History of Medicine
Feb 2025
Peer-Reviewed

Ann Lohman, a midwife in the 1800s also known as Madame Restell, deserves our attention following the US Supreme Court decision in Dobbs v Jackson Women’s Health Organization in June 2022. As abortion regulations change, it is important that health care communities learn from past experiences. This article examines the historical context in which Lohman practiced and draws out key lessons to be applied today.
The 19th-century midwife Ann Lohman deserves our attention as clinicians practicing medicine following the 2022 US Supreme Court decision in Dobbs v Jackson Women’s Health Organization, which overturned Roe v Wade and thus ended federal protections for the right to legal abortion.1 In the 1800s in New York City, a similar time of legal flux for abortion, Lohman, under the name of Madame Restell, offered vital reproductive health care—including abortion services—to women for nearly 40 years. A controversial figure, she was publicly ridiculed as “notorious” and described as growing rich by the “practice of a nefarious business.”2
During our current time of social and legal change, what allowed faculty and preclinical medical students at our Florida medical school to openly discuss the contentious topic of abortion was reading My Notorious Life,3 a novel based on the life of Ann Lohman. This article examines the historical context in which Lohman practiced, including resolutions and advocacy of the newly minted American Medical Association (AMA) and laws criminalizing abortion. Additionally, the article details the evolution of the fields of midwifery and obstetrics and of medical practice and techniques for abortion. At a time when laws regulating abortion are again in flux, it is important that health care communities learn from their history and past experiences to inform current practice.
Some details about Lohman’s life, such as date of birth, date of first marriage, and first husband’s date of death, are unclear due to contradicting information in various primary and secondary sources.2,4,5,6 It is known that Ann, her first husband, Henry Summers, and daughter, Caroline, moved to the United States in 1831 from England.2,4,6,7,8 After Ann was widowed in 1831 or 1833, she began to work as a seamstress.5,6,7,8 She remarried in 1833, becoming Ann Lohman. Six years later, in 1839, Lohman listed her first advertisement as Madame Restell in the New York Sun.2,5,6,7,8 Sources differ on where Lohman learned midwifery, with her first advertisement saying she learned it from her grandmother,5 although others theorize she learned it from neighboring physician and pill compounder, Dr William Evans.4,6 As Madame Restell, Lohman sold abortifacients and performed procedural abortions2,8—this article uses the term abortion to indicate medication or procedural termination of pregnancy.
As Lohman’s practice became more successful and lucrative, competitors—Dr Ward, Mrs Mott, Mrs Bird, Dr Monroe, and Catherine Costello—joined the reproductive health care market by advertising abortifacients to treat “menstrual stoppage.”7 Neither Costello nor Lohman were physicians, although they advertised themselves as “female physicians.” It is unknown whether Drs Ward and Monroe were trained physicians.7 Lohman opened a boardinghouse where patients could give birth and could also pay an additional fee for her to facilitate adoption.4 In this way, Lohman facilitated choices—abortion, birth, and adoption—for her patients.
Practicing during a time in which laws regulating abortion were changing, Lohman served a 1-year sentence from 1847 to 1848 for performing a procedural abortion.2 She was arrested a second time and released in 1856.2 The year following her second husband’s death, Lohman was arrested for a third time for selling abortifacients.2 Lohman died of suicide in 1878 at age 65, just prior to her scheduled trial.2 Her story highlights the fear experienced by many current-day abortion providers as they navigate a volatile and often confusing legal landscape.
