Medical Education
Aug 2016

The 2015 Institute of Medicine report on diagnostic error has placed a national spotlight on the importance of improving communication among clinicians and between clinicians and patients.1 The report emphasizes the critical role that communication plays in patient safety and outlines ways that pathologists can support this process. Despite recognition of communication as an essential element in patient care, pathologists currently undergo limited (if any) formal training in communication skills. To address this gap, we at the University of Washington Medical Center developed communication training with the goal of establishing best practice procedures for effective pathology communication. The course includes lectures, role playing, and simulated clinician-pathologist interactions for training and evaluation of pathology communication performance. Providing communication training can help create reliable communication pathways that anticipate and address potential barriers and errors before they happen.
In 1977 two 747 aircraft crashed on the runway in Tenerife, the worst disaster in aviation history. Root cause analysis identified miscommunication due to cross-cultural language variations and improper terminology usage among a Dutch KLM crew, an American Pam Am crew, and a Spanish air traffic controller as the primary cause of 583 passenger deaths. The National Aeronautics and Space Administration (NASA) conducted a study of jet transportation accidents between 1968 and 1976 and concluded that pilot error was more likely due to failures in team communication and coordination than technical proficiency.2 Later studies identified “communication problems” as a causal factor in about 70 percent of airline accident reports received at that time.3 High reliability industries, like aviation, have implemented standardized communication protocols, safety checklists, and simulation training to ensure robust, open, and effective communication channels. Unfortunately, the health care industry has been relatively slow to acknowledge the key role of communication in keeping patients safe.
Accurate and precise communication is a critical responsibility throughout diagnostic processes. A timely diagnosis is meaningless unless important information reaches both health care professionals and patients in an interpretable and actionable manner. In an 11-year study of sentinel events (2004-2015), the Joint Commission (JC) highlighted the importance of effective communication in medicine.4 Consistent with the NASA results, ineffective communication was determined to be one of the root causes of 66 percent of all reported sentinel events.
The complexities of coordinating multiple specialists’ communications can serve as a barrier to clear and timely communication. Whether and when critical information is effectively transferred is influenced not only by the method of communication but also by hierarchies and power dynamics within and among medical teams. Information must pass both horizontally between services (e.g., anesthesia, surgery, pathology) and vertically according to the flow of authority and status among attending physicians, residents, nurses, and technical staff. Vertical hierarchies are accentuated in teaching institutions and can powerfully influence how critical information is communicated. In the JC study, both communication and human factors (including orientation and training) were leading root causes of errors.4 Lack of attention to robust communication standards in teaching hospitals, where inexperienced trainees rotate through services, can also create potential for serious medical error.
Traditionally, there has been little attention to teamwork and communication skills in pathology and laboratory training. The lack of focus on developing effective communication skills represents a major gap in the education of pathologists, as lack of standardized expectations for conversations and explicit communication training could contribute to errors in information transfers between pathologists and other clinicians. Currently, pathology residents learn how to communicate with other medical professionals informally, typically by observing attending pathologists communicate. This poses two learning challenges. First, attending pathologists vary widely in their communication styles and might not be modeling communication well. Second, learning communication skills through apprenticeship is inefficient compared to learning them through an independent communication course, especially since traditional pathology apprenticeships do not focus formally on communication methods.
With these educational barriers in mind, we developed an interprofessional communication course in 2012 for pathology residents and fellows taught at least annually at the University of Washington Medical Center. The course is partially based on the TeamSTEPPS® program.5 TeamSTEPPS is an evidence-based teamwork system developed by the Agency for Healthcare Research and Quality (AHRQ) aimed at optimizing communication and teamwork skills among health care professionals. This pathology communication curriculum includes formally structured learning opportunities, such as lectures, role playing, simulated clinician scenarios; and didactic skill-building sessions that emphasize core communication concepts and principles. The course focuses on the current standards for the basics of communication, obstacles to communication, and communication of serious pathology errors.6, 7, 8
Communication basics. Before communication training, many trainees failed to use standard verbal elements during communication of significant or unexpected surgical pathology findings (critical values). For example, trainees often failed to identify themselves by name and position or did not request that the receiver repeat the diagnostic information to ensure information was received and understood. To address these communication gaps, our training—both traditional didactics and hands-on learning modules—emphasizes communication elements that should be present in all communications that can influence patients’ care. These include self-identification by name, position and department; confirmation of name and role of the clinician or staff to whom information is delivered; the name of the patient; the type of procedure; and involved patient body site. Optimal information transfer must include clear identification of the purpose of the communication and, for diagnoses, concise, unambiguous, and accurate delivery. To confirm that the message was received and understood, a “check back,” or request that the receiver repeat the diagnostic information back to the trainee, is required. The check back ensures that the receiver fully understands the content of the communication and accepts responsibility for either acting on or delivering the information to be used in appropriate patient care. Additional requirements for communications include inquiring whether the receiver has additional questions or concerns as well as demonstrated professional demeanor.
Tools, such as a framework for structuring communication, are also introduced to provide standardized approaches and set expectations regarding which information should be communicated, how it should be conveyed, and verifying that it is understood as intended. The elements of a proper information transfer are also introduced and practiced. During a proper critical information transfer, the trainee must ensure that the receiver is aware of and has accepted responsibility for the transferred information. When the trainee is uncertain about the communication, it is the trainee’s responsibility to clarify as much as possible and to eliminate sources of ambiguity before a conversation is complete. In addition to including the correct and complete elements of a communication, an information transfer requires acknowledgement by both parties that a transfer of critical information has occurred, especially in the face of communication obstacles.
