Medicine and Society
Aug 2024
Peer-Reviewed
The medical-legal partnership (MLP) and reproductive justice (RJ) movements both seek to solve complex problems, serve diverse populations with intersectional challenges, and resolve community conditions that impact people’s ability to reach their highest health potential. Yet MLPs have been overlooked as a strategy to advance reproductive health and justice. MLP has distinct advantages for advancing RJ, and many MLPs might already be doing RJ work without referring to it by name. By intentionally adopting an RJ strategy and explicitly addressing the unmet social and legal needs that limit people’s ability to plan their reproductive futures, MLPs can better serve their clients and contribute to the movement to combat reproductive oppression.
In June 2022, the US Supreme Court issued its decision in Dobbs v Jackson Women’s Health,1 overruling the constitutional right to abortion founded in Roe v Wade2 and radically transforming access to reproductive health care in the United States.1,2 As predicted, the decision has had disproportionate health impacts on people who face discrimination based on other axes of identity.3 These include Black, Indigenous, and people of color (BIPOC); people with lower incomes and fewer resources; noncitizens; minors; people with disabilities; and people with diverse sexual orientations and gender identities.4 Dobbs brought an end to nearly 50 years of abortion jurisprudence and standard medical practice.1 One year after the decision, 26 states had banned or were likely to ban abortion, thus rolling back access to care for 15.4 million women of color in these states.5 These consequences explain how the Dobbs decision has set back advocacy for reproductive justice (RJ).
RJ encompasses “the complete physical, mental, spiritual, political, social, and economic well-being of women and girls, based on the full achievement and protection of women’s human rights.”6 These human rights include rights to “maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.”7 The decision of whether or not to become a parent has broad implications for one’s health, income, career, education, and relationships.
Medical-legal partnership (MLP) is not typically framed as an intervention for RJ. This article seeks to fill that gap. MLP is a model of collaboration and joint advocacy between lawyers and health care practitioners who seek to improve social conditions that affect health and well-being.8 Many social determinants of health, including sociopolitical and legal systems that perpetuate generational inequity, shape poor health outcomes and cannot be resolved through medical care alone.9 Among them are unaffordable and substandard housing, utility shutoffs, food insecurity, erroneous denials of public benefits, and inadequate funding for public schools. MLP is an effective means to address health and justice gaps, especially for BIPOC and in communities with lower incomes.10,11 The communities that are most likely to access and benefit from the services of MLPs are the very communities that are disproportionately impacted by laws and policies restricting access to sexual and reproductive health care.12
The community conditions that impact reproductive freedom are so broad that many MLPs may be doing RJ work without referring to it by name. This article describes the distinct advantages of MLPs for RJ advocacy and argues that intentionally adopting RJ practices can help MLPs better meet their clients’ needs.
Roe framed the right to abortion as an individual’s choice of whether or not to have a child, without consideration of the social determinants that impact such a choice.2,13 Following Roe, the mainstream reproductive rights movement adopted a single-issue approach by focusing its advocacy solely on abortion and birth control “at the expense of a broader agenda.”14 This narrow approach and “choice” framework did not adequately recognize the ways in which racism, poverty, sterilization abuse, and other structures of subordination influence reproductive destinies, especially for people of color.13,14 In response, women of color advocated for a new, intersectional approach to reproductive rights that highlighted and challenged the structural barriers to reproductive freedom.15
The term reproductive justice was coined in 1994 by a group of Black women who saw the need to better articulate their realities in the movements for sexual and reproductive health.16 The RJ framework “analyzes how the ability of any woman [person] to determine her [their] own reproductive destiny is linked directly to the conditions in her [their] community—and these conditions are not just a matter of individual choice and access.”6 RJ integrates multiple issues and diverse constituencies to highlight how intersectional forms of discrimination contribute to reproductive oppression.6 RJ differs from mainstream reproductive rights advocacy because it includes reproduction and parenting and links abortion to other community-centered concerns.6 It unites social justice movements in organized messaging and powerful grassroots coalitions.17
Like the movement for health justice, which is associated with MLP,9 RJ seeks to eliminate structural inequities, uplift individuals and communities, and secure collective power.18 However, engagement between RJ and health justice is limited, contributing to the public discourse on reproductive health that focuses on abortion exclusively instead of broader issues of protecting bodily autonomy, deciding whether or not to have a child, and parenting in safe and sustainable communities.19 Sexual and reproductive health exceptionalism, which “siloe[s] off reproductive and sexual health from other health care needs,” is rooted in bias and stigma.20 Greater alignment between health justice and RJ can build a more powerful and mainstream movement that better meets the needs of the most marginalized people, families, and communities.8,18
The MLP and RJ movements are aligned in several ways: they seek to solve complex social problems that “transcend the borders of traditional policy domains, involve a wide variety of actors across different scale levels and resist our attempts to solve them”21; they serve diverse populations with intersectional challenges8; and they highlight and resolve community conditions that impact people’s ability to reach their highest health potential by preventing legal and reproductive health crises, respectively. Because of these similarities, it is very likely that most MLPs are advancing RJ but have not framed their work in this way.
