Case and Commentary
Feb 2021
Peer-Reviewed
医生、药剂师和其他卫生专业人员在解决健康问题的社会决定因素和健康差异方面发挥着重要作用。多年来,药剂师一直作为社区的重要成员开展工作,并定期与患者交流,从而解决所有面临健康差异的群体的健康问题社会决定因素。本文所述的案例强调了社会决定因素在健康结果方面所起的作用,以及药剂师应如何帮助改善这些结果。通过合作,药剂师和医生可以帮助降低成本并改善健康结果。
AJ 是一位未参加保险的 85 岁男子,其英语水平有限,长期患有 2 型糖尿病、高血压和肥胖,并且药物依从性较差。AJ 是联邦合格健康中心(federally qualified health center,FQHC)的一名患者,其医生将其转诊至药剂师 ML,以协助其管理慢性疾病。ML 执业于 FQHC 诊所,是跨专业团队的一名成员,该团队由医生、执业护士、医生助理、医疗助理和营养师组成。ML 根据与医生签订的合作实践协议(collaborative practice agreement,CPA)开展工作,该协议允许她扩大执业范围,可根据协议条款启动、修改和停止药物治疗。1在 AJ 就诊期间,ML 在 FQHC 的电子健康档案(electronic health records,EHR)中查看了他的图表记录。ML 注意到 AJ 最近的A1C(衡量患者 3 个月内平均血糖水平的指标)为 11%,这表明 AJ 目前要么没有服用药物,要么服用了药物也没能控制住糖尿病。ML 还注意到 AJ 服用了不止一种血管紧张素转换酶(angiotensin-converting-enzyme,ACE)抑制剂处方药。大约 5% 的老年患者会重复服用 ACE 抑制剂,这通常表明临床医生们在管理患者处方时缺乏沟通。2AJ 还告诉 ML,他使用的胰岛素剂量一直都低于要求的剂量,
试图让胰岛素用得更久一些,并承认他没有按照建议去预约的牙科就诊,因为他一直在省钱以购买食物和支付公交费。他询问他的新处方药要花多少钱。
本案例中的患者正在经历着以下方面所带来的若干典型健康影响:健康问题社会决定因素(social determinants of health,SDOH)或者会显著影响健康的人们出生、成长、生活、工作和变老时的环境(见图 1)。3特别要注意的是,AJ 还受到食物匮乏、获得医疗保健服务的机会有限、健康素养有限、语言障碍和缺乏社会支持等不公待遇——所有这些都是药剂师经常会了解到的方面。
图 1。健康问题社会决定因素
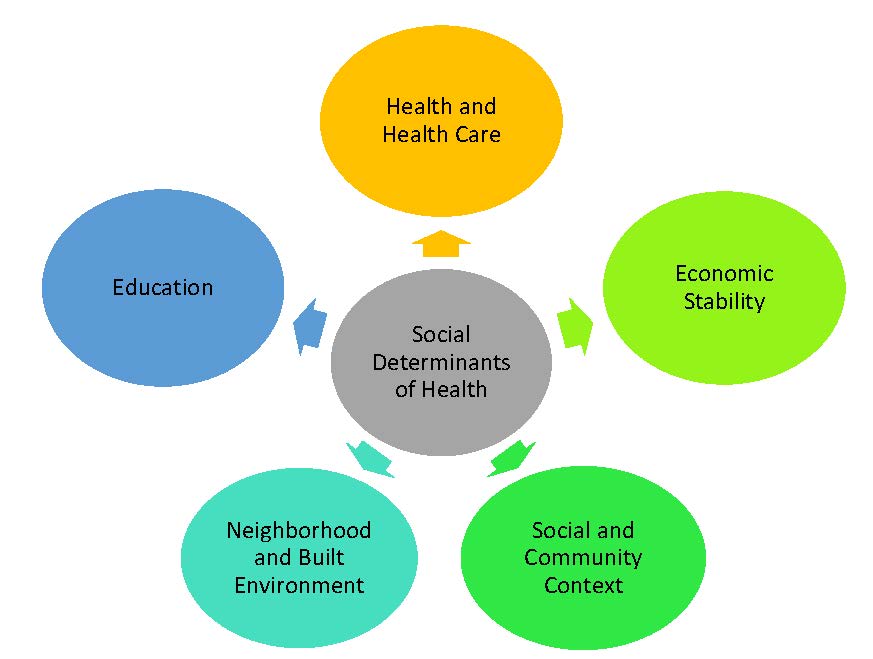
改编自美国卫生与公众服务部。4
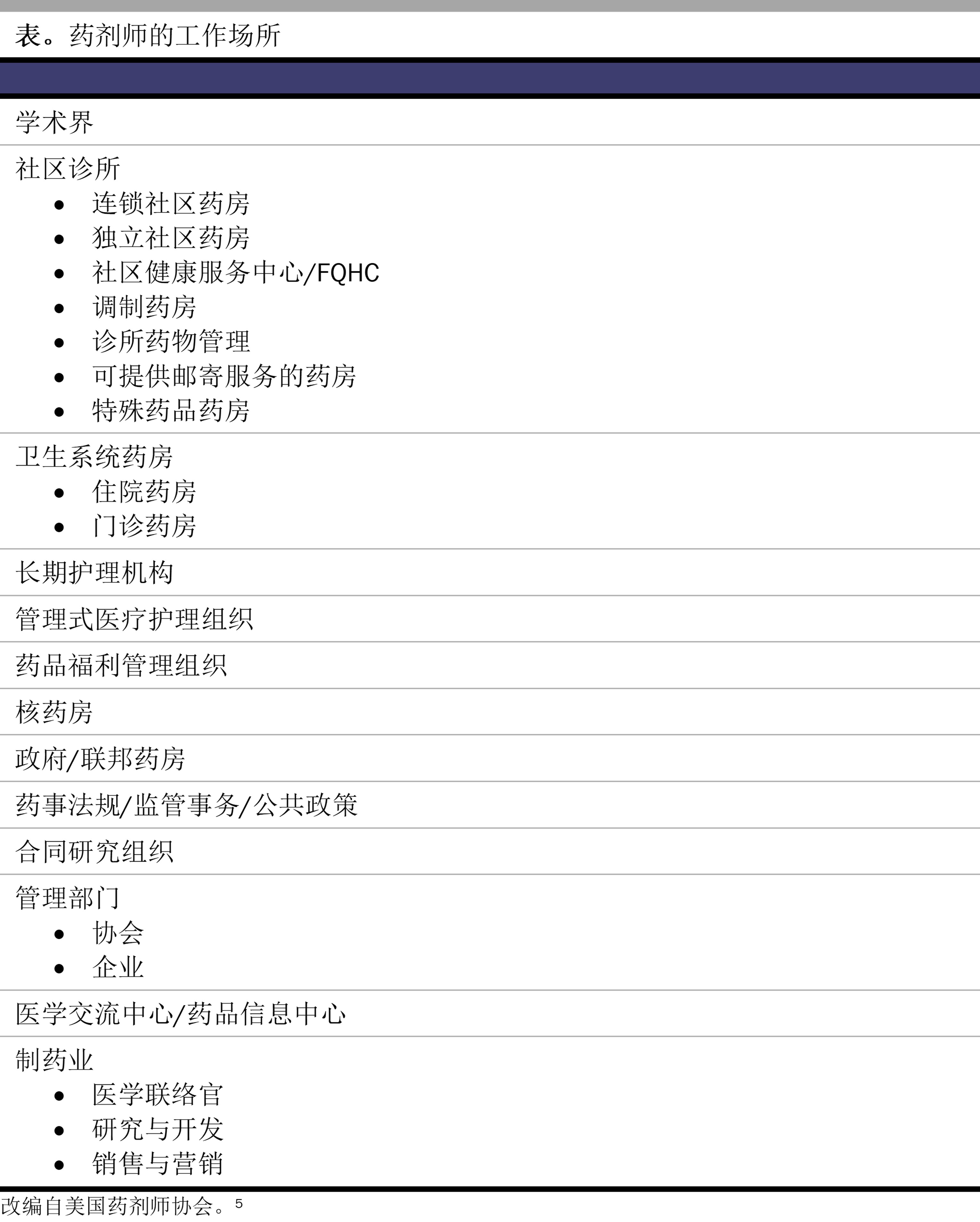
