Medicine and Society
Feb 2024
Peer-Reviewed

One Health—a holistic approach to health that brings the moral status of animals and environments into consideration—is understood as a “professional imperative,” a value-laden obligation that flows from the scope and objectives of professional roles. In this article, antimicrobial resistance provides a case study to demonstrate the fruitfulness of public health and bioethics collaborations by applying One Health key concepts of interconnection and interdependence. Moving toward an ethics of One Health requires a more nuanced analysis of ecological relationships, including humans’ connections to other species as hosts, vectors, domestic companions, meat-eaters’ food, and farmers’ livelihood.
Infectious diseases are a paradigmatic example of the interconnectedness of health behaviors and health outcomes. If you are infected with a virus and do not mask, I am exposed to it. Whether you like it or not, my cough can determine whether you spend the weekend in bed. A One Health approach to health extends relevant interconnections from humans to animals and our environments. One Health is defined as “a collaborative, multisectoral, and transdisciplinary approach—working at the local, regional, national, and global levels—with the goal of achieving optimal health outcomes recognizing the interconnection between people, animals, plants, and their shared environment.”1 It is a useful approach, especially for health problems involving interspecies connections. Antimicrobial resistance in bacterial, viral, and fungal pathogens is a multifactorial challenge that is especially well captured by a One Health model.2 Resistance can be intrinsic, as when cell wall structures create barriers that block antimicrobials from entering the cell. Resistance can also be acquired, since with each exposure to an antimicrobial treatment, microbes with the genetic capacity to withstand (resist) the medicine are more likely to survive. And, unlike human genes that are only shared from generation to generation, bacteria can share genes horizontally, or among members of a colony. These multiple modes of gene transfer enable bacteria to develop the capacity to resist antibiotics very quickly.3
Antimicrobial treatments and resistance are dual public health and moral dilemmas. We need to reduce suffering from infections, but the more we use antimicrobials against pathogens, the more we create the conditions for resistant strains to become dominant, which increases suffering from infections in the future. A One Health model helps us plan and act with greater coordination. It does so by recognizing how microbes and antimicrobial-resistant pathogens can be transmitted across species, thereby directing policy attention to antimicrobial use across human, veterinary, and agricultural sectors simultaneously.4 Applied to problems of antimicrobial resistance, a One Health approach highlights how environmental, animal, and human uses of antimicrobials must be coordinated among many stakeholders and involve complex considerations. Yet the ethical and social aspects of antimicrobial resistance are understudied.5 In this article, antimicrobial resistance provides a case study to demonstrate the fruitfulness of public health and bioethics collaborations by analyzing One Health key concepts of interconnection and interdependence.
John Stuart Mill’s harm principle provides a broad justification for public health policy by distinguishing between self-regarding and other-regarding behavior: “As soon as any part of a person’s conduct affects prejudicially the interests of others, society has jurisdiction over it, and the question whether the general welfare will or will not be promoted by interfering with it, becomes open to discussion.”6 For Mill, other-regarding behavior is a necessary criterion for justifying state restriction of individual liberty in cases of harm prevention. A One Health approach extends Mill’s harm principle beyond nation states and beyond human-only relationships by explicating the far-reaching consequences of human behaviors across borders and species. For instance, a One Health approach is responsive to increasing evidence of the harms of land-use policies that value maximum yields and intensive practices—factors contributing to higher antimicrobial use7,8,9—with the United States being among the leading contributors to antimicrobial use in agriculture.10
A One Health approach to complex causes is also consonant with a variety of environmental ethics traditions. For example, Peter Singer’s championing of animal rights extends the consequentialist tradition by deeply examining the negative ramifications of human meat consumption for animal suffering and environmental sustainability.11 Moreover, Van Rensselaer Potter’s vision of bioethics embraces multidisciplinary research and action, endeavors that “would attempt to generate wisdom, the knowledge of how to use knowledge for social good.”12 Potter’s vision has recently been reinvigorated, partly in response to global health challenges like antimicrobial resistance and climate change.13 Like climate change, antimicrobial resistance heightens the importance of time in our moral and political deliberations. The rise of pathogens that can resist treatment highlights intergenerational justice: what we (fail to) do now to conserve antimicrobial effectiveness determines the infectious disease burden borne by those in the future.14
As with other-regarding behavior, One Health often draws a straight line between interconnectedness and the moral obligations that arise from it. For example, in the Centers for Disease Control and Prevention One Health social media graphics, interconnectedness immediately translates to a promissory rhetoric of collective health action and protection: “One Health is the idea that the health of people is connected to the health of animals and our shared environment…. When we protect one, we help protect all.”15 Implicit appeals like these are a starting point for developing a more explicit One Health ethics.
