Joseph D. Harrison, MBDS and Mitesh S. Patel, MD, MBA
AMA J Ethics. 2020;22(9):E796-801. doi:
10.1001/amajethics.2020.796.
Abstract
Nudges are subtle changes to the design of the environment or the framing of information that can influence our behaviors. There is significant potential to use nudges in health care to improve patient outcomes and transform health care delivery. However, these interventions must be tested and implemented using a systematic approach. In this article, we describe several ways to design nudges for success by focusing on optimizing and fitting them into the clinical workflow, engaging the right stakeholders, and rapid experimentation.
The Potential of Using Nudges in Health Care
Nudges are subtle changes to choice architecture or the framing of information that can significantly influence behavior without restricting choice.1 In health care settings, nudges can be used to improve patient outcomes and health care delivery.2 There is a significant opportunity to expand the use of nudges in health care settings through intentional design, rigorous experimentation, and systematic evaluation. The Penn Medicine Nudge Unit is the world’s first behavioral design team embedded within the operations of a health care system.3 Examples of prior work by our group and others include using default options to increase generic prescribing and reduce opioid prescribing, using active choice to increase influenza vaccination, and using peer comparison feedback to increase statin prescribing and reduce unnecessary antibiotic prescribing.4,5,6,7,8,9,10 These nudges leveraged the electronic health record (EHR) to deploy scalable interventions throughout health systems. In this article, we will describe key factors that drive successful design and implementation of nudges in health care.
Choosing the Right Nudge
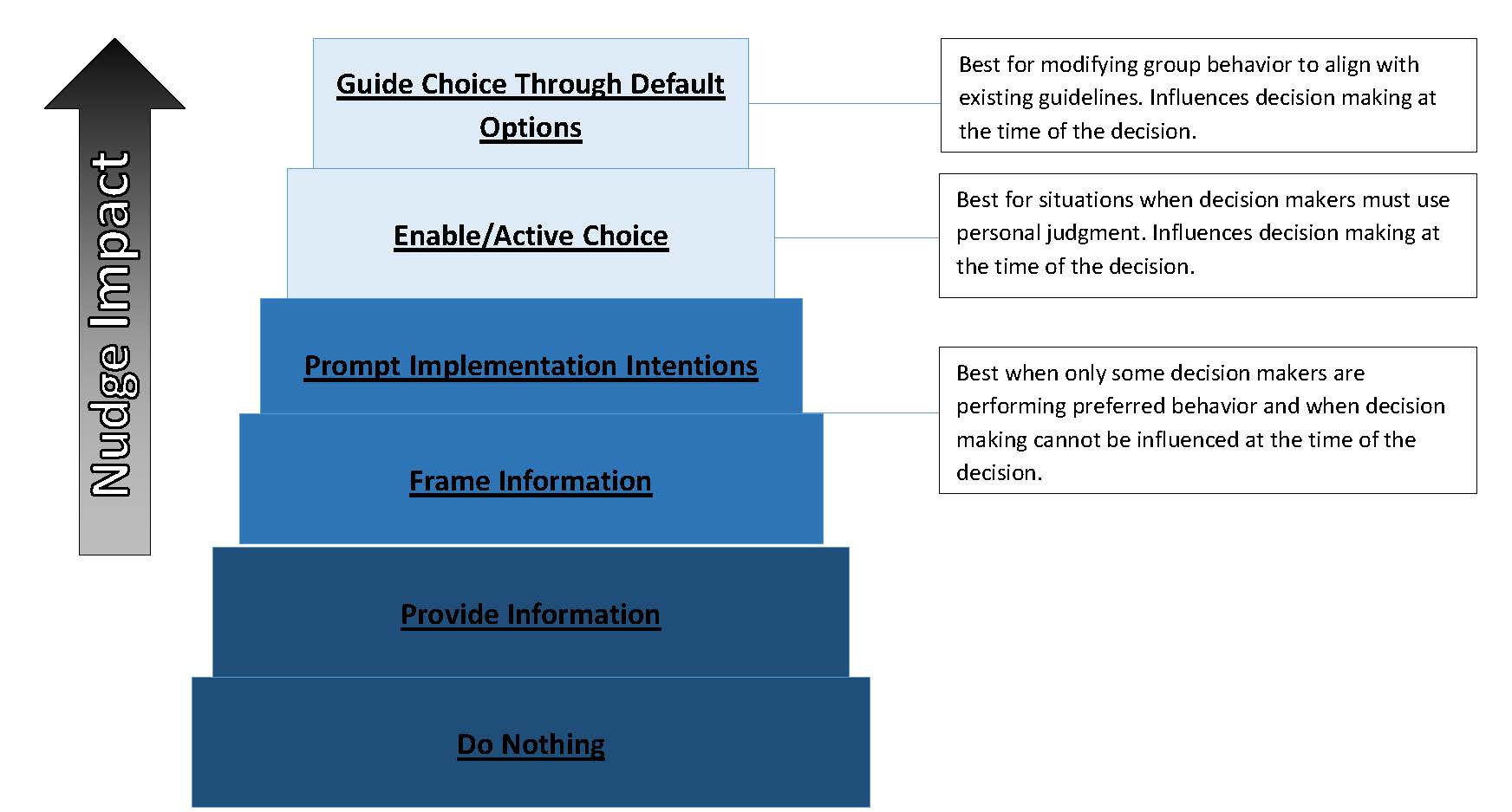
Nudges vary in their approach as well as in their effectiveness. The Figure depicts a nudge intervention ladder that can be used by health systems to help guide the development and implementation of nudges in clinical settings.
