Case and Commentary
Mar 2022
Peer-Reviewed

Abundant evidence demonstrates that enduring, endemic racism plays an important role in determining patient health. This commentary reviews a patient case about disease self-management and subsequent health outcomes that are shaped by social and economic circumstances. We analyze the case using a framework for social care developed in 2019 by the National Academies of Sciences, Engineering, and Medicine (NASEM). We then propose that the NASEM framework be adapted by adding the category abolition, which could make the other social care practices transformative for historically marginalized populations.
Mr W is a 59-year-old man with type II diabetes mellitus. Mr W takes oral medication for diabetes and uses a glucometer when he has access to lancets and strips. Mr W has a primary care physician, Dr PCP, but rarely attends clinic appointments since he does not have transportation. He eats mostly food he finds in trash cans or food donated to him; occasionally, he can purchase fast food. He is currently unsheltered, living in a tent encampment.
A few days after his last lancet finger stick, Mr W’s index finger became swollen, red, and painful. He went to a nearby emergency department (ED), where Dr ED drained a felon abscess and prescribed antibiotics. Mr W’s diet and limited hygiene opportunities have contributed to his ill health, so Dr ED prescribes agency food assistance and offers alcohol wipes so Mr W can clean his fingers before and after finger sticks. An ED social worker offered Mr W a shelter bed, but he declines, preferring to return to his tent and belongings.
To enroll in the food assistance program, Mr W must attend a nutrition consultation, but he has no way to get there and no address to which food can be delivered. Mr W’s phone is stolen, so he misses a reminder call from Dr PCP’s office, can’t access his calendar, and misses a follow-up appointment. The alcohol wipes run out and Mr W stops checking his blood sugar. Soon feeling ill again, Mr W goes to the ED. Mr W is admitted, diagnosed him with hyperglycemia and a urinary tract infection, and prescribed antibiotics and access to a private bathroom. The ED social worker has long been asking the city to supply water and bathroom access for residents of the encampment. Permanent housing requests are placed and pending. Mr W returns to his tent.
A popular public health parable describes the dual urgency of pulling drowning children from a river and looking upstream to prevent more children from entering the water.1 Over decades of telling, the story has taken many forms. A second version of the story casts poisoned fish in the role of the drowning children.2 In health care settings, Mr W’s finger abscess is more commonplace than children drowning in a river or poisoned fish, but the moral of the story is similar. Consistent and convincing evidence shows that social and environmental deprivation—including insufficient or unsafe food, housing, water, and transportation—contribute to poor health.3,4,5,6,7,8,9 In the United States, however, we are less attentive to addressing adverse social conditions than to immediate injuries.10
In this case, Mr W’s medical condition and social circumstances are inextricably linked; their synergies lead to his acute illnesses, diminish the effectiveness of his medical treatment, and impede his opportunity to flourish. In formulating a plan for treatment, Dr ED reasonably looked upstream. In addition to draining Mr W’s abscess and prescribing antibiotics, the physician made referrals to help him obtain nutritious food, safe housing, and clean water. Since emerging evidence suggests that, in cases like Mr W’s, interventions to address social needs and disease self-management may yield health improvements and cost savings,11,12,13,14,15,16 it may be surprising that after multiple well-intentioned attempts by Dr ED to address Mr W’s social needs, neither Mr W’s circumstances nor his health improved. Why?
To answer this question, we first turn to a 2019 National Academies of Sciences, Engineering, and Medicine (NASEM) report on medical and social care integration, which focused explicitly on articulating roles for health care stakeholders in responding to the rapidly growing evidence that health is powerfully shaped by social circumstances.17 The NASEM report defined 5 broad “social care” categories—awareness, assistance, adjustment, alignment, and advocacy—each of which describes different types of activities in which health care systems might participate to influence patients’ social determinants of health.17 The 5 categories encompass patient-level, health care delivery-targeted interventions, and also more community-directed initiatives; all are relevant to Mr W’s case. In this paper, we explore ways that the NASEM report’s recommendations might be used to spur more intentional and coordinated actions by the health care system to improve outcomes for patients like Mr W. We then consider how the NASEM social care categories also might be interrogated and reenvisioned to more deliberately dismantle the inequity in opportunities to achieve health and well-being that more fundamentally shapes Mr W’s story. This reenvisioning process leads us to suggest that the NASEM report’s original social care categories be viewed through the frame of a sixth A: abolition, which would make health care’s social care activities more impactful and enduring.
