Medicine and Society
Feb 2023
Peer-Reviewed
Victims of child abuse and neglect come from every racial, ethnic, and socioeconomic background, yet clinical evaluation, reporting to child protective services, and responses to reports inequitably harm Black children and malign families of color. Racial bias and inequity in suspicion, reporting, and substantiation of abuse and neglect and in services offered and delivered, foster care placement, and criminal prosecution are widely documented. In response, clinicians and health care organizations should promote equity by educating clinicians about racial bias, standardizing evaluation using clinical decision support tools, and working with policy makers to support prevention services. If we decide that it is ethically justifiable for clinicians to err on the side of overreporting, we must ensure fair distribution of associated benefits and harms among all children and families.
The term vulnerable is often used to refer to a population at risk of being harmed and worthy of society’s protection.1 Children are inherently vulnerable due to their dependency on others to survive and flourish.2 This dependency puts them at risk of maltreatment, which includes neglect, abuse, and exploitation. States’ mandated reporter laws, which require clinicians to report suspected abuse and neglect to child protective services (CPS), were created as a way to protect children from such harm. Kim et al estimate that over one-third (37%) of all US children experience a CPS investigation by 18 years of age; the rates are higher for African American children (53%) and lower for Asians/Pacific Islanders (10%).3 While the benefit of protecting a child from abuse and neglect is clear, the harms of over- vs underreporting must also be considered, particularly when certain harms are experienced disproportionately among children from certain racial and ethnic groups.
Unwarranted reports—one consequence of overreporting—not only threaten the therapeutic relationship between the patient or family and clinician but also can result in significant emotional and financial hardships for children and families, including traumatic separation, stigmatization due to CPS involvement, missed workdays, and legal costs associated with the investigation.4,5 Such reports also increase the workload of already overburdened child welfare workers, creating a barrier to identifying and addressing true cases of abuse and neglect or arranging support services for families.5,6,7 Even if a report is unwarranted, children are at risk of both removal from their families and longer-term harms of foster care due to the bias that exists at every step of the child welfare decision-making process. Racial and ethnic differences have been identified in acceptance rates of reports for investigative response, substantiation of maltreatment, referral to services, and out-of-home placement.8,9,10,11 If we decide that these known harms of overreporting are ethically justifiable due to the benefit of protecting children from further maltreatment, we must ensure that the benefits and harms are fairly distributed among all children and families.
