Art of Medicine
Dec 2022
Peer-Reviewed

Identity formation is a critical moral psychological feature of ethics that is often neglected in health professions education. Inner transformation has been philosophically key from antiquity to the present day, especially for thinkers like Gilles Deleuze and Georges Bataille. Francis Bacon, a favorite thinker and painter of Deleuze, specifically inspired meditation on images of corporeal suffering as part of a “spiritual ordeal” that can provoke a kind of transformation key to health professionalism, deepening human solidarity. This article considers this theme in historical, social, and cultural contexts and as an ethical foundation of some of the earliest known hospitals as well as contemporary pursuits of health equity and moral formation in the health professions.
Let all mortal flesh be silent, and stand with fear and trembling…
Divine Liturgy of St James1
Ethical progress requires what might be called internal and external change. The external side of health care ethics—policies, research, and institutions—is often the predominant focus. Far more challenging is the internal side of medical ethics: How does one become an ethical healer? Asking such questions is fraught. Professionalism has been the dominant grammar to speak about the internal aspect of ethical comportment in medicine. But prominent critics have claimed that the mainstream professionalism and medical ethics discourse has been, at the very least, insufficiently formative2,3 and, at worst, protective of patriarchal, economic, and White-guild power.4,5 Furthermore, external ethical action—for example, changing or designing institutional and communal forms—requires being the “right kind of person” for the task, and inner ethical strength is required to resist the deforming nature of unethical external systems. Thus, having a robust ethical inner life is a prerequisite for genuinely ethical medicine. But how can this inner life be developed? As will be discussed in this article, meditative reflection on arresting—even grotesque—images of suffering and illness can be a method to develop inner self-transformation in relation to the world, enabling solidarity with patients and peers. Similar contemplation of the poverty and abject suffering of marginalized people in the 4th century CE gave rise to the birth of the hospital, and, in the same way, contemplation of contemporary images of use of force and torture could motivate institutional change.
Since the time of the ancient philosophers, the task of inner self-transformation (in Greek, askesis) has been consistently recognized as an essential component of the ethical life. But just as consistently, there have been disagreements over the means to and ends of such a change. Classical Stoic philosophers sought self-discipline and cultivated a “negative” apatheia—minimizing the influence of external events on one’s emotional life6—but today we require a “positive” transformation toward compassion, solidarity, and agency. These qualities, although “public” in nature, require one’s inward journey of askesis to be tied to the world around one and to the people in it. Inner transformation comes through both inward reflection and external interaction, leading one to further engage with one’s neighbor.
French postwar philosophers Georges Bataille and Gilles Deleuze were proponents of this new model of askesis. Janae Sholtz describes Bataille’s and Deleuze’s exploration of “radically jarring meditative exercises” or “spiritual ordeals” to move beyond our old selves and overcome indifference, apathy, or passive acceptance of the status quo.6 Bataille, for example, searched for a way to “get out of oneself,” and there are a variety of experiences—laughter, ecstasy, torture, anguish, eroticism—that he identifies to do so, precisely because they expose us to our limits and human finitude. One of Bataille’s favorite techniques was meditation on transfixing images—such as those of torture—because such images operate “through contagion and force”: they transfix him, and he can neither keep looking nor turn away. As described by Sholtz, the “pure violence of the image itself” arouses a kind of “affective contagion” that causes “laceration of the isolated self.”6 In Bataille’s words, “The sight—horrible—of torture opens the sphere that enclosed (or limited) my personal particularity, it opens it violently, lacerates it.”7 In short, the individual’s preoccupation with the self is shattered by the power of the image.