In colonial America, midwives were prominent, respected community members who provided the majority of obstetric care.9 Midwifery was primarily provided by women, although a midwifery school led by a male, Dr William Shippen, Jr, opened in 1762.9 At the time, generalist medical care required no formal education and was provided by both men and women.9 As medical schools began to open in the United States, starting in Philadelphia in 1765, male physicians slowly replaced midwives in attending to the care of upper-class patients, and women were relegated to the confines of providing midwifery services.9
Common law guided early American abortion practices. In the absence of modern-day pregnancy tests, pregnancy was not confirmed and fetal existence was not recognized before “quickening” (ie, feeling fetal movement).10 At that time, prior to quickening, to be pregnant was to carry an “inert non-being” or a “potential for life rather than life itself,” which was not a living soul.10 That quickening was well accepted as marking the beginning of fetal existence in the United States was evident in the contrast between English laws (from which many American laws originated) criminalizing abortion prior to quickening and laws in the early 1800s in the United States that upheld the quickening doctrine—or the idea that fetal existence did not occur until this point in the pregnancy.10 In 1812, the Massachusetts Supreme Court dismissed criminal abortion charges because the woman had not experienced quickening.10 This decision set the legal precedent that stood through 1850: that an abortion before quickening was not criminal.10 On the other hand, providing an abortion after quickening was illegal; in New York State, abortion after quickening could be punished with a $100 fine and one year in prison.8