However, as Jonathan Beever and Nicolae Morar note, interconnectedness is conceptually proximal to, but distinct from, interdependence, although the two are often conflated.16 Interconnectedness may entail simple causal dependence, such that one factor determines the other: use of antibiotics for infections leads to patient satisfaction when symptoms resolve. In ascertaining causation, researchers typically seek to control one factor—such as antibiotic prescribing—to determine its influence on a dependent variable, such as patient demand. In antimicrobial resistance, the causal interconnections involved are so complex they have even been dubbed “super-wicked.”17 For conceptual clarity, it is worth distinguishing 3 forms of interconnectedness when thinking about antimicrobial resistance. I will refer to these as epistemic, practical, and collective interconnectedness.
In contrast to interconnectedness, interdependence captures the normative aspect of forms of connection in which individual or group benefit turns on the behavior of another party.16 There are many forms of interdependence, from deep need to receive and give (such as with an infant and parent) to transactional reliance (including contracts or market exchanges). Interdependence can be among our most valued connections, such as when love generates abiding and multidirectional sharing of vulnerability and advantage (mutuality). But interdependence can also be negative, such as in relationships of oppression, wherein those in power rely on systems of subjugation to extract goods and labor from others and in which the well-being of those who are subjugated rests on the restraint and mollification of those in power.
Confusion between interconnection and interdependence leads to a wide range of views about the role of ethics in a One Health approach. Some contend that One Health interdependence is meant to be a primarily descriptive term, carrying little or no normative weight.18 In contrast, Henrik Lerner and Charlotte Berg have argued that a One Health approach inevitably bears normative implications—first, because it involves delineating which disciplines are included in its collaborative vision and, second, because the approach requires defending a distinctive definition of health for policy makers.19 Splitting the difference, interconnection and interdependence strike me as highly related features of infectious diseases that challenge the fact-value distinction. They may be conceptually distinct, but they are practically entangled. That my health is causally connected to yours inevitably invites questions about how we take our shared or opposing interests into account.
A One Health approach needs a corollary account of how obligations flow from values as well as causal relationships. This approach is implicit in the understanding of One Health as a “professional imperative.”20 A professional imperative refers to a value-laden obligation that flows from the scope and objectives of professional roles. We need not start from scratch in seeking such an account. Because Mill was primarily concerned with delimiting state intervention in private life, a Millian ethos might start by delineating principles for imposing liberty-restricting measures. For example, although the public health harm of antimicrobial-resistant pathogens might be considered a justification for public monitoring of the quantity of antimicrobial prescriptions written by each clinician, challenges to clinicians’ “right” to prescribe have sometimes been framed as an infringement on the clinical autonomy of practitioners.21 However, public health also concerns ascription of responsibility based on consequences that follow from acts of omission as well as acts of commission. Within One Health, the imperative is to recognize that interdependence can be good—involving mutual benefit—and not merely an infringement of individual autonomy. As a result, bioethics and One Health collaborations might also consider the rationale for formation of policy grounded in intergenerational harm prevention, given the morbidity and mortality that will befall future populations if antimicrobial resistance is not effectively mitigated.
