional health.23 The Social Needs Screening Tool, designed by the American Academy of Family Physicians, is used for screening across 5 core health-related domains, including housing, food, transportation, utilities, and personal safety.24 The Health-Related Social Needs Screening Tool, created by the Center for Medicare and Medicaid Innovation, uses the Accountable Health Communities Model; it screens across 5 core domains including housing instability, food insecurity, transportation problems, and utility help needs. Results from this tool are often used to inform treatment plans and make referrals to community services.25 Finally, the Structural Vulnerability Assessment Tool is a 43-item questionnaire that assesses needs across the 6 domains of economic stability, education, social and community context, health and clinical care, neighborhood and physical environment, and food security.9,26 In essence, grasping SDoH is crucial for addressing SUDs, but so is having precise instruments to measure and address them. When assessments are adeptly applied, they can foster more insightful and holistic health care solutions, ensuring a complete understanding of an individual’s socioecological environment.
The devastating grip of drug overdose mortality in minoritized communities underscores the urgent need to center SDoH in harm reduction frameworks. While the impact of SDoH continues to be characterized and described in the medical literature, challenges remain in establishing the most culturally appropriate SDoH metrics. Integrating harm reduction into health care systems and practices is critical but insufficient without a thorough understanding of social context. Although the core principles and strategies of harm reduction were promoted within the context of the civil rights and antiracist movements,8 harm reduction strategies can only realize their transformative power by remaining unwaveringly committed to equity, autonomy, and justice. To save the lives of historically marginalized people amidst the relentless drug overdose crisis, our health care systems must integrate harm reduction strategies that center SDoH.
Drug overdose deaths in the US top 100,000 annually. News release. Centers for Disease Control Prevention; November 17, 2021. Accessed February 17, 2024. https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2021/20211117.htm
Hawk M, Coulter RWS, Egan JE, et al. Harm reduction principles for healthcare settings. Harm Reduct J. 2017;14(1):70.
Arcaya MC, Arcaya AL, Subramanian SV. Inequalities in health: definitions, concepts, and theories. Glob Health Action. 2015;8(1):27106.
Hansen H, Siegel C, Wanderling J, DiRocco D. Buprenorphine and methadone treatment for opioid dependence by income, ethnicity and race of neighborhoods in New York City. Drug Alcohol Depend. 2016;164:14-21.
Hobson JM, Moody MD, Sorge RE, Goodin BR. The neurobiology of social stress resulting from racism: implications for pain disparities among racialized minorities. Neurobiol Pain. 2022;12:100101.
Harm Reduction Steering Committee. Harm Reduction Framework. Substance Abuse and Mental Health Services Administration; 2023. Accessed January 17, 2024. https://www.samhsa.gov/sites/default/files/harm-reduction-framework.pdf
Godkhindi P, Nussey L, O’Shea T. “They’re causing more harm than good”: a qualitative study exploring racism in harm reduction through the experiences of racialized people who use drugs. Harm Reduct J. 2022;19(1):96.
Pamplin JR 2nd, King C, Cooper C, et al. Pathways to racial disparities in the effects of Good Samaritan laws: a mixed methods pilot study. Drug Alcohol Depend. 2023;249:110823.
Khan MR, Hoff L, Elliott L, et al. Racial/ethnic disparities in opioid overdose prevention: comparison of the naloxone care cascade in White, Latinx, and Black people who use opioids in New York City. Harm Reduct J. 2023;20(1):24.
Alegría M, NeMoyer A, Falgàs Bagué I, Wang Y, Alvarez K. Social determinants of mental health: where we are and where we need to go. Curr Psychiatry Rep. 2018;20(11):95.
What is PRAPARE? PRAPARE. Accessed August 11, 2023. https://prapare.org/what-is-prapare/
Social Needs Screening Tool. American Academy of Family Physicians. Accessed August 11, 2023. https://www.aafp.org/dam/AAFP/documents/patient_care/everyone_project/patient-short-print.pdf
Center for Medicare and Medicaid Innovation. The Accountable Health Communities Health-Related Social Needs Screening Tool. Centers for Medicare and Medicaid Services. Accessed August 11, 2023. https://innovation.cms.gov/files/worksheets/ahcm-screeningtool.pdf
Structural Vulnerability Assessment Tool. Kaiser Permanente. Updated June 2020. Accessed February 17, 2024. https://sdh-tools-review.kpwashingtonresearch.org/screening-tools/structural-vulnerability-assessment-tool