In early America, women presenting with amenorrhea were diagnosed with menstrual obstruction, which might be due to a number of causes, including pregnancy.10 The treatment for menstrual obstruction was to bring on the woman’s menses, which might have ended the pregnancy, just as a medication abortion does today. At the time, treatments for menstrual obstruction were considered appropriate medical practice.10 Thus, physicians and midwives at that time could be considered to be following the principle of beneficence, in that they were providing the standard of medical care, and of nonmaleficence, in that many treatments for menstrual obstruction were no more dangerous than childbirth.
Treatments for menstrual obstruction included various pills and powders. In New York City, Lohman commercialized traditional remedies used by enslaved midwives and Native Americans that were discussed in midwifery medical guides and textbooks and taught in medical schools at the time.10,11 Midwifery practices of enslaved African Americans consisted of application of “centuries-old African folk knowledge,” including placing poultices of petroleum jelly and quinine at the cervix; douching with alum water, water from boiling rusty nails, or turpentine; and oral intake of quinine tablets, turpentine, or laxatives such as pennyroyal or papaya seeds.11 Native Americans used black root and red cedar to induce abortion; red cedar was also known as savin or sabina and similarly used by colonial women.12 Other oral abortifacients included pills made of “ergot, calomel, aloe, black hellebore, or ergot mixed with oil of tansy,” which were called “female monthly regulating pills.”7 These treatments, which only worked some of the time, were deemed relatively safe by the clinical standards of that era.10 Furthermore, some physicians considered violent purgatives and poisons to be dangerous to the woman and ineffective.10