Currently, clinicians are taught to report when they have reason to suspect that abuse or neglect has occurred. Yet, of 3.9 million referrals to CPS involving 7 million children, only 618 000 (15.8%) children were substantiated as victims of abuse or neglect in 2020.12 While CPS findings do not identify all victims, and while many families receive services without a formal finding, there is nonetheless a notable margin of error in rates of reporting and substantiation of maltreatment. In particular, national child welfare data show higher rates of abuse and neglect reporting and substantiation among underrepresented minority families, leading some to conclude that minority children are more likely to be abused or neglected than White children.12 However, research that includes children with suspected abuse and neglect who are not reported to CPS has shown either that there are no differences in rates of abuse and neglect by race or ethnicity or that the differences depend on socioeconomic status.13,14 These data indicate that a clinician’s decision to evaluate and report suspected abuse and neglect is influenced by factors other than the actual presence of abuse or neglect. Implicit bias and racism have been postulated to explain these differences, although evidence from multiple research studies examining racial or ethnic disparities in evaluation and reporting of child abuse and neglect is not entirely consistent (see Table).9,10,15,16,17,18,19,20
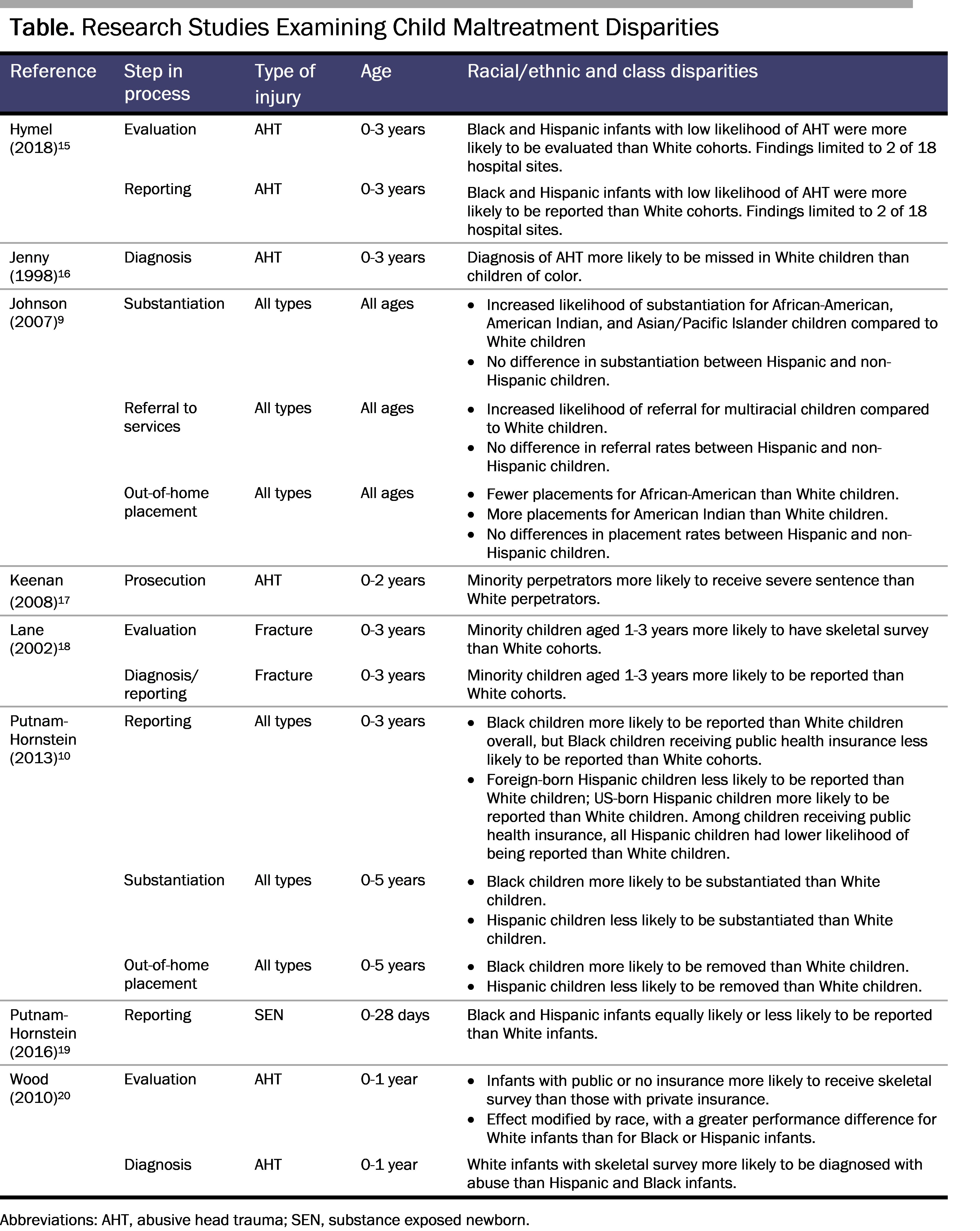
Child abuse and neglect identification bias can occur when minority children are overidentified—or when White children are underidentified—as victims. One of the first to describe this bias in the medical literature was Jenny et al, who found that the diagnosis of abusive head trauma (AHT) was more likely to be missed in White children than in Black children.16 Relatedly, Lane et al found that minority children aged 1 to 3 years were nearly 9 times as likely to be evaluated for abuse with a skeletal survey than White children after adjusting for insurance status, likelihood of abuse, and appropriate ordering of skeletal survey and that minority children at least 12 months old with accidental injuries were more than 3 times as likely to be reported to CPS than White children.18 Using a multicenter administrative database of children’s hospitals, Wood et al found that, while Black children were more likely than White children to be evaluated with skeletal surveys, White children with skeletal surveys were more likely to be diagnosed with abuse.20 These findings suggest a potential higher threshold for ordering a skeletal survey in White children.20 More recently, Hymel et al found that minority children with low risk for AHT were more frequently screened for occult injury (ie, skeletal survey, retina exam) and reported to CPS than White children with low risk for AHT.15 Other studies have shown no differences in evaluation and reporting rates by race/ethnicity after adjusting for social factors (see Table).
