State of the Art and Science
Mar 2006
Acute appendicitis is responsible for more than 250 000 visits to the emergency room every year, with a roughly 7 percent probability of occurrence over one's lifetime [1]. Although appendicitis is usually diagnosed on the basis of clinical findings, computed tomography (CT) and other imaging modalities have been used when the diagnosis is unclear. The escalating use of CT has led physicians to examine its diagnostic role more closely.
Based on the risk-benefit ratio of the surgery, physicians generally accept that about 15 percent of appendectomies will reveal a normal appendix, although this rate varies with the population being considered [2]. In a healthy young man with right lower quadrant pain, this "negative appendectomy" rate is less than 10 percent, whereas it may reach 20 percent in a young woman due to other pelvic processes that obscure the diagnosis and alter the risk-benefit ratio. Young children and patients over the age of 65 historically have higher rates of both perforated appendix and negative appendectomy [3].
As many as 45 percent of patients do not display classic signs of acute appendicitis, making imaging a potentially useful tool. For example, approximately one third of patients have normal white blood cell counts, and some patients are afebrile until perforation [4]. In situations such as these, CT can aid in the diagnosis.
Physicians are increasingly ordering CT scans to balance the risk of a negative appendectomy with the risk of delayed surgery and a perforated appendix. A large, population-based trial published in the Journal of the American Medical Association in 2001, however, demonstrated that the accuracy of diagnosing appendicitis has not improved with the use of advanced imaging techniques over the last 15 years [5]. In general, the researchers recommended imaging only when the diagnosis is unclear, and for these cases CT is usually the preferred method of imaging. The same group published a longitudinal study in the Journal of the American College of Surgeons in December 2005 confirming the unchanged rate of negative appendectomy despite increasing use of CT and ultrasound [6].
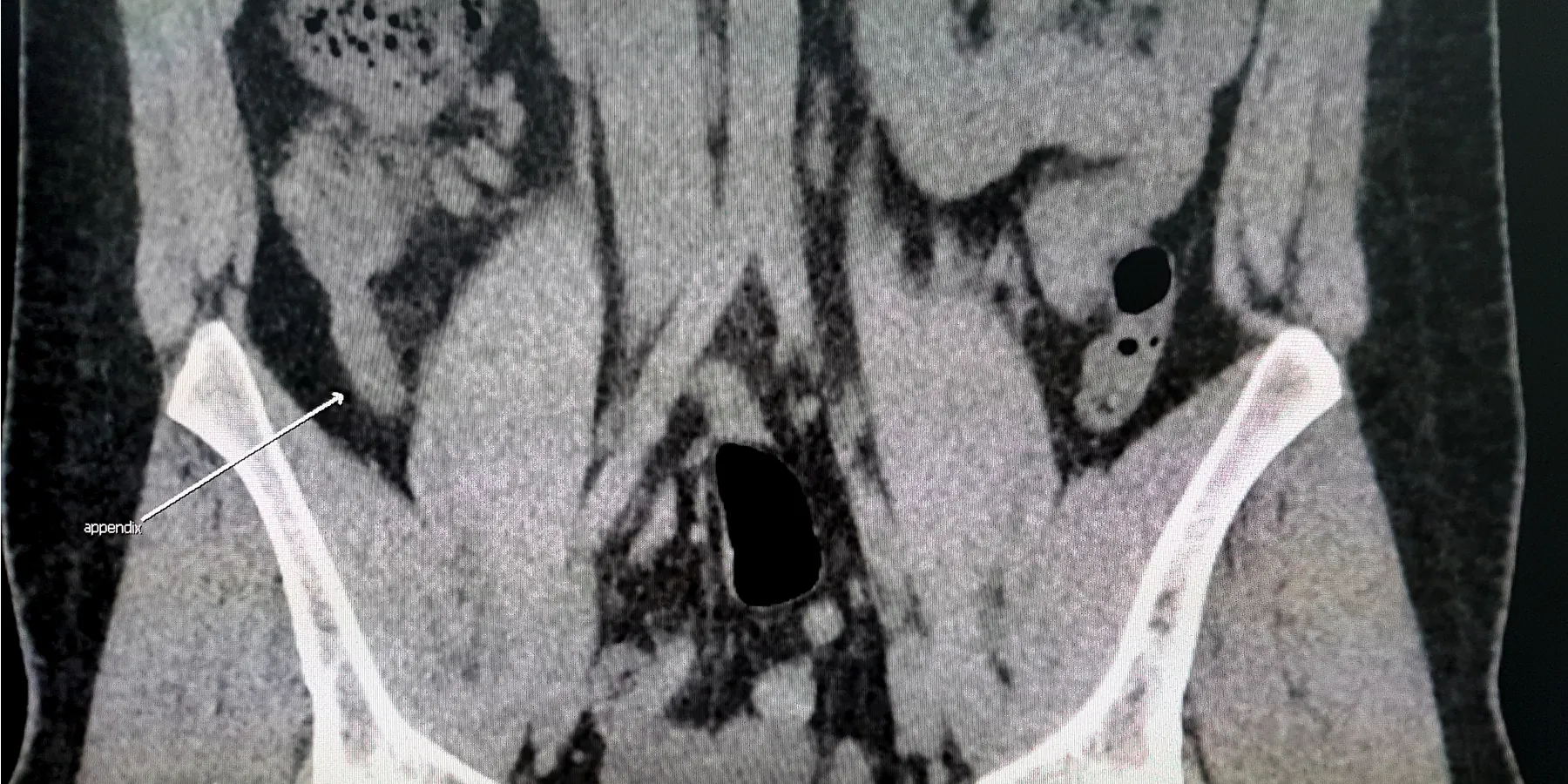