In the 1830s, abortion marketing in penny papers emerged, offering treatment of “suppression, irregularity, or stoppage of the menses” or “female obstruction.”7 Lohman advertised surgical abortions, with one advertisement citing a cost of $20 for poor women and $100 for the wealthy.8 Figures 1 and 2 are 1840s Lohman advertisements from the New York Herald; they show that while surgical abortion was legally precarious, it was openly advertised and sought out by women.13,14 Surgical abortions consisted of dilation of the cervix or rupture of the amniotic sac, causing uterine contraction and fetal expulsion. A surgical abortion was not considered to be more dangerous than childbirth, as “a physically produced abortion handled by a competent physician was not a fearsome process.”10
Figure 1. Madame Restell Advertisement in the New York Herald, April 13, 1840
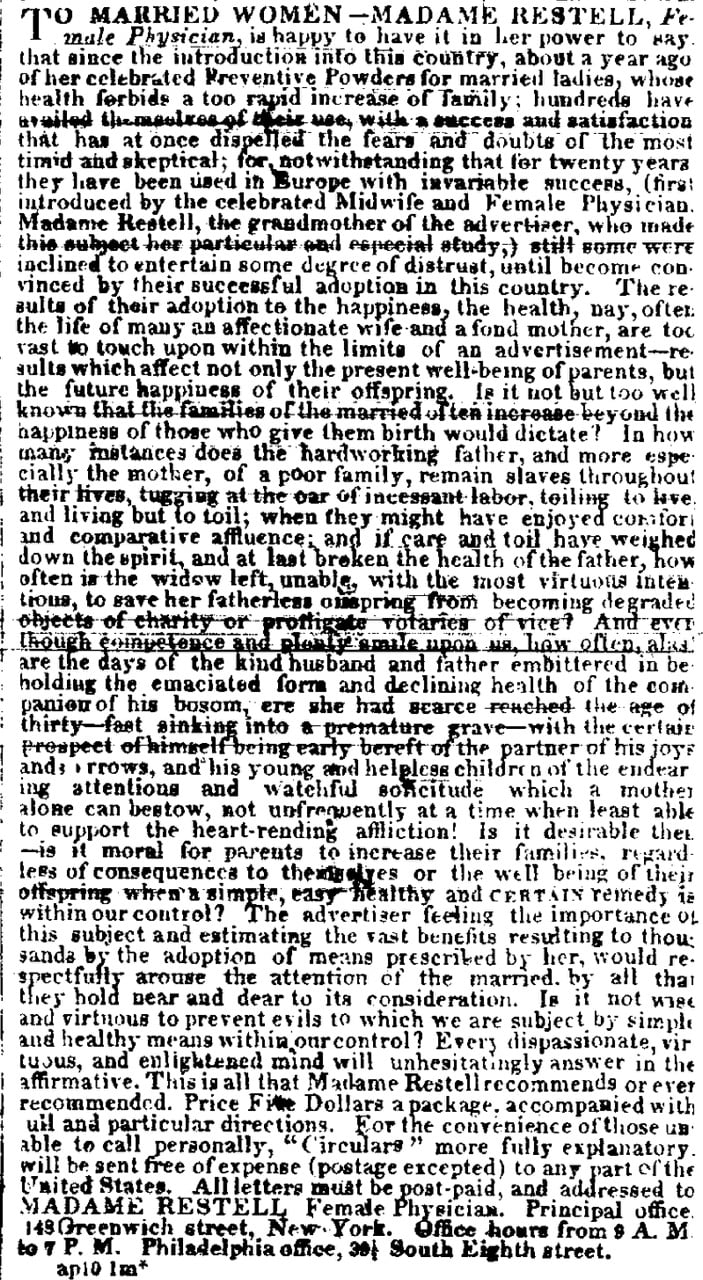
Reproduced from the Library of Congress.13
Figure 2. Madame Restell Advertisement in the New York Herald, September 7, 1842
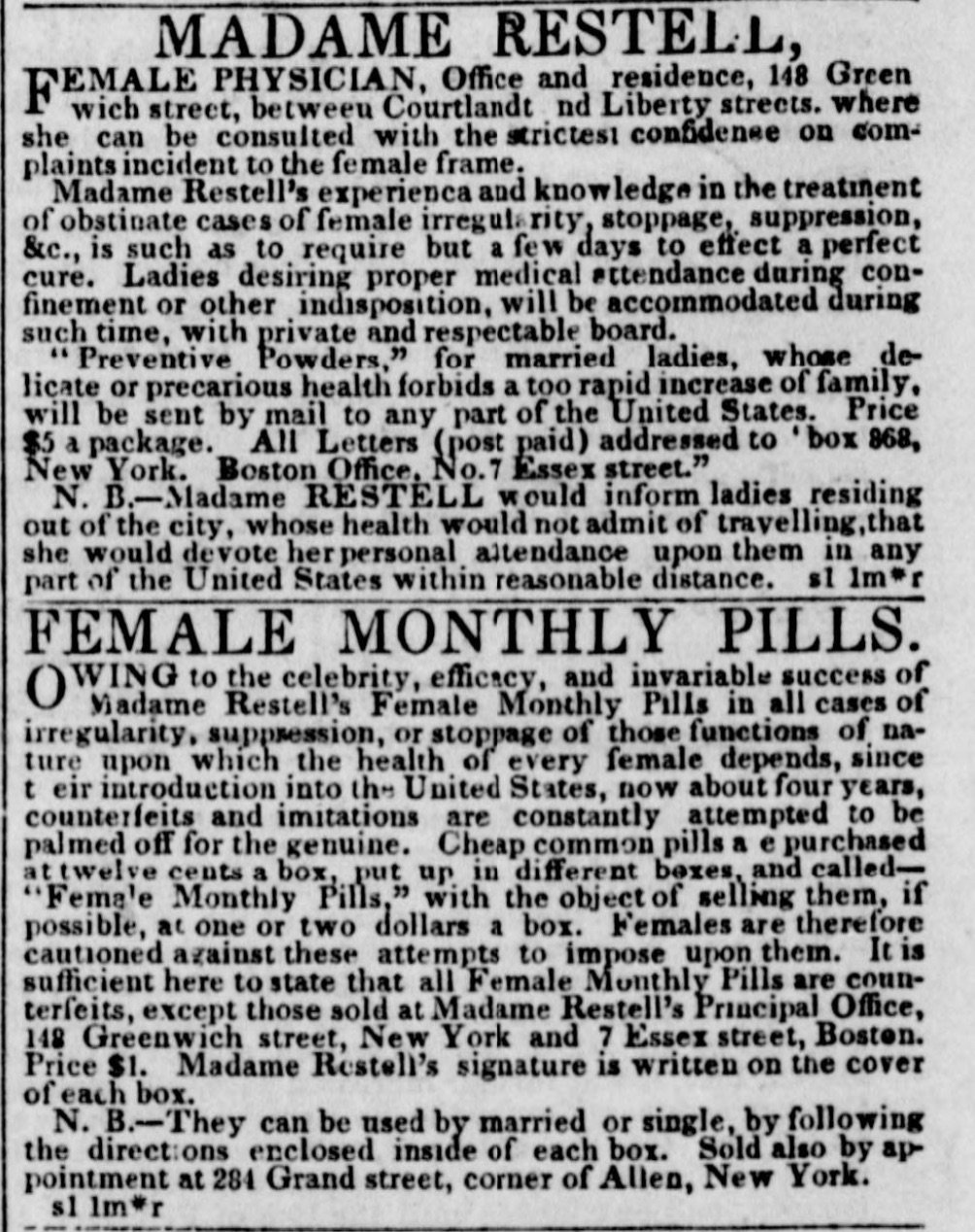
Reproduced from the Library of Congress.14
In 1847, the AMA was founded at the National Medical Convention in Philadelphia, where it sought to establish itself and the medical profession by detailing medical training and professional licensure.15 Medical school-trained physicians had “denounce[d] the amateurs”—including midwives and informally trained generalists—“who dominated the field” and explicitly sought to criminalize all abortion, which was, at that time, legal before quickening.16 Lohman, as a midwife without formal training who performed abortions, was among those targeted by these efforts.
