In the Literature
Feb 2023
Peer-Reviewed

While adverse childhood experiences and trauma, including childhood abuse and neglect, have often been viewed from the lens of psychiatry, their influence on physical health, health behaviors, and factors that moderate health now garner more attention. This article reviews recent literature that has changed clinical and social viewpoints on child abuse and neglect and can be used as a primer to better understand (1) influences of child abuse and neglect on physical illness; (2) critical diagnostic advances relevant to persons who have experienced child abuse and neglect; and (3) ethical, research, and practical questions generated by these new understandings.
Increasing attention is being paid to the impact of child abuse and neglect on health. The rapidly growing knowledge base on long-term outcomes of those exposed to child abuse and neglect in the form of both trauma and adverse childhood experiences (ACEs), such as childhood economic hardship,1 neglect, sexual abuse, emotional abuse, discrimination, racism, household dysfunction, exposure to violence, parental mental illness, and parental substance use has warranted this attention.2 These types of maltreatment have often been viewed only from the lens of psychiatry, but it is now clear that, beyond their impact on mental health, these experiences affect biological mechanisms that influence physical health,3,4 health behaviors, and other factors that moderate good health, making it a general concern for all of health care and for those invested in improving health outcomes at large.
Given these wide-ranging health impacts, health care systems and individual practitioners must be prepared to evaluate childhood maltreatment-related health concerns. Many clinicians feel unprepared to do this sort of work, and it was likely absent from their training.5 This article aims to review recent core literature that has broadened medicine’s understanding of the forms of child abuse and neglect. It also provides a primer to better understand (1) the impact of child abuse and neglect on physical health; (2) critical diagnostic advances relevant to those who have experienced ACEs; and (3) the ethical, research, and practical issues that arise from this new understanding of child abuse and neglect.
In 1998, a Kaiser Permanente survey of adults revealed that ACEs were common among patients undergoing routine medical evaluations and were related to serious health risks and conditions in later life.6 More specifically, the researchers found that over half of 13 000 respondents had been exposed to at least one ACE, with risk for substance use, suicide attempts, and serious medical conditions—such as ischemic heart disease, cancer, and liver disease—increasing with the breadth of exposure to ACEs. The lifetime health effects of child abuse and neglect have since been researched and characterized in depth.7
In 2017, the American Heart Association published a scientific statement outlining the downstream effects of ACEs, which included trauma, on cardiac disease.8 Increased cardiac disease and cardiac disease risk factors in adults who experienced maltreatment as children are seen in mostly high-income countries.9,10,11,12,13,14,15,16 This cornerstone publication gave further scientific credence to the critical role of child abuse and neglect in physical health more generally. Specifically, it highlighted that ACEs affect physical health through 3 mechanisms: (1) change in health behaviors (eg, decreased physical activity, tobacco use), (2) biological embedding (eg, inflammation, abnormal endocrine function), and (3) increases in mental health problems. Given this broadened understanding, efforts are needed to mitigate the impact of child abuse and neglect on people’s overall health.
Currently, a patchwork of diagnostic concepts and standard methods of documenting trauma exist. Here, we focus on posttraumatic stress disorder (PTSD), which was first included in the Diagnostic and Statistical Manual of Mental Disorders (DSM)-III in 1980.17,18 As a construct, PTSD presents with diverse symptoms, creating diagnostic challenges in clinical work. There are over 630 000 different combinations of symptoms within the primary symptom clusters of PTSD (intrusive, avoidance, cognitive/affective, and arousal) in DSM-5.19,20 This level of heterogeneity has led many to question the validity of PTSD in its current form, and different phenotypes have been suggested based on biological studies and brain imaging.21 Moreover, it has been argued that existing DSM-5 diagnostic categories should include a code to specify the presence of trauma exposure.22 The identification of clinically relevant subgroups would contribute to more accurate diagnoses and better-tailored treatment modalities.