Figure. Ladder of Nudge Interventions With Best Practices Recommendationsa
a Adapted with permission from Nuffield Council on Bioethics.11 Nudges can produce various degrees of behavioral impact, with information framing exerting lighter influence and guiding choices through defaults exerting stronger influence.
Nudges towards the bottom of the ladder focus on delivering information. These approaches can be used to deliver infrequent messaging that can influence everyday decisions. For example, in a randomized trial testing the use of an automated dashboard, statin prescribing was significantly greater when a single peer comparison message was sent via email at the beginning of the 2-month intervention (with 2 reminders) to inform clinicians of how their performance compared with that of other physicians at their health system.9
Nudges in the middle of the intervention ladder depend on framing existing information or on prompting goal-directed implementation intentions that specify when, where, or how goal-directed behavior will be enacted.12 Behavioral tools such as precommitment devices can be used to prompt implementation intentions and have been deployed in the past to reduce inappropriate antibiotic prescribing practices.13 For example, in a randomized clinical trial of 5 primary care practices, posting a commitment letter in patient examination rooms for 12 weeks resulted in an absolute decrease in inappropriate antibiotic prescribing of 19.7% relative to the control group, for which no commitment letters were posted.13 In an additional example, leadership across 7 practice sites in the University of Pennsylvania Health System sought to increase high-value prescribing—specifically, of zoledronate over denosumab, which have annual costs of $215 vs $26 000, respectively.14 The retrospective analysis compared increases in the probability of zoledronate prescription of 2 nudge groups—one in which clinical leadership endorsed zoledronate and clinicians received quarterly performance feedback at meetings and via email and another that also included a requirement to justify denosumab prescriptions to pharmacy—to a control group that delivered care as usual.14 Reframing from leadership and performance feedback was associated with a 26% increase in the probability of zoledronate prescription compared with the control, while accountable justification to pharmacy was associated with a 44.9% increase compared with the control.14
Nudges are more likely to be successful when they fit well into the workflow of key decision makers.
As one moves up the ladder, nudges are delivered more directly at the time of decision making either by enabling active choice or setting the evidence-based option as the default selection. While nudges higher on the ladder are often more aggressive, if designed well, they are also often more effective than nudges lower on the ladder. Furthermore, nudges higher on the ladder may best address suboptimal EHR design, which may account for potential decision errors that lead to the overprescription of brand-name drugs when more cost-effective, medically equivalent generics are available.4,15 Recognizing the opportunity to broadly shift clinician behavior to accord existing guidelines, one health system changed the default to set generic prescribing as the opt-out preference, which led to an increase in generic prescription rates from 75.3% to 98.4%.4 Changing defaults is a good approach when clinicians and patients have weakly held preferences for the options and guidelines clearly indicate that the default option is evidence based.
Embedding Nudges Into Clinical Workflow
Nudges are more likely to be successful when they fit well into the workflow of key decision makers. Moreover, there is often an opportunity to shift work away from busy clinicians and onto other members of the team. For example, in one study, an active choice alert in the EHR was implemented to remind clinicians to address influenza vaccination during patient visits to primary care clinics.7 Relative to control practices that did not receive the reminder, the intervention practice had an adjusted increase of 6.6% in influenza vaccination. However, there is evidence that too many EHR-based reminders can cause alert fatigue. Therefore, in a subsequent study, the alert was redirected to medical assistants who could template orders for primary care clinicians to review by asking patients during the check-in process if they were interested in receiving an influenza vaccination, thereby reducing alert burden for clinicians.8 Relative to control practices, this intervention led to an adjusted increase of 9.5% in influenza vaccination, which represents a larger magnitude increase than in the previous study while the intervention more easily fit into clinician workflow. Another study used technology enabled by the EHR to increase low rates of cardiac rehabilitation referral by relieving busy cardiologists of the burden of identifying these patients. Using existing technology platforms, including the EHR, to automatically identify eligible patients and template referral forms increased referral rates from 15% before the intervention to 85% after it was implemented.16
Stakeholder Engagement and Alignment With Health System Operations
Designing nudges for successful implementation requires careful attention to and engagement with relevant stakeholders, including personnel responsible for information systems, frontline clinicians, and health system leadership. It is often challenging to navigate the complex social and political environment that influences health system operations and various stakeholder relationships. Individuals interested in designing nudges should consider reaching out to stakeholders within their own institutions to understand their perspectives and align project indicators with stakeholder indicators for success. In a randomized trial conducted with radiation oncologists, the goal was to reduce unnecessary imaging for palliative cancer patients and change physician practices to be more in line with national guidelines.15 The second author (M.S.P.) and colleagues did several things to engage the appropriate stakeholders. First, the department leadership named this project as one of its quality improvement initiatives of the year. This announcement communicated both the project’s importance and leadership buy-in to members of the department. Second, the study team met with all members of the radiation oncology faculty to go over the guidelines and provide them with feedback on their performance. Third, the intervention—setting the default imaging frequency to be in line with guidelines—was made transparent and communicated throughout the department. Fourth, the study authors obtained feedback from clinicians after the intervention was implemented to identify ways to further improve the design. As a result of this stakeholder co-design process, the introduction of a default imaging order in the EHR that specified no imaging for patients undergoing palliative radiotherapy resulted in an adjusted reduction of 18.6% in daily imaging in a network of 5 radiation oncology practices.17
There are also ways to engage stakeholders more broadly. Each year, the Penn Medicine Nudge Unit holds a crowdsourcing tournament to identify new opportunities for interventions. During this process, anyone from the health system can submit an idea. Through subsequent rounds of review by the Nudge Unit, the ideas are narrowed down to the top submissions and then the selected teams, comprising health system clinicians and staff, pitch their ideas to health system leadership. This approach engages a broad community within our health system and helps to align the goals of leadership, clinicians, and staff.