We also need ethical and political analyses of situations in which individual and collective freedoms or rights conflict in the context of antimicrobial resistance. Such analyses are needed as a corrective to Western European cultural biases, which can overly emphasize individualism, and could encompass a range of other-regarding relationships—ranging from domination, exploitation, and complicity to dependence, trust, and care.21,22,23,24,25,26 In the end, a One Health ethics will need a holistic ethos of individual and collective action. As Onora O’Neill has articulated, bioethical conceptualizations of autonomy sometimes render other forms of reliance—such as trust—undesirable.27 In other words, if we depict the best relationship to health as independence from others so we can each choose, are we doing unintentional damage by suggesting that all forms of dependence are undesirable? A One Health ethics would advance efforts to enact health policies that recognize the connections, conceptually and practically, between individual and community, freedom and public benefit.
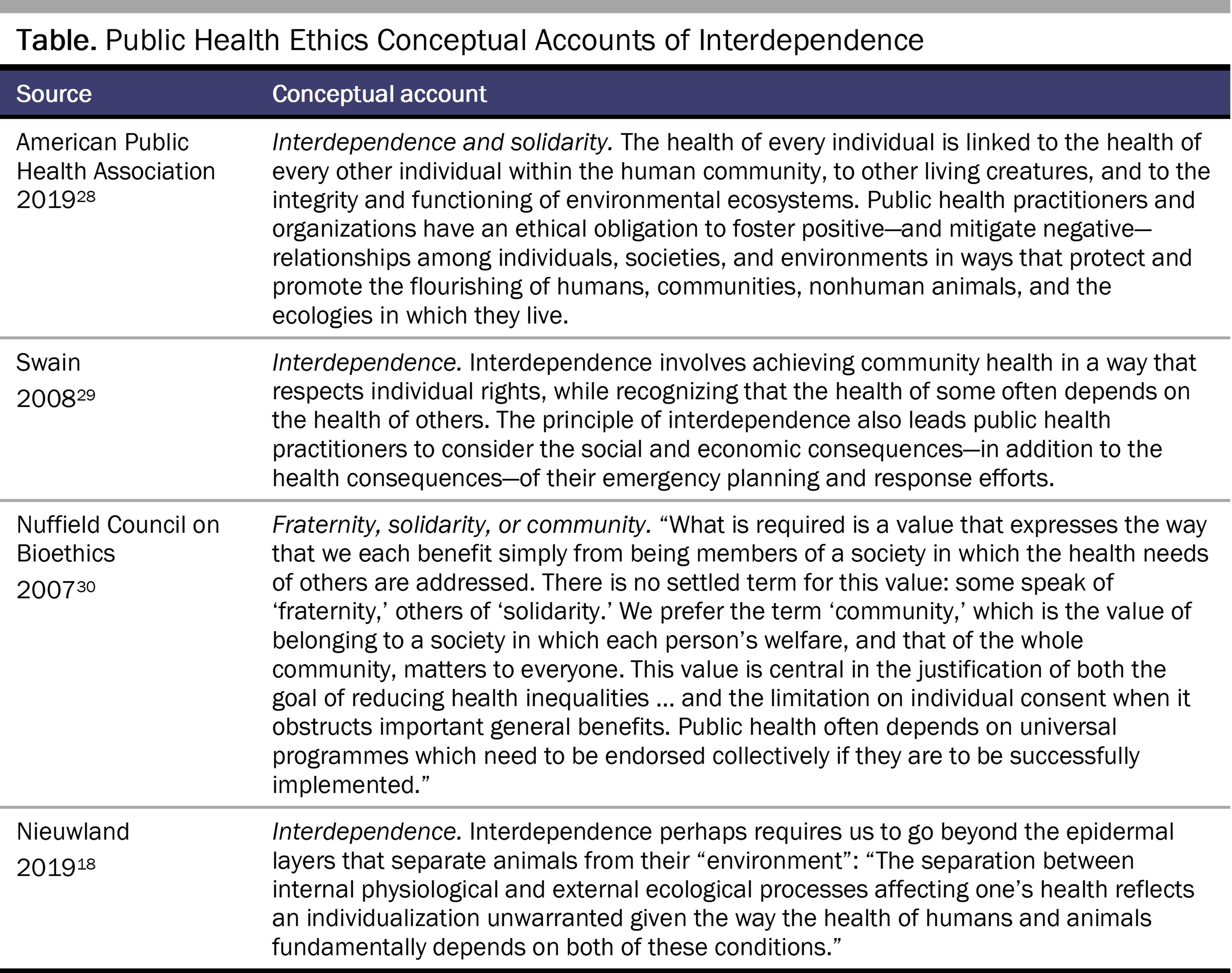
Conceptual clarity and practical action are especially relevant to a One Health approach, wherein interdependence plays a central role. As with interconnection, accounts of interdependence in public health ethics are widely varied (See Table).