药剂师经常会遇到像 AJ 这样的情况,但是他们具备可协助解决这些障碍的知识和技能。尽管药剂师通常在社区药房工作,但也有许多药剂师在医生诊所、诊所、医院、长期护理机构和其他场所工作(见表)。
在这种情况下,AJ 的医生在安排预约之前与 ML 讨论了患者的病情,并请求 ML 协助管理其慢性疾病并优化其药物治疗。尽管将 AJ 转诊至双语药剂师 ML 处,可以促进沟通、建立信任并管理其慢性疾病,但是想必还有其他工具(例如翻译专线服务)可供其他团队成员在需要时使用。ML 全面评估了 AJ 所患疾病的药物治疗情况,确定了教育领域,制定了护理计划,并根据既定的 CPA 停用了重复使用的 ACE 抑制剂。
由于 AJ 未参加保险,ML 应指引 AJ 去患者导航员处,评估他是否符合健康保险或患者援助计划的资格,或者是否符合根据其收入按浮动比例收费的资格。因为FQHC 是为未参加保险的患者和低收入患者提供医疗保健服务,所以符合 340B 药品定价计划的资格,这让他们能够以极低的价格获得药物,同时也可让患者享受这些折扣价格。通过评估 AJ 的收入,患者导航员可以帮助他享有获得更实惠药物的资格。
此外,ML 还可以在社会支持方面提供协助。例如,ML 可以促进 AJ 与社区健康顾问之间的联系,后者可以为他提供资源,让他可以免费或以折扣价获得杂货和膳食。ML 还可告知 AJ,FQHC 可提供免费交通服务以及如何在医疗助理的帮助下为其就诊和牙科预约安排交通工具。
ML 随后还可与医生进行简短沟通,讨论行为健康服务转诊以帮助 AJ 调节压力。在这次会诊中由不同团队成员(包括 ML在内)执行的所有干预措施都将记录在 EHR 中,以促进护理连续性并监测患者的健康结果。想象一下,在他 3 个月的随访中,由于适当使用药物、明显改变生活方式和增加获得护理的机会,AJ 的 A1C 水平已降至 9.7%(目标是低于 9%6)。
该案例说明了利用各种医疗保健专业人员解决 SDOH 的益处。了解并解决患者在临床方面以外面临的护理障碍,可能会对其整体健康结果产生重大影响。该案例中的医疗保健从业人员将 SDOH 评估整合到临床护理中,并利用各种医疗保健从业人员的专业知识和社区资源来解决 AJ 在获得护理方面面临的障碍。
美国在其医疗保健系统上的投资多于其他很多国家,但该国医疗保健方面的差异仍然存在,导致许多群体中出现了不必要的发病和死亡情况。7,8,9SDOH 加剧了这种部分群体(例如按种族或族裔、性别认同、年龄、残疾、社会经济地位或地理位置划分的群体)之间的健康结果差异,导致医疗保健缺乏公平性。10,11一些计划设置了目标和工具包,以实现卫生公平性、消除差异并改善所有美国人的健康。12,13,14,15多年来,药剂师一直作为社区重要成员开展工作,并定期与该社区中的患者交流,从而解决所有面临健康差异的群体的 SDOH,他们不仅在特殊药品和社区药房工作,而且也在综合健康服务网络、管理式医疗护理组织和以社区为基础的场所、医疗保健诊所和医生诊所以及医院提供服务。16,17