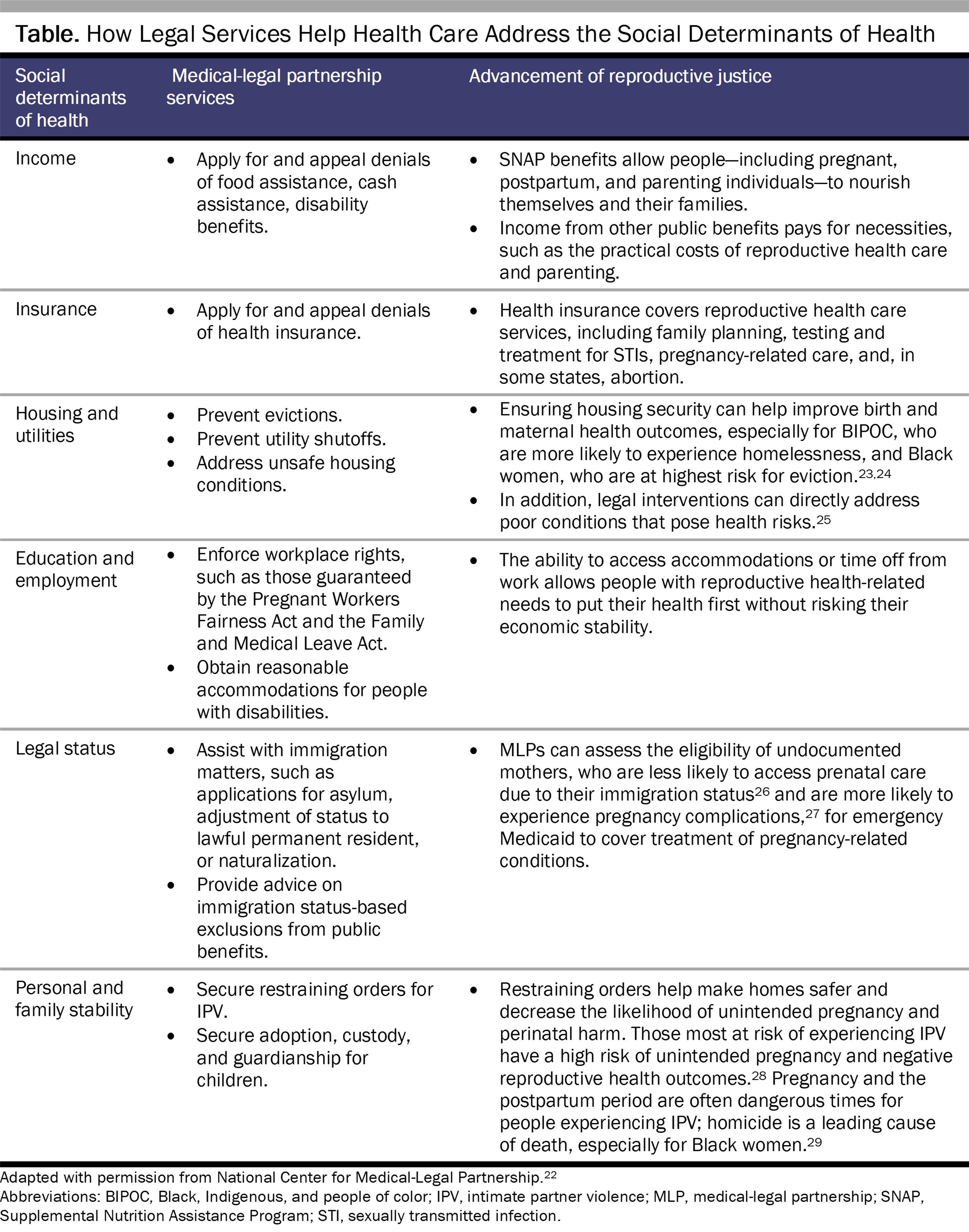
Linking RJ priorities to the types of services that MLPs provide reveals how MLPs help to advance RJ. In the literature on MLPs, I-HELPTM refers to advocacy relating to income and insurance, housing and utilities, education and employment, legal status, and personal and family stability.22 It is often cited to describe the legal domains in which MLPs operate. The chart below, adapted from the National Center for Medical-Legal Partnership,22 shows how MLPs can intervene to address unmet social and legal needs that limit reproductive freedom, thereby advancing RJ.