Explicating an ethics of interdependence is a key task for advancing ethics and One Health policy. Collective interconnection, such as the shared impacts of widespread antimicrobial resistance, raises questions about interdependence—how we distribute or share responsibility when we rely on each other to coordinate action because of our shared fate. Take the example of a farmer on the East Coast whose use of antimicrobials to increase the growth rate of his turkey flock possibly (highly contingently) increases the chance of a 21-year-old in the Southwest dying from an antimicrobial-resistant infection. The contingencies make it difficult to attribute antimicrobial resistance to a single or significant casual factor. In parallel, any related responsibilities are also challenging to justify and assign. Analysis of collective responsibility for antimicrobial resistance on the population or systems level would provide stronger causal evidence—and perhaps stronger normative grounds—for policy change. It is known that the greater the demand for meat, the greater the use of antimicrobials for growth promotion, and the higher the chances of generating antimicrobial resistance in human populations.31 A One Health ethics cries out for greater clarity on how different forms of connection and dependence might generate distinct responsibilities. For example, are national obligations to mitigate antimicrobial resistance distinct? That is, what do affluent nations owe low- and middle-income countries when the affluent have more resources to dedicate to mitigating the development of antimicrobial resistance? As an ethics of interdependence is developed, its relevance for population health challenges other than antimicrobial resistance—such as chronic diseases that also require policy coordination—can also be examined.32
A One Health approach sets the broadest backdrop for exploring social and ethical questions that arise in relation to antimicrobial-resistant infections. A shared appreciation for pragmatic, interprofessional problem solving in bioethics and One Health provides a shared starting point for future collaborations. For social scientists, a research goal might be to critically analyze how antimicrobial resistance results from interdependence and how interdependent relationships are made possible or discouraged by social systems. For ethicists, analysis of interdependence often involves value-based assessments of whether such interdependencies are good or desirable, generate obligations, or violate rights of parties. Public health practitioners with environmental, agricultural, and health policy expertise also have key contributions to make in future collaborations. Beyond the One Health level of analysis, antimicrobial resistance calls for similar efforts to advance multidisciplinary team science. Other pertinent levels of analysis range from patient-clinician relationships to meso-level contexts much narrower than the One Health framing (see Figure).