药剂师持有药学博士学位,通过持续应用药剂师的患者护理流程步骤来确定和满足医疗保健需求(见图 2)。18该护理流程不仅限于临床服务,还考虑到了患者的生活方式、偏好、信仰、功能目标和社会经济因素。此外,还会对患者的健康和功能状态、风险因素、健康数据、文化背景、健康素养和药物获取情况进行评估,以便制定以患者为中心的护理计划。无论执业环境或特殊药品规定如何,药剂师都坚持应用此流程。
图 2。药剂师的患者护理流程
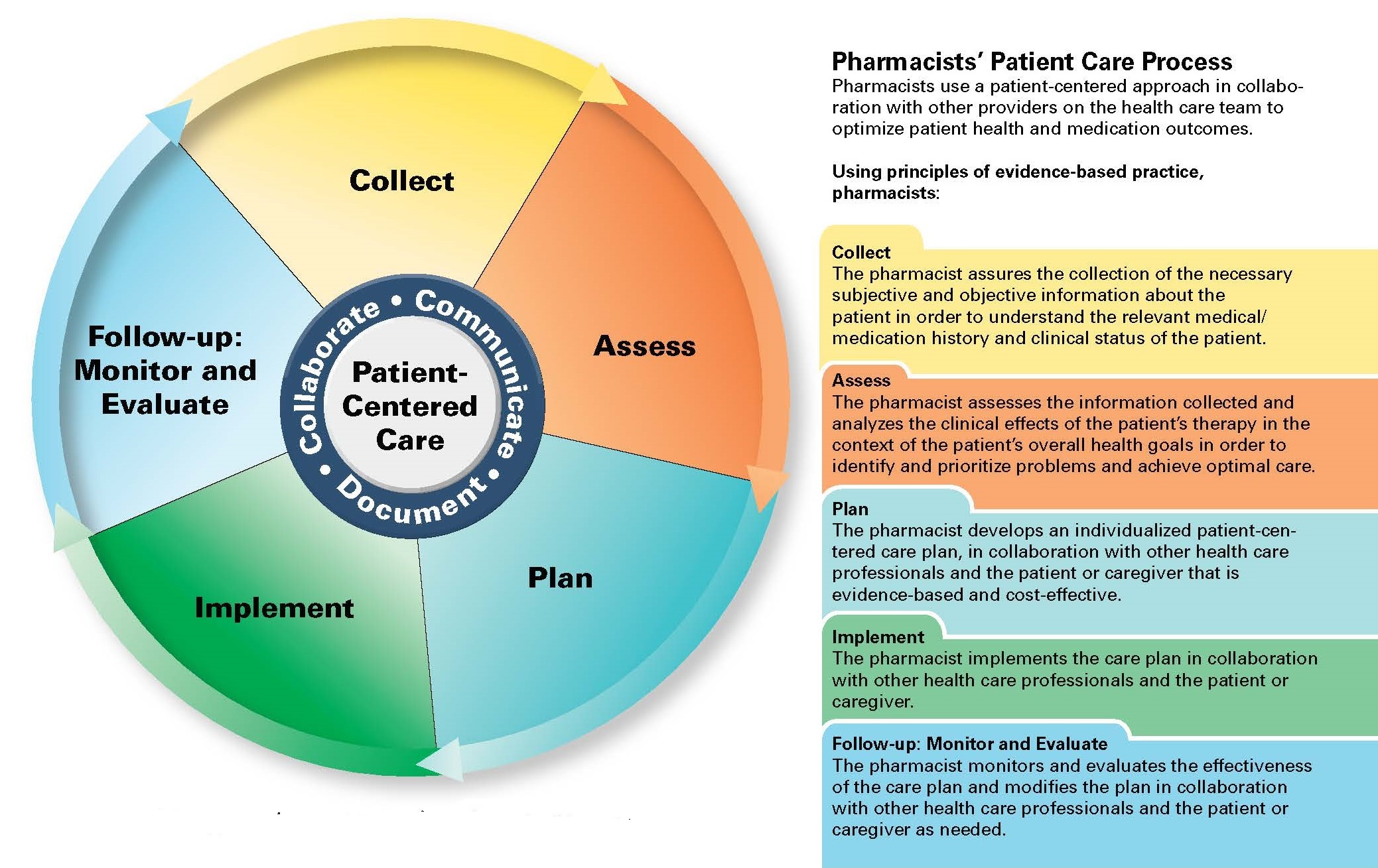
经药学从业人员联合委员会许可转载。18
在 48 个州和哥伦比亚特区,药剂师可以通过与医生签订合作实践协议来扩大其执业范围,以增加患者获得协调护理的机会。1合作实践协议因州而异,但医生委托给药剂师的职能一般会包括启动、修改或停止药物治疗以及安排、解释和监控实验室检测。美国公共卫生局向美国医务总监提交的一份报告为全面的药剂师患者护理服务提供了证据支持。19药剂师借助其药物和健康专业知识,可以提供慢性疾病管理、综合用药管理以及用药比对和评估等服务;帮助降低药物费用;协助检查处方;并促进家庭药物寄送和会诊,以及提供众多其他服务。20,21,22,23,24,25
药剂师与服务不足群体开展合作的卫生和健康促进领域包括参与健康筛查计划、促进自我保健、采取戒烟干预措施、提供孕前保健服务和管理疫苗接种。26,27,28,29这些举措改善了群体成员(包括医疗服务欠缺地区的成员)的生活,并有助于解决主要的健康差异。在 2006 年,美国公共卫生协会的政策认可了药剂师在公共卫生中所起的作用。30
卫生专业人员处于弥合健康差异的最前沿,可以通过将 SDOH 评估与临床实践中的干预措施相结合,在实现这一目标方面发挥直接作用,同时还提供临床预防服务,可解决烟草和物质使用障碍、营养、身体活动和肥胖等问题,并改善心理、口腔和性健康。9,31在 STEPS Forward 计划中,美国医学会支持将药剂师作为医疗保健团队中的必需成员,因为他们在药物治疗方面具备专业知识并且可提供服务。32在合理安排的情况下,药剂师(其中 55% 在社区药房中工作)33通过与医疗保健团队的其他成员协力合作,共同解决护理方面的差距。例如,明尼苏达州的一家社区健康中心发现,在将一名药剂师纳入临床团队后,达到预期药物治疗效果的患者(包括英语和非英语患者)的百分比提高了 24%。34此外,药剂师还可协助医生进行慢性疾病管理。