Presently, there is unprecedented interest in combatting reproductive oppression.5,30 While inequities in abortion access existed long before Dobbs, the United States has seen worsening maternal and infant health outcomes, attacks on gender-affirming care,31 and growing maternal health care deserts in the year since the decision was issued.32,33 In the 26 states that had already banned or were likely to ban abortion 12 months after Dobbs,5,34 residents face unique barriers to reproductive freedom. As noted, these barriers often fall disproportionately on BIPOC and people with lower incomes.5
Yet the potential for MLPs to advance reproductive health and justice is underappreciated.35,36 There is a notable overlap in the communities that utilize MLP services and the communities that are most harmed by reproductive oppression.5,37 For example, the large majority of people who accessed legal aid services in 2021 were women, roughly a quarter of whom were aged 18 to 35 years37; in June 2023, more than 36 million women of reproductive age lived in states that had banned or were likely to ban abortion.5 However, while 60% of MLPs served a “general population” in 2016, only 9% targeted pregnancy as a specific health condition for MLP intervention.38 Screening for health-harming legal needs and directing legal services to pregnant patients would align more MLPs with RJ. In addition, nearly half of legal aid clients identify as Black, Hispanic of any race, or Native American,39 and Black and Native American women are most likely to live in states that ban abortion, with Latinas being the largest group harmed by bans.5 Failing to recognize how intersecting identities and experiences may structurally disadvantage clients and impact their reproductive future neglects the holistic needs of clients and forgoes the power of MLPs to create change in lives, communities, and policies.
One of the advantages of MLPs as a tool for RJ is that the different strategies MLPs employ—direct representation, institutional change, and policy advocacy—provide several avenues of action for RJ.
Direct representation. On the individual client level, MLP staff can stay informed on issues impacting reproductive freedom in their community and build connections with local RJ organizations that may be better equipped to handle such issues when they arise among MLP patients-clients. For example, MLPs can work in tandem or in partnership with resource centers for people experiencing intimate partner violence. Additionally, expanding MLPs into abortion clinics or through collaboration with abortion funds (organizations that provide logistical and financial support to people seeking abortions)40 creates opportunities for MLPs to work with pregnant, postpartum, and post-pregnancy clients who are facing significant social and economic challenges and who otherwise may not find their way to a legal aid office.41 Lawyers and health care practitioners (ob-gyns, doulas, and others) can build relationships and partnerships with each other in order to reach specific populations with RJ-related legal needs.
MLP staff who work directly with patients-clients can take measures to acknowledge their sexual and reproductive needs. Incorporating RJ in MLP may be as simple as providing access to condoms in a medical or legal services waiting room, which may indicate that the medical or legal professional is comfortable discussing social and legal needs relating to sexual and reproductive health, thereby opening the door to patient-client-initiated conversations about those topics. MLP staff can also create processes for identifying compelling client stories and sharing them (with informed consent) with legislators or in op-eds for greater impact.
Attorneys can take further measures by counseling clients on the legality and availability of abortion care, over-the-counter birth control, and emergency contraception.42 It is worth noting that while MLPs funded by the Legal Services Corporation (LSC) are not permitted to help clients access abortion care, this restriction does not apply to other types of reproductive health care, such as contraceptives or sexually transmitted infections testing and treatment.43 MLPs that do not receive LSC funding, such as MLPs in law school clinics or non-LSC affiliates of legal aid organizations, are not subject to these restrictions.