Two new diagnoses that are potentially relevant to child abuse and neglect have been proposed: complex PTSD (cPTSD)23 and developmental trauma disorder (DTD).24 However, these diagnoses have not been formally included in the DSM, seemingly due to ongoing debate about whether they should be separate from PTSD.25,26 The Table compares criteria for a diagnosis of PTSD and borderline personality disorder (BPD) to these newly proposed constructs.
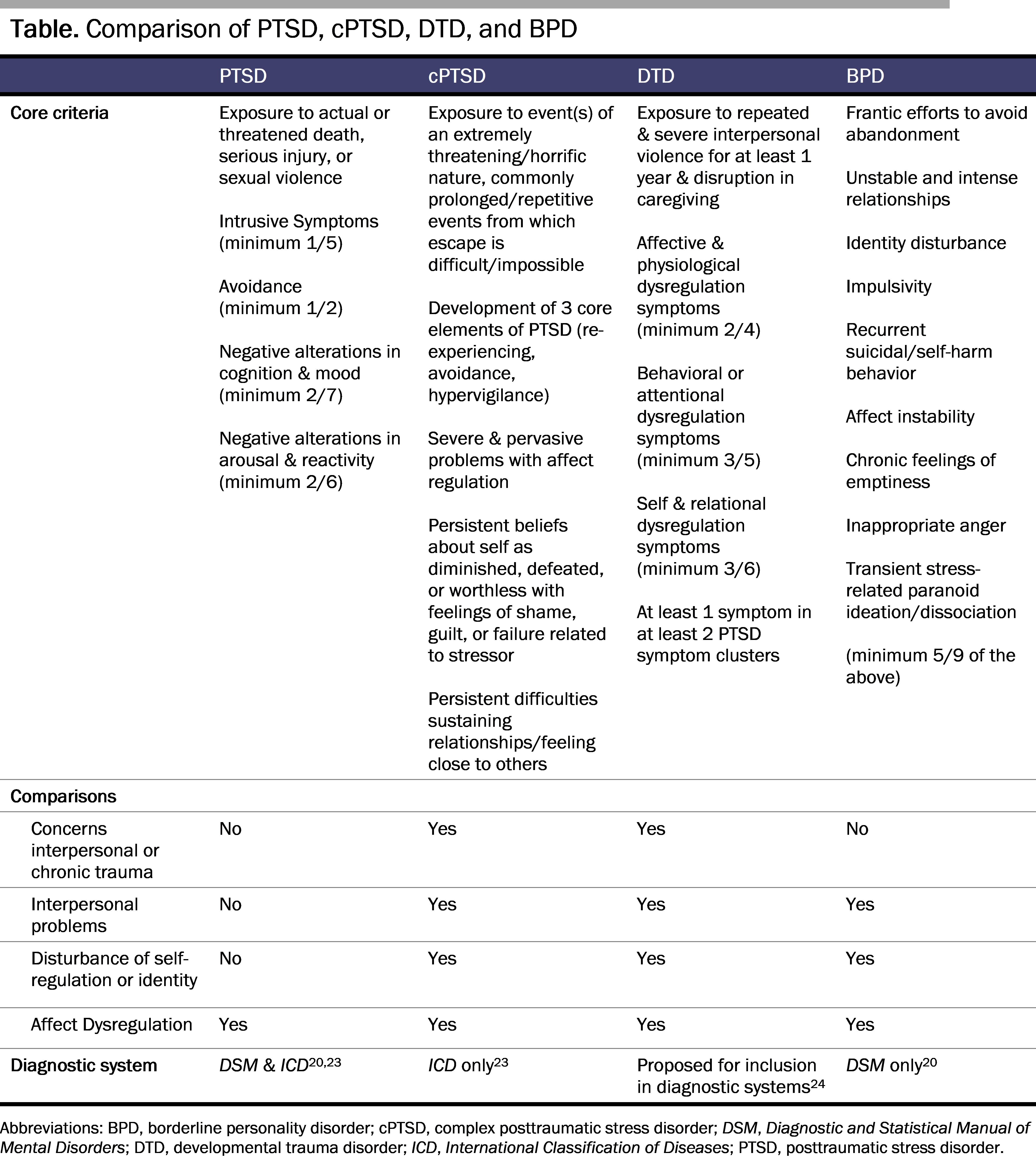
While not included in DSM-5, cPTSD is recognized in the 11th revision of the International Classification of Diseases23 and was previously under consideration for inclusion in DSM-IV as disorders of extreme stress not otherwise specified.27 It is intended to characterize symptoms experienced by survivors of prolonged or repeated trauma, especially trauma of an interpersonal nature. DTD is also intended to capture sequelae of interpersonal trauma, especially for children and adolescents,28 as criteria for PTSD are not met by many children affected by abuse and neglect.22
Although both cPTSD and DTD require the individual to meet some criteria for PTSD, these diagnostic categories place greater emphasis on the relational impact of trauma. Specifically, DTD requires the person to have experienced a disruption in caregiving and either self or relational dysregulation. cPTSD requires persistent difficulties in feeling close to others or in sustaining relationships. In contrast, while PTSD includes interpersonal symptoms, such as detachment from others and negative beliefs about others, one can meet criteria for the diagnosis without these.
Although having no criteria regarding trauma exposure, the diagnosis of BPD shares symptoms with PTSD, cPTSD, and DTD—namely, affect dysregulation, altered sense of self/identity, and relational issues. The possible role of child abuse and neglect in the development of this condition, as well as evidence of symptom overlap and comorbidity among these conditions, has led experts to conclude that they are related but distinct, creating additional layers of complexity in clinical work.29
An understanding of child abuse and neglect that transcends psychiatry and psychology means embracing an increasing amount of complexity and accepting pluralistic approaches to explanations and mechanisms of disease while striving for the highest level of application of our medical understanding of these conditions and related processes.30 In order to promote justice for those affected by child abuse and neglect across health systems, Teicher et al22 recently advanced 