慢性疾病(如糖尿病、高血压、血脂异常和肥胖),影响了 60% 的美国人,共占诊所医生会诊人数的 37%,并且该比例还在继续上升。35,36少数族裔和服务不足群体受到这些慢性疾病不成比例的影响,一种可能的解释是这些疾病与营养差异、适于行走的社区的可及性和烟草营销之间存在某种关联。37,38在一项为期一年的糖尿病患者研究中,接受药剂师药物治疗管理服务的非裔美国人中,有 56.3% 患者的糖尿病得到显著改善,而对照组的这一比例为 22.7%。21参与护理过渡的药剂师还可以帮助患者在住院后安全度过过渡期,并通过管理药物和教育患者,避免其在出院后 30 天内再次住院或到急诊室就诊。39因此,药剂师在临床预防服务、慢性疾病状态管理和护理过渡中的参与,对于消除健康差异至关重要。
随着收费从按服务收费模式日益向基于价值的收费模式转变,药剂师可以与其他医疗保健临床医生携手合作,以达到健康结果和成本指标。40基于价值的计划中有许多必要措施,例如国家质量保证委员会、医疗服务效果数据及信息收集系统以及药品质量联盟的措施,这些措施都涉及到药物的最佳使用。例如,一项专注于医生和药剂师合作管理血压的大型试验表明,分配到有药剂师的团队的个别患者,其血压更有可能会显著降低。202019 年公布的一项研究强调了这些结果,表明药剂师通过与社区医生和当地医生合作,可以改善 94% 去过诊所并接受药剂师会诊的非裔美国男性的血压,而对于那些去过诊所且被建议接受临床医生随访、但却未接受药剂师会诊的人,这一比例仅为 29%。41通过合作,药剂师和医生可以帮助优化群体中弱势患者的健康结果。
解决健康差异需要使用基于团队的多学科方法。本文所述的案例以及所提供的证据强调了药剂师在慢性疾病管理和预防、药物管理、卫生和健康以及患者支持等领域的作用。尽管药剂师、医生和其他临床医生可以分别解决健康差异问题,但只有通过协力合作,医疗保健系统才能更有效地解决健康差异问题并实现联邦政府设定的目标,改善所有美国人的健康。
US Department of Health and Human Services. Advancing team-based care through collaborative practice agreements: a resource and implementation guide for adding pharmacists to the care team. Centers for Disease Control and Prevention; 2017. Accessed June 30, 2020. https://www.cdc.gov/dhdsp/pubs/docs/CPA-Team-Based-Care.pdf
NCHHSTP social determinants of health. Centers for Disease Control and Prevention. Reviewed December 19, 2019. Accessed June 30, 2020. https://www.cdc.gov/nchhstp/socialdeterminants/index.html
Disparities. Healthy People, Office of Disease Prevention and Health Promotion, US Department of Health and Human Services. Accessed September 15, 2020. https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities
Career option profiles. American Pharmacists Association. Accessed August 20, 2020. https://www.pharmacist.com/career-option-profiles
Diabetes and health centers. Health Resources and Services Administration. Accessed August 23, 2020. https://bphc.hrsa.gov/qualityimprovement/clinicalquality/diabetes.html
Schneider EC, Sarnak DO, Squires D, Shah A. Mirror, mirror 2017: international comparison reflects flaws and opportunities for better US health care. Commonwealth Fund; July 2017. Accessed December 9, 2020. https://www.commonwealthfund.org/sites/default/files/documents/___media_files_publications_fund_report_2017_jul_schneider_mirror_mirror_2017.pdf
Maloney LR, Thompson KK, Vanderpool HK. ASHP’s role in eliminating health disparities. Am J Health Syst Pharm. 2005;62(18):1871.