As clinicians, one of our professional and ethical obligations is to “do no harm.” We must ask ourselves whether the existing structure of reporting is truly accomplishing this goal. How can we prevent one harm (maltreatment) without introducing other harms (eg, mistrust, trauma, stigmatization) in the evaluation and reporting process? Instead of focusing on simply more reporting, we should be focusing on more accurate and equitable reporting. Additionally, in order to promote good and to avoid unintended harm, there is a need to shift from tertiary prevention of abuse and neglect toward more primary and secondary prevention strategies, such as improving access to services that support families in caring for their children.
Promote accuracy in evaluation and reporting through clinician training. In order to improve clinicians’ accuracy in child abuse and neglect evaluation and reporting, we should expand clinician education in bias, inequities, and social determinants of health. We should also utilize the expertise of child abuse pediatricians. Child Abuse Pediatrics (CAP) is a fairly new subspecialty of general pediatrics in which physicians assess the likelihood of maltreatment, help identify or rule out conditions that may mimic maltreatment, and make recommendations about additional assessment, reporting, and treatment. CAP fellowship training requires education on social determinants of health and ethical issues related to diagnosis and reporting.21 Most CAPs staff work within a hospital or community-based multidisciplinary team (MDT), which, in addition to CAPs, may include CPS, law enforcement, social workers, family advocates, and mental health clinicians. Studies examining the role of CAP and MDT consultation have demonstrated reductions in the unwarranted reporting of noninflicted injuries to CPS,22,23 although the authors of these studies did not assess whether child race or ethnicity contributed to these effects.22,23 Nevertheless, the higher frequency of reporting of minority children with noninflicted injuries suggests that CAP and MDT involvement could benefit these children more than White children and could reduce disparities in reporting by race and ethnicity.
Promote equity in evaluation and reporting through the use of clinical decision support tools. Clinical guidelines, clinical pathways, standardized electronic medical record (EMR) tools, and prediction rules can decrease the likelihood of bias in the evaluation and reporting of maltreatment. For example, at one institution, the implementation of a clinical guideline for unwitnessed head injury in infants eliminated racial disparities in ordering of skeletal surveys.24 At another institution, the use of standardized child abuse EMR order sets led to compliance with American Academy of Pediatrics’ evidence-based guidelines that specify which children should be screened for physical abuse and with which tests.25 Clinical pathways can also increase the likelihood of consultation and evaluation by a hospital-based child protection team, as well as reduce socioeconomic disparities in the medical evaluation of suspected physical abuse.26 Several validated clinical prediction rules may also decrease bias. The TEN-4-FACESp clinical rule for predicting bruises caused by physical abuse had high sensitivity (ie, few false negatives) and high specificity (ie, few false positives) when used in children younger than 4 years who were seen in the emergency department.27 The Pediatric Brain Injury Research Network has also developed and evaluated a clinical prediction rule for identifying AHT.28,29 Best practice alerts or pop-up reminders in the EMR could trigger clinicians to use decision-making support tools (eg, standardized order sets, prediction tools, standardized report templates) when a child with signs of abuse and neglect presents in the clinical setting. These tools can help clinicians conduct thorough evaluations and make accurate determinations of the likelihood of abuse.
While improving accuracy and equity in evaluation and reporting of abuse and neglect is important, there is also a need to think about more upstream prevention solutions. The Centers for Disease Control and Prevention has published a technical report on evidence-based abuse and neglect prevention strategies, which focuses on 5 strategies: strengthening economic support for families, supporting positive parenting, providing quality early child care and education, augmenting parenting skills to facilitate healthy child development, and intervening to mitigate harms and prevent future risk.30 Interventions such as home visiting programs and parenting programs that promote positive parenting and enhance parenting skills have been shown to decrease maltreatment. The Nurse Family Partnership, a home visiting program in which specially educated nurses provide support to first time moms from pregnancy through the child’s second birthday, has been shown to significantly reduce child abuse and neglect, as well as risk factors for maltreatment.31,32 Long-term participation (4 to 6 years) in child-parent centers—an enrichment program with family engagement—was associated with a 33% reduction in substantiated maltreatment.33 Additionally, policies and supports that economically strengthen families, such as tax credits, subsidized child care, housing assistance, livable wages, and paid parental leave, have been shown to decrease the risk of child maltreatment.30,34,35,36,37 One study showed that paid parental leave was associated with reductions in hospitalization rates for AHT.35 Another study found that lack of waitlists to access subsidized child care decreased rates of child abuse and neglect, even after adjusting for known risk factors (eg, poverty, education level, unemployment).34
While all children are inherently vulnerable to abuse and neglect and deserving of protection, we need to acknowledge that our efforts to protect them can introduce unintended consequences when we overreport minority children and underreport White children. Decades of research reveal the existence of evaluation and reporting bias and the need to implement changes that promote accuracy and equity. At the same time, investing in evidence-based interventions that support families and prevent abuse and neglect would reduce the need for assessment and reporting and reduce demands on the child welfare system. Through such interventions, including expanded clinician education on maltreatment; utilization of child abuse pediatricians; development of abuse and neglect clinical pathways, guidelines, and prediction tools; and investment in upstream prevention services and supports, we can more equitably protect our children.