5 recommendations: (1) that clinicians screen all patients with mental illness for child abuse and neglect, (2) that diagnosis include a code to differentiate between those with abuse and neglect histories and those without, (3) that all treatment trials collect child abuse and neglect data for use as a moderator, (4) that research on biological bases of psychiatric disorders collect child abuse and neglect data, and (5) that concerted efforts be made to reduce child abuse and neglect and prevent development of related disorders in those exposed to it.
For public health professionals, upstream factors that precondition, precipitate, and perpetuate child abuse and neglect must be addressed if we are to effectively prevent serious medical illnesses such as cancer31 and heart disease.32 Preventing psychological trauma caused by racial-, ethnic-, gender-, and identity-based violence and victimization, hate crimes, and political violence should become a focal point, and structural factors that can be acted on to prevent trauma should receive more clinical and research attention.33
For health care systems and individual clinicians, serious consideration should be given to mechanisms to screen for and treat the sequela of ACEs and trauma, given that the risks and dangers of “therapeutic mislabeling”34 and misdiagnosis (with the potential for mismanagement) are high. A concerted effort needs to be made to screen patients effectively and empathically (without causing undue harm) while respecting the uniqueness and treatment wishes of each individual, since the extent to which these experiences affect the development, severity, or course of physical and mental illness—let alone how the individual will respond to specific treatments or treatment modalities—is unknown. Once widespread screening for ACEs has been implemented, efforts should be taken to ensure that such screening is thoughtful, considerate, and careful.35 Because responses to adverse experiences vary widely, some argue that screening for trauma symptoms, rather than for traumatic experiences alone, is preferable because it would identify children who would most benefit from trauma-specific treatment.36
Large-scale efforts are underway to improve trauma-informed care within primary care and pediatrics.37,38 Applying updated treatment recommendations for trauma-related conditions remains prudent.39,40,41 In clinical settings, screening for child abuse and neglect might help target interventions more effectively, and, in research on interventions, exposure to trauma should be regarded as a critical variable.