The AMA’s motivations for criminalizing abortion were multipronged.16 Women sought abortions from skilled practitioners, and, because many physicians lacked skill in performing abortions, physicians might gain control over abortion by criminalizing it.16 With obstetrics evolving as a profession, midwives were viewed as competition who might decrease physician profit and societal standing.7 The AMA also espoused the argument that abortion was immoral and violated medical ethics in adopting a resolution referring to it as “unwarrantable destruction of human life.”17 By depicting abortion as evil, the AMA sought to uplift medicine as the standard of morality.16 A visual representation of this perspective is Figure 3, an 1847 sketch of Lohman hovering over a creature with a baby in its mouth, which was published in the National Police Gazette.18
Figure 3. The Female Abortionist, National Police Gazette, March 13, 1847
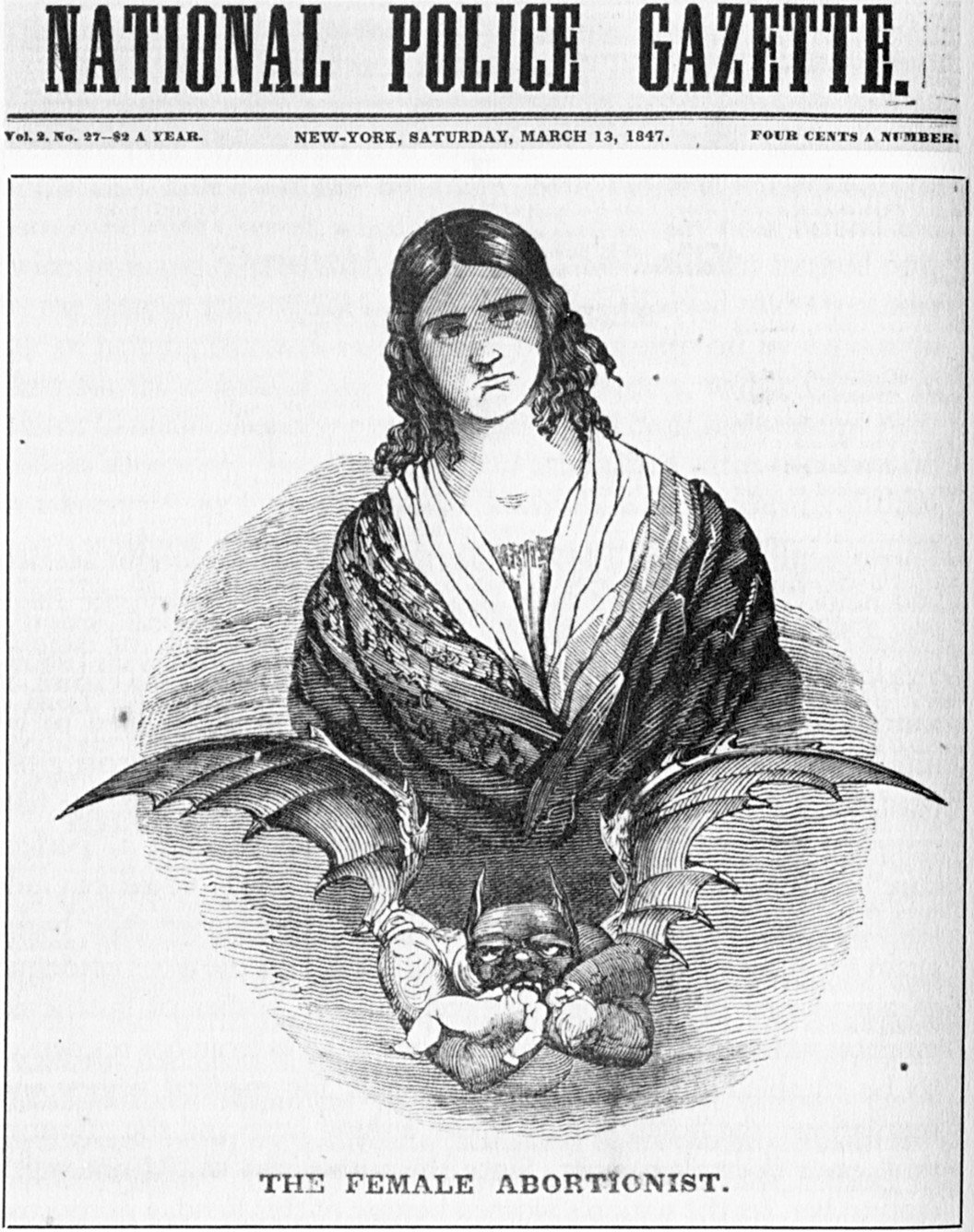
Reproduced from Wikimedia Commons.18
In 1859, the AMA unanimously adopted Dr Horatio Storer’s 4-page proposal, “Report on Criminal Abortion.”17 The report simultaneously recognized the social acceptance of abortion while deeming it immoral: “The heinous guilt of criminal abortion, however viewed by the community, is everywhere acknowledged by medical men.”17 Storer noted that physicians “are the physical guardians of women” and that abortion was “the wanton and murderous destruction of her child” and called on “governors and legislatures of several States, and, as representing the federal district, to the President and Congress” to carefully examine and revise the statutory and common law.17 The AMA formally espoused the idea that life begins at conception, rather than at quickening, and resolved to publicly protest abortion, lobby lawmakers to criminalize abortion, and enlist AMA-associated state medical societies in the cause.17 The AMA’s campaign resulted in the passage of over 40 anti-abortion statutes in state and territorial law codes between 1860 and 1880.16 Today’s increase in state-level abortion regulations is reminiscent of this period.