The NASEM framework begins by underscoring the relevance of efforts to understand patients’ socioeconomic environments (awareness), including patient- and community-level social needs and assets, as a core element of integrated care approaches. It also defines 2 categories of patient care interventions that might stem from increased awareness about social conditions. These include activities to tailor the delivery of medical care based on identified social barriers (adjustment) and to more directly intervene on social risk (assistance). Finally, alongside patient-level activities, the framework recommends work at the community and policy level. In these areas, health care systems might assume roles to better align their own efforts with community needs and priorities (alignment) and to advocate for deeper social and structural investments (advocacy) (see Table).
| Social Care Category | Definition |
|---|---|
|
Awareness |
“Activities that identify the social risks and assets of defined patients and populations” |
|
Adjustment |
Activities that alter “clinical care to accommodate identified social barriers” |
|
Assistance |
Activities that reduce “social risk by assistance in connecting patients with relevant social care resources” |
|
Alignment |
Activities “undertaken by health care systems to understand existing social care assets in the community” and then organize and invest in health care activities to facilitate synergies that positively affect health outcomes. |
|
Advocacy |
Activities in which “health care organizations work with partner social care organizations to promote policies that facilitate the creation and (re)deployment of assets or resources” to address health and social needs. |
|
a Adapted from National Academies of Sciences, Engineering, and Medicine.17
|
|
A robust social care program would involve complementary work at both the patient and the community level. In Mr W’s case, the ED physician learns about Mr W’s housing instability (awareness) and provides cleaning supplies and referrals for food and housing (assistance), and the ED social worker advocates for improved hygiene resources for the tent encampment (advocacy).
In the NASEM report, a strong emphasis is placed on health care systems that can ensure that social care activities in each of the 5 categories are not only feasible but also impactful for both individuals and populations. Feasible and impactful social care in this case would eliminate reliance on the good-hearted Dr ED and instead embed social care practices in Dr ED’s workflow to help him identify and intervene on the socioeconomic adversities faced by Mr W and many other patients like him. Yet it is not clear from the case presentation that the health care system responsible for Mr W’s care has committed to systematically engaging in high-quality activities in any of the NASEM categories. Dedicated social care staff and staff training, modified clinical workflows, and health information technology tools embedded in those core workflows are needed to provide high-quality social care and to ensure that data generated from individual patient care can be used in real time both to improve care and to guide investments at the population level.18 For instance, is a standardized social risk/asset screening systematically conducted in settings with well-trained, culturally competent staff who sensitively approach patients with an understanding of their lived experience? Are data about socioeconomic risks documented and protected in electronic health records? What informatics tools and processes are available to generate and, as appropriate, track relevant referrals to community-based services and disease management support? How are data from patients like Mr W aggregated and applied to inform future care as well as community-level alignment and advocacy decisions?
Unfortunately, Mr W’s health outcomes might not improve even in a health care system investing in the high-quality practices defined in the NASEM report. Although the framework provides a useful organizing tool to operationalize health care sector actions related to social adversity, these social care activities—whether focused on patient care or at the community level—are often implemented absent an awareness of the racialized systems and structures that have led to and perpetuate health inequities. Inattention to structural and systemic racism as fundamental causes of individuals’ socioeconomic risks means that health care’s social care practices will prove insufficient for improving health outcomes for marginalized patients. Although the case does not provide information about Mr W’s racial or ethnic identity, in the United States, Black, Indigenous, and other persons of color are disproportionately homeless.19 Black Americans constitute 13.4% of the US population20 but make up 39% of the US homeless population19 as a result of structural inequities in housing, education, employment, and policing and carceral systems that discriminate against Black people.21 These same structures also limit opportunities for other socially marginalized groups.22
It is therefore not surprising that we must do more, do it differently, and do it better in order to improve health and health equity. Overcoming health inequity demands more than adding social care practices to health care. It also requires addressing the inequities in other sectors and institutions (eg, education, criminal justice, housing) that influence the physical health and well-being of Black and other marginalized populations.
In this particular case, we are specifically tasked with improving the design and delivery of social care practices in the health care sector to better meet the needs of patients like Mr W. To achieve this goal, we follow the lead of a recent Lancet article describing abolition medicine.23 The Thirteenth Amendment to the US Constitution, which abolished slavery as we currently understand it, nonetheless allowed slavery and “involuntary servitude” to continue for those convicted of crimes.24 As a result, the abolition movement has predominantly focused on eradicating racialized policing, surveillance, and carceral systems.25 The Lancet article authors advocate for similarly challenging racialized practices in medicine,23 which also have worked to diminish the health and well-being of Black people. We now extend their argument to propose abolition as a sixth category through which to frame health care’s other social care activities (see Figure), appreciating that this framing will influence outcomes for all racial/ethnic minorities and other socially marginalized populations.