Institutional change. In an effort to create institutional change within health care systems, MLPs can educate health care practitioners on existing laws and policies related to sexual and reproductive health,8 perhaps in consultation with the health system’s general counsel’s office. Trainings may cover how to prepare for changes in the law on medication abortion and birth control,44 current case law interpreting the legal definition of an emergency abortion,45 or how patients can access doula coverage under Medicaid.46
Policy advocacy. With respect to policy change, lawyers and health care practitioners—as stewards of power—are well-positioned to advocate for policies that make health care more equitable, accessible, effective, and affordable. For example, they can encourage state policy makers to adopt health-promoting options in federal programs, such as pregnancy-related Medicaid extensions.47 Lawyers and health care professionals can also use their experience working with individual patient-clients and the specific health injustices those patients-clients encounter to inform the policy changes for which they advocate. In several contexts, MLPs have used this “patient-to-policy” strategy to successfully persuade policy makers to enact change.48
Although there are MLPs advancing RJ by working in perinatal settings36—and 9% of MLPs target pregnant individuals for MLP services, as reported in a 2016 survey38—it is rare or unheard of for MLPs to explicitly make the connection between their work and RJ beyond perinatal care. Excluding certain components of sexual and reproductive health care, such as abortion and birth control, from the MLP space reflects and reproduces stigma, invites partisan divide into the legal-health space, and abandons communities who may need these essential services. When MLPs fail to consciously implement RJ practices or align their work with the RJ movement, they risk creating an environment where clients do not feel safe to express the full scope of their needs.49
In the Supreme Court’s opinion in Dobbs, the majority claimed that returning the “issue of abortion” to the states would allow the rule of law to prevail.1 Instead, Dobbs created a geographic patchwork of laws regulating abortion as well as confusion among patients and clinicians about the permissibility of reproductive health care.50,51 As a movement founded on the principle that leveraging legal services in health care settings can address structural problems at the root of health inequities, MLPs can play a role in mitigating reproductive oppression compounded by Dobbs.52 The vision on which RJ was founded—reproductive freedom for all—is increasingly under attack, and MLPs can support the movement by adopting an intentional RJ strategy and explicitly addressing the unmet social and legal needs that limit people’s ability to plan their reproductive futures.
Dobbs v Jackson Women’s Health Organization, 142 S Ct 2228 (2022).
Roe v Wade, 410 US 113 (1973).
Human rights crisis: abortion in the United States after Dobbs. Human Rights Watch. April 18, 2023. Accessed September 23, 2023. https://www.hrw.org/news/2023/04/18/human-rights-crisis-abortion-united-states-after-dobbs#_Toc132207240
Fuentes L. Inequity in US abortion rights and access: the end of Roe is deepening existing divides. Guttmacher Institute. January 17, 2023. Accessed February 4, 2024. https://www.guttmacher.org/2023/01/inequity-us-abortion-rights-and-access-end-roe-deepening-existing-divides
Robbins KG, Goodman S, Klein J. State abortion bans harm more than 15 million women of color: Dobbs impact felt nationwide. National Partnership for Women and Families; 2023. Accessed September 23, 2023. https://nationalpartnership.org/wp-content/uploads/2023/02/state-abortion-bans-harm-woc.pdf
Ross L. What is reproductive justice? In: Reproductive Justice Briefing Book: A Primer on Reproductive Justice and Social Change. Pro-Choice Public Education Project; SisterSong Women of Color Reproductive Justice Collective; 2007. Accessed September 23, 2023. https://www.law.berkeley.edu/php-programs/courses/fileDL.php?fID=4051
Ross L, Solinger R. Reproductive Justice: An Introduction. University of California Press; 2017.
Makhlouf M. Addressing racism through medical-legal partnerships. Bill of Health. September 24, 2020. Accessed September 23, 2023. https://blog.petrieflom.law.harvard.edu/2020/09/24/addressing-racism-medical-legal-partnerships/
Benfer E, Bhandary-Alexander J, Cannon Y, Makhlouf M, Pierson-Brown T. Setting the health justice agenda: addressing health inequity and injustice in the post-pandemic clinic. Clin Law Rev. 2021;28:45-84.