Figure. Levels of Analysis for Advancing Research on Ethical and Social Aspects of Antimicrobial Resistance
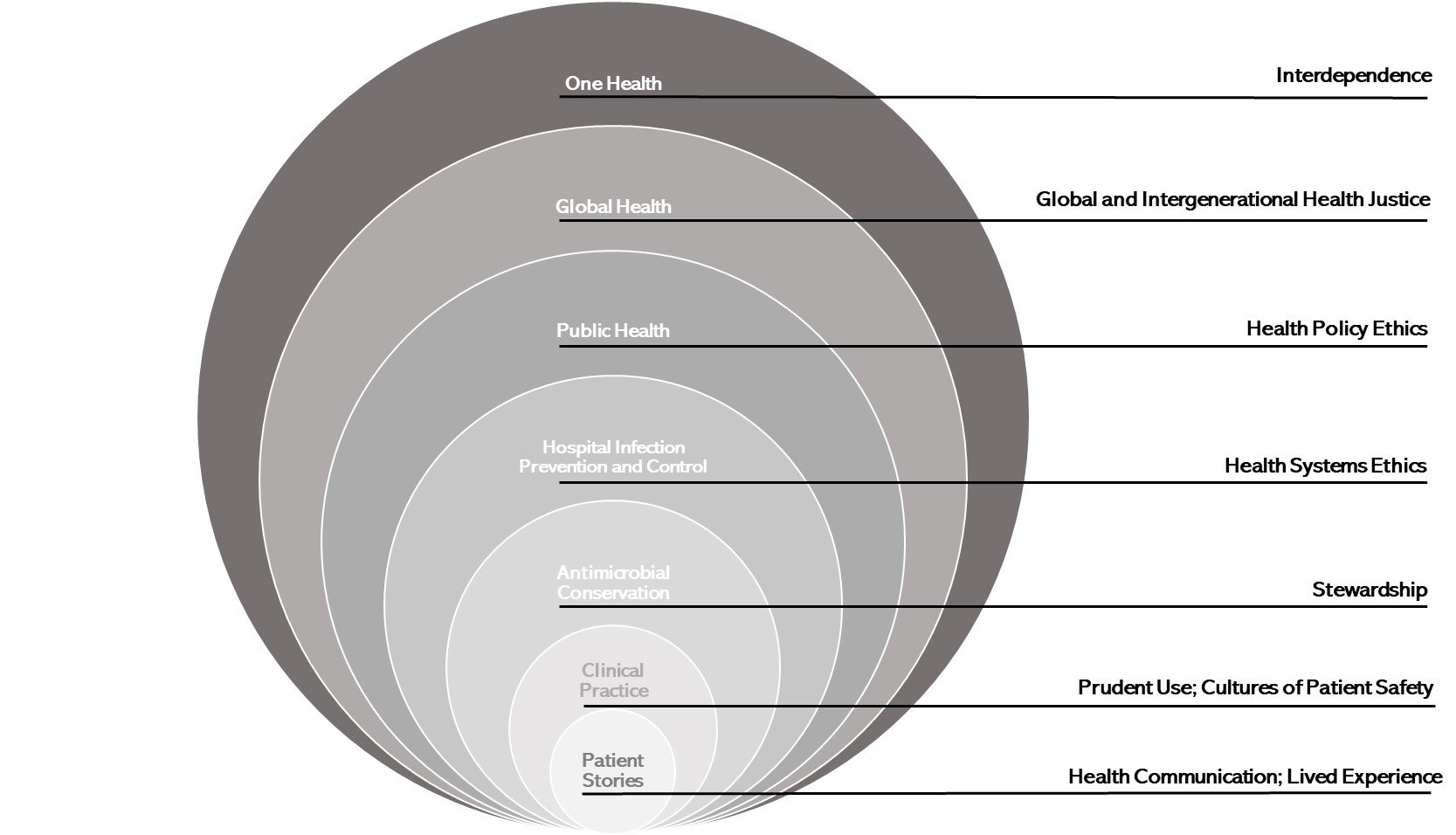
The complexity of antimicrobial resistance lends itself to multiple framings.33,34 Rather than viewing frames as competing approaches, multidisciplinary teams might employ different frames to focus on an element of antimicrobial resistance. A One Health backdrop serves as a reminder to avoid oversimplification by keeping interconnection and interdependence front and center as new solutions are envisioned, designed, and implemented.
One Health. Centers for Disease Control and Prevention. Reviewed May 24, 2023. Accessed March 29, 2023. https://www.cdc.gov/onehealth/index.html
Jorge P, Magalhães AP, Grainha T, et al. Antimicrobial resistance three ways: healthcare crisis, major concepts and the relevance of biofilms. FEMS Microbiol Ecol. 2019;95(8):fiz115.