Baciu A, Negussie Y, Geller A, et al, eds; National Academies of Sciences, Engineering, and Medicine. The state of health disparities in the United States. In: Communities in Action: Pathways to Health Equity. National Academies Press; 2017:chap 2.
Truman BI, Smith KC, Roy K, et al; Centers for Disease Control and Prevention. Rationale for regular reporting on health disparities and inequalities—United States. MMWR Suppl. 2011;60(1):3-10.
Carter-Pokras O, Baquet C. What is a “health disparity”? Public Health Rep. 2002;117(5):426-434.
Disparities. US Department of Health and Human Services. Accessed June 30, 2020. https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities
Reducing disparities in health care. American Medical Association. Accessed August 23, 2020. https://www.ama-assn.org/delivering-care/patient-support-advocacy/reducing-disparities-health-care
Attaining health equity. Centers for Disease Control and Prevention. Accessed August 23, 2020. https://www.cdc.gov/nccdphp/dch/programs/healthycommunitiesprogram/overview/healthequity.htm
About SDOH in healthcare. Agency for Healthcare Research and Quality. Accessed August 23, 2020. https://www.ahrq.gov/sdoh/about.html
Nessel J. 2020 trends in pharmacy care: value-based pharmacy and social determinants of health. Pharmacy Times. January 22, 2020. Accessed December 9, 2020. https://www.pharmacytimes.com/news/2020-trends-in-pharmacy-care-value-based-pharmacy-and-social-determinants-of-health
Chiara A. The expanding role of pharmacists: a positive shift for health care. Commonwealth Medicine blog. March 26, 2019. Accessed October 27, 2020. https://commed.umassmed.edu/blog/2019/03/26/expanding-role-pharmacists-positive-shift-health-care
Joint Commission of Pharmacy Practitioners. Pharmacists’ patient care process. May 29, 2014. Accessed June 30, 2020. https://jcpp.net/wp-content/uploads/2016/03/PatientCareProcess-with-supporting-organizations.pdf
Pharmacist Professional Advisory Committee. Improving patient and health system outcomes through advanced pharmacy practice: a report to the US Surgeon General, 2011. Commissioned Corps of the US Public Health Service. Revised September 27, 2019. Accessed August 23, 2020. https://dcp.psc.gov/osg/pharmacy/sc_comms_sg_report.aspx
Santschi V, Chiolero A, Colosimo AL, et al. Improving blood pressure control through pharmacist interventions: a meta-analysis of randomized controlled trials. J Am Heart Assoc. 2014;3(2):e000718.
The role of the pharmacist in public health. Policy No. 200614. American Public Health Association. November 8, 2006. Accessed June 30, 2020. https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2014/07/07/13/05/the-role-of-the-pharmacist-in-public-health
Green GR, Nze C. Language-based inequity in health care: Who is the “poor historian”? AMA J Ethics. 2017;19(3):263-271.
Choe HM, Standiford CJ, Brown MT. Embedding pharmacists into the practice. American Medical Association STEPS Forward. Accessed April 19, 2020. https://edhub.ama-assn.org/steps-forward/module/2702554
Occupational Outlook Handbook: pharmacists. US Bureau of Labor Statistics. Revised September 4, 2019. Accessed October 26, 2020. https://www.bls.gov/ooh/healthcare/pharmacists.htm#tab-3
Buttorff C, Ruder T, Bauman M. Multiple chronic conditions in the United States. RAND Corporation; 2017. Accessed September 20, 2020. https://www.rand.org/content/dam/rand/pubs/tools/TL200/TL221/RAND_TL221.pdf
Ashman JJ, Rui P, Okeyode T. Characteristics of office-based physician visits 2016. Centers for Disease Control and Prevention; January 2019. NCHS data brief 331. Accessed September 20, 2020. https://www.cdc.gov/nchs/products/databriefs/db331.htm
US Department of Health and Human Services. National Healthcare Quality and Disparities Report, 2018. Agency for Healthcare Research and Quality; September 2019. AHRQ publication 19-0070-EF. Accessed June 30, 2020. https://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/nhqrdr/2018qdr.pdf
American Pharmacists Association. Successful integration of pharmacists in accountable care organizations and medical home models: case studies. March 2020. Accessed June 30, 2020. https://www.pharmacist.com/sites/default/files/APhA_Medical_Home_ACO_Report_Final.pdf