Cannon YZ. Medical-legal partnership as a model for access to justice. Stanford Law Rev Online. 2023;75:73-88.
Abrams Z. Abortion bans cause outsized harm for people of color. Monitor on Psychology. 2023;54(4):24. Accessed February 4, 2024. https://www.apa.org/monitor/2023/06/abortion-bans-harm-people-of-color
Ziegler M. The price of privacy, 1973 to the present. Harv J Law Gend. 2014;37:285-329.
Murray M, Shaw K, Siegel RB, eds. Reproductive Rights and Justice Stories. Foundation Press/West Academic; 2019.
About. Liberate Abortion Campaign. Accessed September 23, 2023. https://www.liberateabortion.org/about
Wiley LF, Yearby R, Clark BR, Mohapatra S. Introduction: what is health justice? J Law Med Ethics. 2022;50(4):636-640.
Rebouché R. Health justice meets reproductive justice. Bill of Health. September 28, 2021. Accessed September 23, 2023. https://blog.petrieflom.law.harvard.edu/2021/09/28/reproductive-justice-health/
Mainstreaming reproductive health. UCLA School of Law. Accessed September 23, 2023. https://law.ucla.edu/academics/centers/center-reproductive-health-law-and-policy/mainstreaming-reproductive-health
How legal services help the health care system address social needs. National Center for Medical-Legal Partnership. Accessed September 23, 2023. https://medical-legalpartnership.org/response/i-help/
Mhatre N. Moms and babies series: homelessness hurts moms and babies. National Partnership for Women and Families; National Birth Equity Collaboration; 2021. Accessed September 23, 2023. https://nationalpartnership.org/wp-content/uploads/2023/02/homelessness-hurts-moms-and-babies.pdf
Blumenthal C. The disproportionate burden of eviction on Black women. Center for American Progress. August 14, 2023. Updated August 29, 2023. Accessed February 4, 2024. https://www.americanprogress.org/article/the-disproportionate-burden-of-eviction-on-black-women/#:~:text=Ashfaq%20Khan-,Black%20women%20are%20at%20greatest%20risk%20of%20eviction,United%20States%20are%20Black%20women
Bhasin A. Moms and babies series: a systemic failure—immigrant moms and babies are being denied health care. National Partnership for Women and Families; National Birth Equity Collaboration; 2021. Accessed September 23, 2023. https://nationalpartnership.org/wp-content/uploads/2023/04/immigrant-moms-and-babies-denied.pdf
Hasstedt K, Rowan A. Understanding intimate partner violence as a sexual and reproductive health and rights issue in the United States. Guttmacher Institute. June 30, 2016. Accessed September 23, 2023. https://www.guttmacher.org/gpr/2016/07/understanding-intimate-partner-violence-sexual-and-reproductive-health-and-rights-issue
Lawn RB, Koenen KC. Homicide is a leading cause of death for pregnant women in US. BMJ. 2022;379:o2499.