One Health Initiative. World Health Organization. Accessed March 28, 2023. https://www.who.int/teams/one-health-initiative/quadripartite-secretariat-for-one-health
Frid-Nielsen SS, Rubin O, Baekkeskov E. The state of social science research on antimicrobial resistance. Soc Sci Med. 2019;242:112596.
Mill JS. On Liberty. Rapaport E, ed. Hackett Publishing; 1978.
Binot A, Duboz R, Promburom P, et al. A framework to promote collective action within the One Health community of practice: using participatory modelling to enable interdisciplinary, cross-sectoral and multi-level integration. One Health. 2015;1:44-48.
Mulchandani R, Wang Y, Gilbert M, Van Boeckel TP. Global trends in antimicrobial use in food-producing animals: 2020 to 2030. PLOS Glob Public Health. 2023;3(2):e0001305.
Singer P. Animal Liberation: Towards an End to Man’s Inhumanity to Animals. Granada Publishing; 1990.
Potter VR. Bioethics: Bridge to the Future. Prentice-Hall; 1971.
What is One Health? Centers for Disease Control and Prevention. Accessed June 28, 2023. https://www.cdc.gov/onehealth/images/social-media/what-is-one-health-fb.jpg
Littmann J, Viens AM, Silva DS. The super-wicked problem of antimicrobial resistance. In: Jamrozik E, Selgelid M, eds. Ethics and Drug Resistance: Collective Responsibility for Global Public Health. Springer Cham; 2020:421-443.
Nieuwland J, Meijboom FLB. One Health: how interdependence enriches veterinary ethics education. Animals (Basel). 2019;10(1):13.
Lerner H, Berg C. The concept of health in One Health and some practical implications for research and education: what is One Health? Infect Ecol Epidemiol. 2015;5:25300.
One Health Initiative Task Force. One Health: a new professional imperative. American Veterinary Medical Association; 2008. Accessed March 28, 2023. https://www.avma.org/KB/Resources/Reports/Documents/onehealth_final.pdf
Longino HE. Subjects, power, and knowledge: description and prescription in feminist philosophies of science. In: Alcoff L, ed. Feminist Epistemologies. Routledge; 2013:101-120.
Kutz C. Complicity: Ethics and Law for a Collective Age. Cambridge University Press; 2000.
MacIntyre AC. Dependent Rational Animals: Why Human Beings Need the Virtues. Open Court Publishing; 1999.
Giubilini A, Savulescu J. Moral responsibility and the justification of policies to preserve antimicrobial effectiveness. In: Jamrozik E, Selgelid M, eds. Ethics and Drug Resistance: Collective Responsibility for Global Public Health. Springer; 2020:141-154.
O’Neill O. Autonomy and Trust in Bioethics. Cambridge University Press; 2002.
American Public Health Association. Public health code of ethics. American Public Health Association; 2019 Accessed June 5, 2023. https://www.apha.org/-/media/files/pdf/membergroups/ethics/code_of_ethics.ashx
Nuffield Council on Bioethics. Public Health: Ethical Issues. Nuffield Council on Bioethics; 2007. Accessed June 5, 2023. https://www.nuffieldbioethics.org/assets/pdfs/Public-health-ethical-issues.pdf
Avraam C, Lambrou AS, Jiang W, Siddiqui S. Antimicrobial resistance and livestock trade for low and middle income countries: regional analysis of global coordination policies. Front Sustain Food Syst. 2021;5:650315.
Destoumieux-Garzón D, Mavingui P, Boetsch G, et al. The One Health concept: 10 years old and a long road ahead. Front Vet Sci. 2018;5:14.
Meagher KM, Watson S, Suh GA, Virk A. The new precision stewards? J Pers Med. 2022;12(8):1308.




{kind=link}