When using CT to diagnose appendicitis, there are 2 main options: the standard abdominal and pelvic scan and the appendiceal scan with rectal contrast. The former displays classic patterns such as concentric, thickened appendiceal walls; an appendicolith, fat stranding, or other signs of inflammation. A phlegmon, abscess, or free air can also be suggestive of appendicitis. Contrast or air present within the lumen of the appendix virtually excludes the diagnosis of appendicitis. Based on a systematic review of patients with suspected appendicitis, the sensitivity and specificity of a pelvic and abdominal CT scan are 94 percent and 95 percent, respectively [7]. The benefit of a complete abdominal scan is that alternative diagnoses are made in up to 15 percent of patients [8].
The other option is an appendiceal CT scan with rectal contrast. Introduced in 1996, these are helical, thin-collimation images focused on the right lower quadrant of the abdomen. Contrast is supplied rectally to enable full visualization of the lumen of the bowel. A major benefit of this type of imaging is the rapidity with which results can be obtained—less than 15 minutes. But this method looks only at the appendix, so the scan, if it is normal, will not help in the diagnosis of other pelvic diseases. Thus, the physician should have a high clinical suspicion of appendicitis before choosing this imaging method. Appendiceal CT scans are considered to be 98 percent accurate in diagnosing acute appendicitis when read by an experienced radiologist [9].
Other methods of imaging, such as nuclear scans, use a radiolabeled mononuclear antibody directed against neutrophils. They appear to have a limited role in assisting the diagnosis of appendicitis, mainly due to time required for the scan and limited around-the-clock availability [10].
Before a CT is even considered, history, physical exam, and simple laboratory tests should point to appendicitis as the most likely diagnosis. One should keep in mind that, because nausea and emesis typically occur after the onset of abdominal pain, anorexia is nearly always present in acute appendicitis. Classic physical exam signs include Rovsing's sign and tenderness at McBurney's point. A urinalysis should be ordered to rule out a urinary tract infection (although up to 30 percent of patients with appendicitis also have microscopic hematuria and pyuria due to local irritation of the bladder and ureters), as well as pelvic cultures and a pregnancy test for female patients.
Liu CD, McFadden DW: Acute abdomen and appendix. In: Greenfield LJ, Mulholland MW, Oldham KT, Zelenock GB, Lillemoe KD, eds. Surgery: Scientific Principles and Practice. 2nd ed. Baltimore, Md: Williams & Wilkins; 1997:1246-1261.
Schuler JG, Shortsleeve MJ, Goldenson RS, Prex-Rossello JM, Perlmutter RA, Thorsen A. Is there a role for abdominal computed tomographic scans in appendicitis? Arch Surg. 1998;133(4):373-376.