Figure. Health Care System Activities That Strengthen Social Care Integrationa
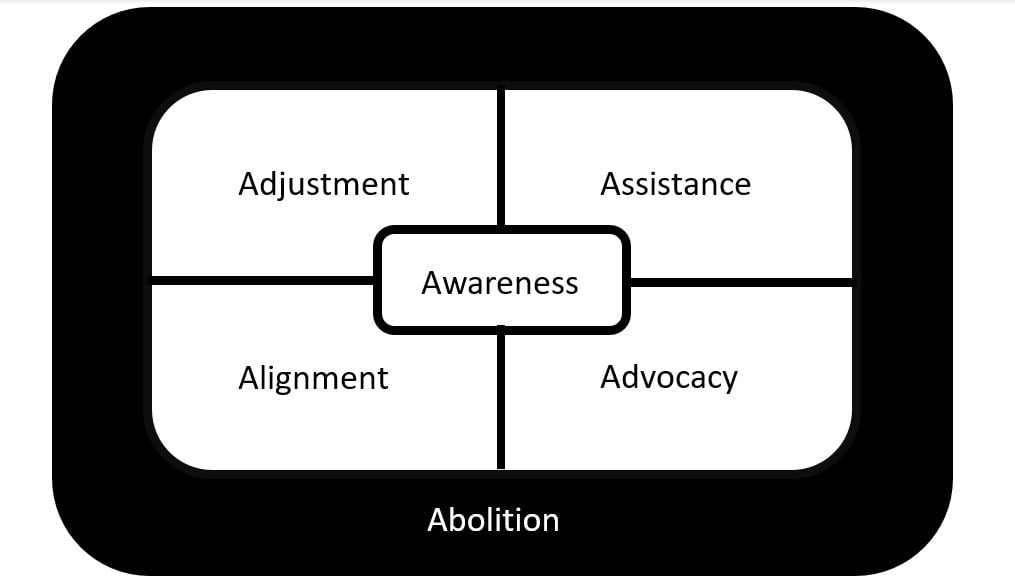
a Adapted with permission of the National Academies Press from National Academy of Sciences, Engineering, and Medicine.17 Permission conveyed through Copyright Clearance Center, Inc.
Applying an abolition frame involves redefining the goals, methods, and activities associated with each of the 5 social care categories originally articulated by NASEM. As described below, doing so would require more explicitly designing and implementing social care integration practices that are antiracist to help health care teams both to understand and to reverse racial inequity and opportunity gaps for patients like Mr W.
Awareness. Abolition-influenced awareness activities would be designed in collaboration with patients from marginalized backgrounds, whose input on framing, content, and implementation could improve these patients’ experiences with social risk and asset screening.26,27 Health care teams would also protect against the potential harms of such screening—including the possibility that collected data could increase opportunities for police surveillance and discrimination and exacerbate distrust—instead ensuring that data collection is paired with data use and distribution safeguards as well as meaningful interventions.28,29 Awareness activities would not end at patient-directed socioeconomic risk and asset assessments; health care teams would be required simultaneously to increase their own awareness about racism, including current and historical institutional racism and antiracist practices.30,31,32,33
Adjustment. Looking at adjustment strategies through an abolition frame would proactively involve patients in treatment planning (eg, using shared decision-making tools) with the intent of improving both the experience of social care and outcomes for historically marginalized patients.34,35 In Mr W’s case, a shared decision-making discussion might explore the comparative advantages of his transition to a temporary shelter bed vs staying close to his worldly possessions and familiar community. Shared decision making is a particularly powerful abolition strategy because shared decision making is fundamentally about supporting patients’ agency, which can affect both their experience of health care and their health outcomes. Although the practice has been used less frequently in care provided to racial and ethnic minorities and other socially marginalized patients than in care provided to White patients,35 if implemented both well and routinely, it would support abolition’s goals of sharing power, increasing patient agency, and building clinician humility. If achieved, these types of changes would counter some forms of institutional racism and help to decrease health inequities.
Assistance. Abolition also would involve ensuring that assistance activities are designed in ways that maximize patient dignity. For instance, health systems might develop ways in which people can simultaneously give and receive. Three studies of CommunityRx, a community resource referral intervention, show that half the patients who received social care information shared it with others.27,36,37 At the University of Chicago, the Feed1st program has provided emergency food relief to thousands of patients over 10 years via self-serve, no barriers, hospital-based food pantries. Over time, many patients and family members who have obtained services from the pantries have also contributed back (eg, donating food, stocking shelves, participating in advocacy, creating their own food security initiatives.38,39) Providing these kinds of opportunities can simultaneously strengthen patients’ self-respect and build community, both of which are foundational to abolition.