The AMA physicians declaring recommendations regarding the care of women’s bodies did so without a woman’s voice.15,17 While the 1859 AMA “Report on Criminal Abortion” was about women’s health care, there were no women authors. Similarly, the AMA campaign for abortion criminalization was led by men, especially Storer.1 In the 1847 and 1859 AMA proceedings, physicians are always referred to as “men,” whereas women are referenced as “wives” or “patients.”15,17 Today’s new legislation regulating abortion is similarly written and championed by primarily male politicians who are not familiar with its medical or procedural aspects.
In 1873, Anthony Comstock, Postmaster General special agent and Society for the Suppression of Vice secretary, proposed the federal bill that later that year became the Comstock Law, which criminalized the use of mail to communicate information about preventing conception.19 Comstock visited Lohman’s office twice under an alias to learn about her practice and buy an abortifacent.2 On his third visit, 5 years after the passage of the Comstock Law by Congress and 19 years after the AMA’s “Report on Criminal Abortion,” Comstock arrested Lohman for selling abortifacients.2 The New York Times reported on April 1, 1878, that Lohman was “driven to desperation” and “came to a violent end by cutting her throat from ear to ear.”2 The Comstock Law is being considered as one possible way for legislators to regulate access to abortion pills today. Although the Comstock Law is federal policy, some city and county ordinances state that mailing or receiving abortion medications is illegal.20
In 2020, Dr Meera Shah, chief medical officer of Planned Parenthood Hudson Peconic in New York State, wrote that “remaining silent about providing abortion care perpetuates the stereotype that abortion is unusual or deviant or that legitimate, skilled, intelligent doctors do not perform them.”21 Shah’s words invite a comparison with the mid-19th-century delegitimization of abortion in AMA proceedings as unskilled medical care and the derogatory language used to describe those who performed abortions, epitomized by the 1878 New York Times article referring to Lohman as “mysterious,” “notorious,” and “nefarious” for practicing abortion.2
Abortion regulations are once again changing. The Dobbs decision has allowed individual states to recriminalize abortion.1 Indeed, after the 2023 change to the US Food and Drug Administration Mifepristone Risk Evaluation Mitigation Strategy, which allows certified pharmacies to dispense mifepristone, 20 attorneys general posted communications to 2 major national pharmacy retailers citing the Comstock Act as criminalizing the mailing of abortifacients and asserting that their states could enforce the Comstock Act.20 Thus, in the wake of the Dobbs decision, the Comstock Act is again the word of law, and conservative interpretation could lead to federal prosecution of those mailing abortifacients or even medications that may threaten pregnancies, such as methotrexate.20
In Texas, Senate Bill 8 bans abortions after fetal cardiac activity is detected (approximately 6 weeks gestational age) and Senate Bill 4 makes it a felony, punishable by jail time and a $10 000 fine, for a physician to medically terminate a pregnancy after 49 days gestational age.22,23 A study that explored the effect on maternal morbidity of these 2 abortion restrictions implemented in 2021 found that women in Texas did not receive what was once standard of care,22 indicating that physicians could no longer practice beneficence and justice. In Texas, physicians observed women for an average of 9 days until patients experienced severe complications that threatened their lives, such as hemorrhage and infection.22 As a result, the Texas patients had nearly double the morbidity rate of women in states without abortion restrictions.22
In 2022, 160 years after its initial condemnation of abortion, the AMA adopted policies opposing abortion criminalization and supporting abortion access: “The AMA is steadfastly opposed to governmental interference in the practice of medicine, especially for well-established, medically necessary treatments. Patients and physicians need assurances that they won’t be accused of crimes for medically necessary treatment … that medically necessary treatment can be criminalized speaks volumes about these misguided abortion laws.”24 The AMA’s statement supports physicians practicing the standard of care, which is embedded in the ethical pillars of beneficence and nonmaleficence. Additionally, the AMA states that the decision to terminate a pregnancy “should be made privately within the relationship of trust between patient and physician.”25,26 In light of the Dobbs decision, the AMA is explicitly recognizing the sanctity and privacy of the patient-physician relationship, one which centers patient autonomy despite legal restrictions.