Rapid Experimentation and Implementation Timing
Each day, health systems around the country are making changes to the design of EHRs that are meant to influence clinician behavior. These processes are often fluid and dynamic, which allow for frequent changes based on feedback. However, in most cases, EHR changes are deployed without first experimentally comparing the intervention with a control and evaluating it for longer-term periods or for unintended consequences. Randomized trials could be used more systematically to improve the design of these interventions.18 This more rigorous approach could provide faster feedback for transferring changes that work in one setting to other settings throughout the health system, while curtailing changes that may reduce cognitive burden but do not improve patient care. In a randomized trial focused on increasing primary care physicians’ statin prescribing rates, M.S.P. and colleagues conducted a 2-month study to test ways to engage physicians with automated patient dashboards.9 We found that a one-time message comparing the physicians’ performance to peer clinicians significantly increased engagement. This rapid experiment allowed us to incorporate these elements in the design of larger interventions throughout the entire primary care network.
Conclusion
There is a significant opportunity to improve the delivery of health care by allocating more strategic attention to the implementation of nudges to guide clinician decisions and patient behavior. To improve success, it is important to consider the optimal nudge design, embed interventions within clinical workflow (such as through the EHR), engage a wide range of stakeholders, and implement interventions through carefully designed experimentation.
Patel MS, Day SC, Halpern SD, et al.
Generic medication prescription rates after health system-wide redesign of default options within the electronic health record.JAMA Intern Med.
2016;176(6):847-848.
Olshan D, Rareshide CAL, Patel MS.
Longer-term durability of using default options in the electronic health record to increase generic prescribing rates.J Gen Intern Med.
2019;34(3):349-350.
Delgado MK, Shofer FS, Patel MS, et al.
Association between electronic medical record implementation of default opioid prescription quantities and prescribing behavior in two emergency departments.J Gen Intern Med.
2018;33(4):409-411.
Patel MS, Volpp KG, Small DS, et al.
Using active choice within the electronic health record to increase influenza vaccination rates.J Gen Intern Med.
2017;32(7):790-795.
Kim RH, Day SC, Small DS, Snider CK, Rareshide CAL, Patel MS. Variations in influenza vaccination by clinic appointment time and an active choice intervention in the electronic health record to increase influenza vaccination. JAMA Netw Open. 2018;1(5):e181770.
Patel MS, Kurtzman GW, Kannan S, et al. Effect of an automated patient dashboard using active choice and peer comparison performance feedback to physicians on statin prescribing: the PRESCRIBE Cluster Randomized Clinical Trial. JAMA Netw Open. 2018;1(3):e180818.
Meeker D, Linder JA, Fox CR, et al.
Effect of behavioral interventions on inappropriate antibiotic prescribing among primary care practices: a randomized clinical trial.JAMA.
2016;315(6):562-570.
Robinson SA, Bisson AN, Hughes ML, Ebert J, Lachman ME.
Time for change: using implementation intentions to promote physical activity in a randomised pilot trial.Psychol Health.
2019;34(2):232-254.
Takvorian SU, Ladage VP, Wileyto EP, et al.
Association of behavioral nudges with high-value evidence-based prescribing in oncology.JAMA Oncol.
2020;6(7):1104-1106.
Vaughn VM, Linder JA.
Thoughtless design of the electronic health record drives overuse, but purposeful design can nudge improved patient care.BMJ Qual Saf.
2018;27(8):583-586.
Sharma S, Guttmann D, Small DS, et al.
Effect of introducing a default order in the electronic medical record on unnecessary daily imaging during palliative radiotherapy for adults with cancer: a stepped-wedge cluster randomized clinical trial.JAMA Oncol.
2019;5(8):1220-1222.