Alignment and advocacy. As in the original NASEM framework, abolition would require pairing patient-focused social care interventions with community-directed alignment and advocacy activities. But now these community-directed investments would more specifically focus on the systems and structures that perpetuate inequities, including racist policies and practices both within and external to the health care system. Consistent with the abolition movement’s original focus, health systems committing to social care would analyze and share data about the health effects of police violence and incarceration.40 They would use those data to advocate to overcome racialized policing and carceral policies that in turn perpetuate and exacerbate homelessness.40 They would leverage the health care system’s role as an anchor institution to invest in neighborhood low-income housing,41 with special attention to eliminating racist programs and policies built into many housing assistance programs.42,43,44
Returning to Mr W, we again pose the question of why Dr ED’s well-intentioned efforts did not clearly change the course of Mr W’s illness. One potential explanation might lie in the lack of institutional investment in a high-quality system that supports the integration of social and medical care for individuals and populations. But our collective failure to effectively serve patients in circumstances like Mr W’s also reflects the lessons of a modern version of our public health parable. In the modern retelling, the bank of the river is three-dimensional: Black, Indigenous, and other persons of color living in the United States, people living in poverty, and others affected by structural and systemic racism are forced to stand closer to the edge of the river than other groups of people, thereby disproportionately increasing their initial risk of falling into the water. As a result of restricted access to pools, lakes, and rivers, marginalized groups also are less likely to have learned how to swim, which increases their risk of drowning.45 The updated parable underscores how social determinants of health are closely tied to social determinants of equity.46 In the case of Mr W, that link forces us to critically evaluate health care initiatives concerning social adversity to ensure not only that such initiatives are high quality, standardized, and systematically implemented, but also that they are designed in ways that both acknowledge and help to reduce the entrenched and inequitable threats to health levied on historically marginalized people.
McKinlay J. A case of refocusing upstream: the political economy of illness. In: Jaco EG, ed. Patients, Physicians, and Illness: A Sourcebook in Behavioral Science and Health. 3rd ed. Free Press; 1979:9-25.
Dave G, Wolfe MK, Corbie-Smith G. Role of hospitals in addressing social determinants of health: a groundwater approach. Prev Med Rep. 2021;21:101315.
Schoeni R, House J, Kaplan G, Pollack G. Making Americans Healthier: Social and Economic Policy as Health Policy. Russell Sage Foundation; 2008.
Smedley BD, Syme SL; Committee on Capitalizing on Social Science and Behavioral Research to Improve the Public’s Health. Promoting health: intervention strategies from social and behavioral research. Am J Health Promot. 2001;15(3):149-166.
Bradley EH, Taylor LA. The American Health Care Paradox: Why Spending More Is Getting Us Less. Public Affairs; 2013.
Rojas Smith L, Amico P, Goode S, Hoerger T, Jacobs S, Renaud J. Evaluation of the Health Care Innovation Awards: Community Resource Planning, Prevention, and Monitoring: Second Annual Report. RTI International; 2016. Accessed January 19, 2022. https://downloads.cms.gov/files/cmmi/hcia-communityrppm-secondevalrpt.pdf
Armstrong Brown J, Berzin O, Clayton M, et al. Accountable Health Communities (AHC) Model Evaluation. First Evaluation Report. RTI International; 2020. Accessed January 19, 2022. https://innovation.cms.gov/data-and-reports/2020/ahc-first-eval-rpt
Peng Y, Hahn RA, Finnie RKC, et al; Community Preventive Services Task Force. Permanent supportive housing with housing first to reduce homelessness and promote health among homeless populations with disability: a community guide systematic review. J Public Health Manag Pract. 2020;26(5):404-411.
Ponka D, Agbata E, Kendall C, et al. The effectiveness of case management interventions for the homeless, vulnerably housed and persons with lived experience: a systematic review. PLoS One. 2020;15(4):e0230896.
National Academies of Sciences, Engineering, Medicine. Integrating Social Care Into the Delivery of Health Care: Moving Upstream to Improve the Nation’s Health. National Academies Press; 2019.