Obstacles to communication. Concise, clear, and effective communication can be difficult even under optimal conditions. During training in minimizing obstacles to communication, residents practice strategies for communicating clearly, such as avoiding environmental distractions, navigating variations in communication styles, and responding to unexpected questions, conflict, or lack of information. Practicing pathologists are familiar with the most common obstacles encountered during information transfer. For example, a common question in the frozen section setting is whether a procured tumor is primary (e.g., lung, ovary, GI) or represents a metastasis to the organ. When challenged with verifying information about a procured tumor in simulation training, many trainees gave confusing or inappropriate answers. Providing trainees with exposure to common barriers prior to encountering them during a critical conversation affords them opportunities to practice difficult communications in a less stressful environment.
Communication of serious errors. Perhaps the most challenging communications involve communicating serious pathology errors to patients and the clinicians treating them. This is a skill that we believe must be practiced and refined in advance of actual disclosures of errors. Error disclosure communication training includes introduction to the key elements of error disclosure content that both treating clinicians and patients would like communicated to them after an error occurs.9, 10, 11 Following errors, treating clinicians and patients want an explicit statement that an error occurred; information about why the error happened and how recurrences will be prevented; an apology, including an expression of sympathy for all adverse events; and plans for follow-up. Resident physicians undergo didactic training, simulated phone conversations with clinicians, and in-class role playing emphasizing these key elements during their error disclosure module.12, 13, 14
Both before and after completing the course, residents communicate with trained simulated clinicians by phone using scripted scenarios, which are designed to give residents opportunities to practice communication skills ranging from diagnosis reporting to conflict resolution and error disclosure. Audio recordings of resident interactions with simulated clinicians are provided to the residents to enhance performance feedback and allow self-assessment. Checklists are often used in simulation-based medical education to enhance training and scoring of communications. In order to develop a checklist for determining the proper performance of the individual steps in critical value communications, we analyzed audio communications in terms of their elements and individual practice components using data from our first class. The checklist was refined in subsequent classes for resident evaluation. The completed checklist of 15-20 elements outlines key communication components for evaluating resident performance (see figure1).
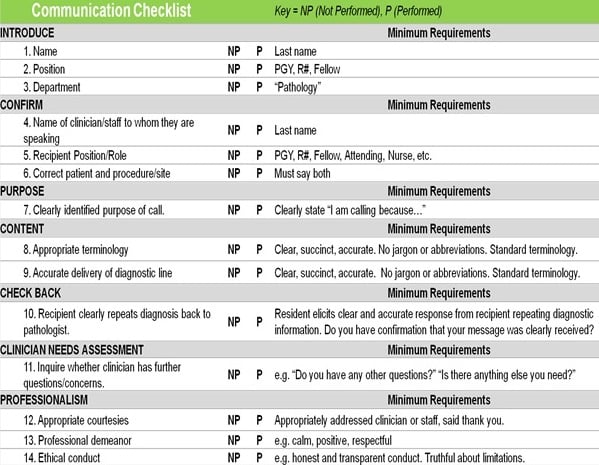
Figure 1. Checklist for critical value pathology communications developed at the University of Washington.
Pre- and posttests of communication skills and post-course evaluation forms demonstrate both objective and subjective improvements in critical value communication skills among resident physicians. Based on pretest and posttest performance averaged over several classes, overall performance on communication improved approximately 15 percent after training. We found that the combination of lectures and hands-on exercises was most effective at helping residents learn to use standard communication elements during critical value conversations. Residents also reported increased confidence in their ability to communicate in difficult situations after training and increased awareness of flaws in their pretest performance as they completed training.
Our resident communication course has provided us with valuable insight into how a simulation-based communication training course can improve residents’ skill in transferring information during critical value conversations. Miscommunications can be reduced by ensuring that introductions are performed, content is clear and complete, and immediate acknowledgement of information receipt is routinely solicited. Exposure to barriers frequently encountered during information transfer can also help mitigate miscommunication of critical patient information. Most importantly, formal communication training serves to emphasize both the connection between communication and medical error and the frequency of miscommunications. Such training allows participants to practice improvement strategies and a repertoire of skills to assist them in daily critical communications.
Balogh EP, Miller BT, Ball JR, eds; Institute of Medicine Committee on Diagnostic Error in Health Care. Improving Diagnosis In Health Care. Washington, DC: National Academies Press; 2015.
Cooper GE, White MD, Lauber JK, eds; National Aeronautics and Space Administration. Resource Management on the Flight Deck. http://ntrs.nasa.gov/archive/nasa/casi.ntrs.nasa.gov/19800013796.pdf. Published March 1980. Accessed April 25, 2016.
Connell L. Pilot and controller communications issues. In: Kanki BG, Prinzo OV, eds. Methods and Metrics of Voice Communications. Washington, DC: Office of Aviation Medicine; 1996:19-28. https://www.faa.gov/data_research/research/med_humanfacs/oamtechreports/1990s/media/AM96-10.pdf. Accessed April 25, 2016.
Joint Commission. Sentinel event data: root causes by event type, 2004-2015. http://www.jointcommission.org/assets/1/18/Root_Causes_by_Event_Type_2004-2015.pdf. Accessed April 25, 2016.
Agency for Healthcare Research and Quality. TeamSTEPPS®: strategies and tools to enhance performance and patient safety. http://www.ahrq.gov/professionals/education/curriculum-tools/teamstepps/index.html. Published May 2016. Accessed April 25, 2016.
Joint Commission. Joint Commission Perspectives. 2012;32(8).
Truog RD, Browning DM, Johnson JA, Gallagher TH. Talking with Patients and Families about Medical Error: A Guide for Education and Practice. Baltimore, MD: Johns Hopkins University Press; 2011.
Dintzis SM, Clennon EK, Prouty CD, Reich LM, Elmore JG, Gallagher TH. Pathologists’ perspectives on disclosing serious pathology error. Arch Pathol Lab Med. In press.