Braveman P, Heck K, Egerter S, Rinki C, Marchi K, Curtis M. Economic hardship in childhood: a neglected issue in ACE studies? Matern Child Health J. 2018;22(3):308-317.
Mehta D, Kelly AB, Laurens KR, et al. Child maltreatment and long-term physical and mental health outcomes: an exploration of biopsychosocial determinants and implications for prevention. Child Psychiatry Hum Dev. Published online September 29, 2021.
Pletcher BA, O’Connor M, Swift-Taylor ME, DallaPiazza M. Adverse childhood experiences: a case-based workshop introducing medical students to trauma-informed care. MedEdPORTAL. 2019;15:10803.
Kendall-Tackett KA. Treating the lifetime health effects of childhood victimization. 2nd ed. Civic Research Institute; 2013. https://www.civicresearchinstitute.com/toc/LHE%202nd%20TOC.pdf
Pierce JB, Kershaw KN, Kiefe CI, et al. Association of childhood psychosocial environment with 30‐year cardiovascular disease incidence and mortality in middle age. J Am Heart Assoc. 2020;9(9):e015326.
Chandan JS, Okoth K, Gokhale KM, Bandyopadhyay S, Taylor J, Nirantharakumar K. Increased cardiometabolic and mortality risk following childhood maltreatment in the United Kingdom. J Am Heart Assoc. 2020;9(10):e015855.
Rogers NT, Power C, Pinto Pereira SM. Child maltreatment, early life socioeconomic disadvantage and all-cause mortality in mid-adulthood: findings from a prospective British birth cohort. BMJ Open. 2021;11(9):e050914.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. American Psychiatric Association; 1980.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed. American Psychiatric Publishing; 2013.
6B41 Complex post traumatic stress disorder. In: International Classification of Diseases. 11th rev. World Health Organization; 2022. Accessed September 26, 2022. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/585833559
van Der Kolk B, Ford JD, Spinazzola J. Comorbidity of developmental trauma disorder (DTD) and post-traumatic stress disorder: findings from the DTD field trial. Eur J Psychotraumatol. 2019;10(1):1562841.
Ford JD, Spinazzola J, van der Kolk B, Grasso DJ. Toward an empirically based developmental trauma disorder diagnosis for children: factor structure, item characteristics, reliability, and validity of the developmental trauma disorder semi-structured interview. J Clin Psychiatry. 2018;79(5):17m11675.
Ford JD, Courtois CA. Complex PTSD and borderline personality disorder. Borderline Personal Disord Emot Dysregul. 2021;8(1):16.
American Medical Association. AMA principles of medical ethics. Code of Medical Ethics. Adopted June 1957. Revised June 2001. Accessed December 6, 2022. https://code-medical-ethics.ama-assn.org/principles
Magruder KM, McLaughlin KA, Elmore Borbon DL. Trauma is a public health issue. Eur J Psychotraumatol. 2017;8(1):1375338.
Finkelhor D. Screening for adverse childhood experiences (ACEs): cautions and suggestions. Child Abuse Negl. 2018;85:174-179.
Keeshin B, Byrne K, Thorn B, Shepard L. Screening for trauma in pediatric primary care. Curr Psychiatry Rep. 2020;22(11):60.
Duffee J, Szilagyi M, Forkey H, Kelly ET. Trauma-informed care in child health systems. Pediatrics. 2021;148(2):e2021052579.
Ford JD, Courtois CA, Herman JL, van der Kolk BA. Treating Complex Traumatic Stress Disorders in Adults: Scientific Foundations and Therapeutic Models. 2nd ed. Guilford Publications; 2020.
Martin A, Naunton M, Kosari S, Peterson G, Thomas J, Christenson JK. Treatment guidelines for PTSD: a systematic review. J Clin Med. 2021;10(18):4175.