Henry M, de Sousa T, Roddey C, Gayen S, Bedar JT; ABT Associates. The 2020 Annual Homeless Assessment Report (AHAR) to Congress: Part 1: Point-in-Time Estimates of Homelessness. US Department of Housing and Urban Development; 2021. Accessed November 22, 2021. https://www.huduser.gov/portal/sites/default/files/pdf/2020-AHAR-Part-1.pdf
QuickFacts: United States. US Census Bureau. Accessed October 22, 2021. https://www.census.gov/quickfacts/fact/table/US/PST045219
Homelessness and racial disparities. National Alliance to End Homelessness. Updated October 2020. Accessed April 12, 2021. https://endhomelessness.org/homelessness-in-america/what-causes-homelessness/inequality/
United States of America 1789 (rev. 1992). Constitute. Accessed October 22, 2021. https://www.constituteproject.org/constitution/United_States_of_America_1992
Alexander M. The New Jim Crow: Mass Incarceration in the Age of Colorblindness. New Press; 2012.
Smedley BD, Stith AY, Nelson AR, eds; Institute of Medicine. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. National Academies Press; 2003.
Braveman P, Gottlieb L, Francis D, Arkin E, Acker J. What can the health care sector do to advance health equity? Robert Wood Johnson Foundation. November 12, 2019. Accessed April 12, 2021. https://www.rwjf.org/en/library/research/2019/11/what-can-the-health-care-sector-do-to-advance-health-equity.html
Powell W, Adames HY, Lewis JA. Breath, eyes, memory: transforming health systems and advancing public health policies for radical healing. Health Disparities Institute, UConn Health; 2021. Accessed February 16, 2022. https://health.uconn.edu/health-disparities/wp-content/uploads/sites/260/2021/05/RadicalHealingPolicy.pdf
Washington HA. Medical Apartheid: The Dark History of Medical Experimentation on Black Americans From Colonial Times to the Present. Harlem Moon; 2006.
Hogan Lovells, LLP. ACCC Financial Advocacy Network shared decision making summit executive summary. Association of Community Cancer Centers; 2018. Accessed November 30, 2021. https://www.accc-cancer.org/docs/Documents/meetings/2018-shared-decision-making-for-financial-advocates-summit/financial-advocacy-network-shared-decision-making-executive-summary-final
Levine L. Hospital food pantries serve staff, patients, caregivers, and family: Feed1st food pantries alleviate hunger at U of C Medical Center. South Side Weekly. January 20, 2021. Accessed October 24, 2021. https://southsideweekly.com/hospital-food-pantries-serve-staff-patients-caregivers-and-family/
DeGrane S. Cancer survivor brings nutritional support to cancer patients in Homewood. Chicago Tribune. August 18, 2020. Accessed October 24, 2021. https://www.chicagotribune.com/suburbs/daily-southtown/ct-sta-cancer-center-farmers-market-st-0819-20200818-fdq5gwhpj5amrgwqzx4eqr644i-story.html
Gillespie S, Batko S, Chartoff B, VeShancey Z, Peiffer E. Five charts that explain the homelessness-jail cycle—and how to break it. Urban Institute. September 16, 2020. Accessed November 22, 2021. https://www.urban.org/features/five-charts-explain-homelessness-jail-cycle-and-how-break-it
Hawryluk M. Why hospitals are getting into the housing business. Kaiser Health News. October 4, 2019. Accessed April 12, 2021. https://khn.org/news/why-hospitals-are-getting-into-the-housing-business/
Velasco G, Fedorowicz M. Applying a racial equity lens to housing policy analysis. Housing Matters. August 5, 2020. Accessed April 13, 2021. https://housingmatters.urban.org/articles/applying-racial-equity-lens-housing-policy-analysis
Housing discrimination against racial and ethnic minorities 2012 dataset. Office of Policy Development and Research. Accessed July 8, 2021. https://www.huduser.gov/portal/datasets/hsg_discrimination.html
Moses J. Demographic Data Project: part III: race, ethnicity, and homelessness. National Alliance to End Homelessness; 2019. Accessed April 13, 2021. https://endhomelessness.org/wp-content/uploads/2019/09/DDP-Race-brief-09272019-byline-single-pages-2.pdf
Gadberry A, Gadberry J. Black drowning deaths: an introductory analysis. Int J Aquatic Res Educ. 2020;13(1):4.
Jones C. Achieving health equity: tools for naming and addressing racism and other forms of structured inequity. Address presented at: We Can Do Better 10th Annual Conference; January 17, 2019; Portland, OR. Accessed Oct 24, 2021. https://www.youtube.com/watch?v=G3KOs7hg9Bs