Nash E, Guarnieri I. In the US midterm elections, resounding victories for abortion on state ballot measures. Guttmacher Institute. November 9, 2022. Accessed August 20, 2023. https://www.guttmacher.org/2022/11/us-midterm-elections-resounding-victories-abortion-state-ballot-measures
Reproductive rights include bodily autonomy for trans and intersex youth. National Women’s Law Center. August 9, 2022. Accessed September 23, 2023. https://nwlc.org/resource/reproductive-rights-include-bodily-autonomy-for-trans-and-intersex-youth/
Baden K, Driver J. The state abortion policy landscape one year post-Roe. Guttmacher Institute. June 15, 2023. Accessed September 23, 2023. https://www.guttmacher.org/2023/06/state-abortion-policy-landscape-one-year-post-roe
Tu L. One year after Dobbs, abortion bans are harming reproductive care, ob-gyns say. Scientific American. June 23, 2023. Accessed September 23, 2023. https://www.scientificamerican.com/article/one-year-after-dobbs-abortion-bans-are-harming-reproductive-care-ob-gyns-say1/
After Roe fell: abortion laws by state. Center for Reproductive Rights. Accessed September 23, 2023. https://reproductiverights.org/maps/abortion-laws-by-state/
Mace S. Statement in response to Dobbs v Jackson Women’s Health Organization. HELP MLP. June 27, 2022. Accessed September 24, 2023. https://helpmlp.org/2022/06/27/statement-in-response-to-dobbs-v-jackson-womens-health-organization/
Using legal services as part of a community strategy to improve maternal and child health: 2023 learning collaborative. National Center for Medical-Legal Partnership. March 1, 2023. Accessed September 24, 2023. https://medical-legalpartnership.org/mlp-resources/maternal-health-learning-collab-2023/
Legal Services Corporation. By The Numbers: The Data Underlying Legal Aid Programs. Legal Services Corporation; 2022. Accessed September 24, 2023. https://lsc-live.app.box.com/s/e0ejxcp3lp4msvp77mvrzy9w0z354tf7
Regenstein M, Trott J, Williamson A. The state of the medical-legal partnership: field findings from the 2016 National Center for Medical-Legal Partnership surveys. National Center for Medical-Legal Partnership; 2017. Accessed February 4, 2024. https://medical-legalpartnership.org/wp-content/uploads/2017/07/2016-MLP-Survey-Report.pdf
Fast facts about abortion funds. National Network of Abortion Funds. Accessed March 19, 2024. https://abortionfunds.org/abortion-funds-fast-facts/
Richards M. The public, including women of childbearing age, are largely confused about the legality of medication abortion and emergency contraceptives in their states. Kaiser Family Foundation. February 1, 2023. Accessed September 24, 2023. https://www.kff.org/womens-health-policy/press-release/the-public-including-women-of-childbearing-age-are-largely-confused-about-the-legality-of-medication-abortion-and-emergency-contraceptives-in-their-states/
The Legal Services Corporation Act, 42 USC §2996f (b)(8) (2023).
Shetty N. Abortion medication minefield causing pharmacists confusion. Bloomberg Law. June 9, 2023. Accessed August 20, 2023. https://news.bloomberglaw.com/us-law-week/abortion-medication-minefield-causes-confusion-for-pharmacists
Chen A, Robles-Fradet A, Arega H. Building a successful program for Medi-Cal coverage for doula care: findings from a survey of doulas in California. National Health Law Program; 2020. Accessed August 20, 2023. https://healthlaw.org/wp-content/uploads/2020/04/NHeLP-DoulaCare-Web-Format-final.pdf
Rappazzo N, Chen A. Aligning pregnancy-related Medicaid coverage extensions and Medicaid doula coverage to improve maternal health. National Health Law Program. August 3, 2023. Accessed September 24, 2023. https://healthlaw.org/resource/aligning-pregnancy-related-medicaid-coverage-extensions-and-medicaid-doula-coverage-to-improve-maternal-health/
Glicksman E. Stigma’s toll on sexual and reproductive health. Hopkins Bloomberg Public Health. October 17, 2022. Accessed August 20, 2023. https://magazine.jhsph.edu/2022/stigmas-toll-sexual-and-reproductive-health
Mattioli ML, Strandquest JK. Protection of health info post-“Dobbs”: providers and patients are stuck in the middle. Legal Intelligencer. June 30, 2023. Accessed September 24, 2023. https://www.law.com/thelegalintelligencer/2023/06/30/protection-of-health-info-post-dobbs-providers-and-patients-are-stuck-in-the-middle/
Nash E, Ephross P. State policy trends at midyear 2022: with Roe about to be overturned, some states double down on abortion restrictions. Guttmacher Institute. June 22, 2022. Accessed September 24, 2023. https://www.guttmacher.org/article/2022/06/state-policy-trends-midyear-2022-roe-about-be-overturned-some-states-double-down
New KFF national survey of OBGYNs finds Dobbs decision has made it harder to treat miscarriages and other pregnancy-related emergencies in affected states; in states with bans, half report patients who were unable to obtain an abortion they sought. News release. Kaiser Family Foundation; June 21, 2023. Accessed September 24, 2023. https://www.kff.org/womens-health-policy/press-release/kff-national-survey-of-obgyns-finds-dobbs-decision-has-made-it-harder-to-treat-miscarriages-and-other-pregnancy-related-emergencies-in-states-with-bans/