Lohman’s story remains relevant as we experience a movement towards limiting women’s bodily autonomy and access to reproductive care. Criminalization of abortion during Lohman’s lifetime parallels the restrictions occurring in the present day. Considering the motivations for and impact of laws restricting reproductive care during Lohman’s time provides a medium through which to further reflect on our current laws and their impact today.
Dobbs v Jackson Women’s Health Organization, 597 US 215 (2022).
End of a criminal life. New York Times. April 2, 1878. Accessed June 28, 2024. https://www.nytimes.com/1878/04/02/archives/end-of-a-criminal-life-mme-restell-commits-suicide-she-cuts-her.html
Manning K. My Notorious Life: A Novel. Scribner; 2013.
Wright J. Madame Restell: The Life, Death, and Resurrection of Old New York’s Most Fabulous, Fearless, and Infamous Abortionist. Hachette Books; 2023.
Carmack SD. Madame Restell: The True Story of New York City’s Most Notorious Abortionist. Her Early Life, Family, and Murder. Scattered Leaves Press; 2023.
Syrett NL. The Trials of Madame Restell: Nineteenth-Century America’s Most Infamous Female Physician and the Campaign to Make Abortion a Crime. New Press; 2023.
Kahler A. Madame Restell: the abortionist of Fifth Avenue. Smithsonian Mag. November 27, 2012. Accessed June 28, 2024. https://www.smithsonianmag.com/history/madame-restell-the-abortionist-of-fifth-avenue-145109198/
Mohr J. Abortion in America: The Origins and Evolution of National Policy, 1800-1900. Oxford University Press; 1978.
To married women—Madame Restell, female physician. Advertisement. New York Herald. April 13, 1840. Library of Congress. Accessed June 28, 2024. https://www.loc.gov/resource/ppmsca.02923/
Madame Restell, female physician. Female monthly pills. Advertisement. New York Herald. September 7, 1842. Library of Congress. Accessed June 28, 2024. https://www.loc.gov/resource/sn83030313/1842-09-07/ed-1/?sp=4&st=image&r=0.606,0.54,0.57,0.356,0
Proceedings of the National Medical Conventions, Held in New York, May 1846, and in Philadelphia, May 1847. American Medical Association; 1847. Accessed June 28, 2024. https://ama.nmtvault.com/jsp/PsImageViewer.jsp;jsessionid=DC1B9B2166D7B6EDC0D6008DCF63FC9A?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD000001%2F0039PROC
Minutes of the twelfth annual meeting of the American Medical Association. Trans Am Med Assoc. 1859;12:9-42. Accessed October 22, 2024. https://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000012
The female abortionist. Cover image. National Police Gazette. March 13, 1847. Wikimedia Commons. Accessed June 28, 2024. https://commons.wikimedia.org/wiki/File:National_Police_Gazette_Restell.jpg
Felix M, Sobel L, Salganicoff A. The Comstock Act: implications for abortion care nationwide. Kaiser Family Foundation. April 15, 2024. Accessed June 25, 2024. https://www.kff.org/womens-health-policy/issue-brief/the-comstock-act-implications-for-abortion-care-nationwide/
Shah M. You’re the Only One I’ve Told: The Stories Behind Abortion. Chicago Review Press; 2020.
ACOG responds to Texas SB 4. American College of Obstetricians and Gynecologists. Accessed November 13, 2022. https://www.acog.org/community/districts-and-sections/district-xi/advocacy/texas-sb4
O’Reilly KB. AMA holds fast to principle: reproductive care is healthcare. American Medical Association. November 17, 2022. Accessed June 26, 2024. https://www.ama-assn.org/delivering-care/public-health/ama-holds-fast-principle-reproductive-care-health-care
Schwartz PA. Opinion of the Council on Ethical and Judicial Affairs. American Medical Association; 2022. Accessed June 28, 2024. https://www.ama-assn.org/system/files/i22-ceja-reports.pdf
American Medical Association. Opinion 4.2.7 Abortion. Code of Medical Ethics. Accessed June 28, 2024. https://code-medical-ethics.ama-assn.org/ethics-opinions/abortion



{kind=link}