Raz M. Calling child protectives services is a form of community policing that should be used appropriately: time to engage mandatory reporters as to the harmful effects of unnecessary reports. Child Youth Serv Rev. 2020;110:104817.
How can child welfare leaders safely decrease investigation backlogs? Casey Family Programs. April 3, 2020. Accessed March 17, 2022. https://www.casey.org/child-welfare-leaders-safely-decrease-investigation-backlogs/#:~:text=Prioritize%20leadership%20involvement&text=Successful%20leadership%20strategies%20to%20reduce,the%20details%20of%20backlogged%20cases
Child Welfare Information Gateway. Caseload and workload management. Children’s Bureau, US Department of Health and Human Services; 2016. Accessed March 10, 2022. https://www.childwelfare.gov/pubpdfs/case_work_management.pdf
Choi MJ, Kim J, Roper A, LaBrenz CA, Boyd R. Racial disparities in assignment to alternative response. Child Youth Serv Rev. 2021;125:124.
Children’s Bureau. Child Maltreatment 2020. US Department of Health and Human Services; 2022. Accessed January 23, 2022. https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2020.pdf
Sedlack A, Mettenburg J, Basena M, et al. Fourth National Incidence Study of Child Abuse and Neglect (NIS-4): Report to Congress. US Department of Health and Human Services; 2010. Accessed January 23, 2022. https://www.acf.hhs.gov/sites/default/files/documents/opre/nis4_report_congress_full_pdf_jan2010.pdf
Sedlack A, McPherson K, Das B. Fourth National Incidence Study of Child Abuse and Neglect (NIS-4): Supplementary Analyses of Race Differences in Child Maltreatment Rates in the NIS-4. US Department of Health and Human Services; 2010. Accessed January 23, 2022. https://www.acf.hhs.gov/sites/default/files/documents/opre/nis4_supp_analysis_race_diff_mar2010.pdf
Hymel KP, Laskey AL, Crowell KR, et al. Racial and ethnic disparities and bias in the evaluation and reporting of abusive head trauma. J Pediatr. 2018;198:137-143.e1.
Putnam-Hornstein E, Prindle JJ, Leventhal JM. Prenatal substance exposure and reporting of child maltreatment by race and ethnicity. Pediatrics. 2016;138(3):e20161273.
Subboard of Pediatric Child Abuse. Content outline: child abuse pediatrics subspecialty in-training, certification, and maintenance of certification (MOC) examinations. American Board of Pediatrics; 2021. Accessed July 22, 2022. https://www.abp.org/sites/abp/files/pdf/chab.pdf
Anderst J, Kellogg N, Jung I. Is the diagnosis of physical abuse changed when child protective services consults a child abuse pediatrics subspecialty group as a second opinion? Child Abuse Negl. 2009;33(8):481-489.
Pierce MC, Kaczor K, Lorenz DJ, et al. Validation of a clinical decision rule to predict abuse in young children based on bruising characteristics. JAMA Netw Open. 2021;4(4):e215832.
Fortson BL, Klevens J, Merrick MT, Gilbert LK, Alexander SP. Preventing child abuse and neglect: a technical package for policy, norm, and programmatic activities. Centers for Disease Control and Prevention; 2016. Accessed September 22, 2022. https://www.cdc.gov/violenceprevention/pdf/can-prevention-technical-package.pdf
Klevens J, Barnett SB, Florence C, Moore D. Exploring policies for the reduction of child physical abuse and neglect. Child Abuse Negl. 2015;40:1-11.
Raissian K, Bullinger L. Money matters: does the minimum wage affect child maltreatment rates? Child Youth Serv Rev. 2017;72:60-70.