There are many historical examples of transfixing images of violence that have spurred this laceration of the personal sphere, engendering solidarity and engagement. To name a few, pictures of the horrors of the Holocaust have played a role in ongoing work against anti-Semitism and ethnic cleansing/genocide worldwide. Nationwide broadcasting of footage of the Edmund Pettus Bridge in Selma on “Bloody Sunday” turned the tide of the civil rights movement, drawing more people from all over the country to participate.8 More recently, the images of George Floyd’s murder have shown the personally transformative and socially revolutionary power of such images. As strange as Bataille’s suggestion may at first seem, meditation on particularly intense images certainly has the power to change the world. Rather than dehumanizing the other, beholding such images can simultaneously increase compassion and desensitize us just enough to get our hands dirty. The suffering other, whose image has lacerated one’s own personal sphere, demands a response.
The 20th-century painter Francis Bacon was the creator of a series of images that evoke ghastly flesh, although his work pushes even beyond the human form. Bacon blurs the boundary between man and beast by dismantling human forms (such as in his famous series of “screaming” Pope heads, deconstructions of Velázquez’s famous portrait of Pope Innocent X9) and by giving nonhuman forms emotional voice, as can be seen in his Fragment of a Crucifixion or Three Studies for Figures at the Base of a Crucifixion.10,11
Figure 1. Head 1, 1948 (CR 48-01), by Francis Bacon

© The Estate of Francis Bacon. All rights reserved. DACS, London/Artists Rights Society, New York 2022.
Figure 2. Fragment of a Crucifixion, 1950 (CR 50-02), by Francis Bacon
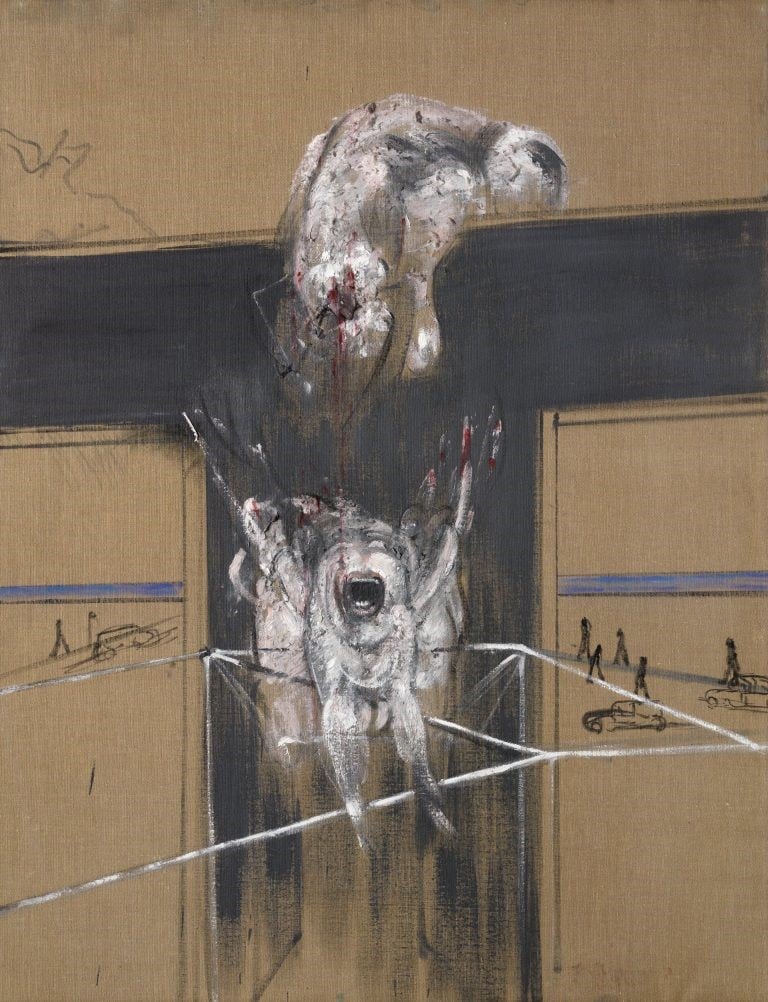
© The Estate of Francis Bacon. All rights reserved. DACS, London/Artists Rights Society, New York 2022.
Figure 3. Three Studies for Figures at the Base of a Crucifixion (CR 44-01), 1944, by Francis Bacon
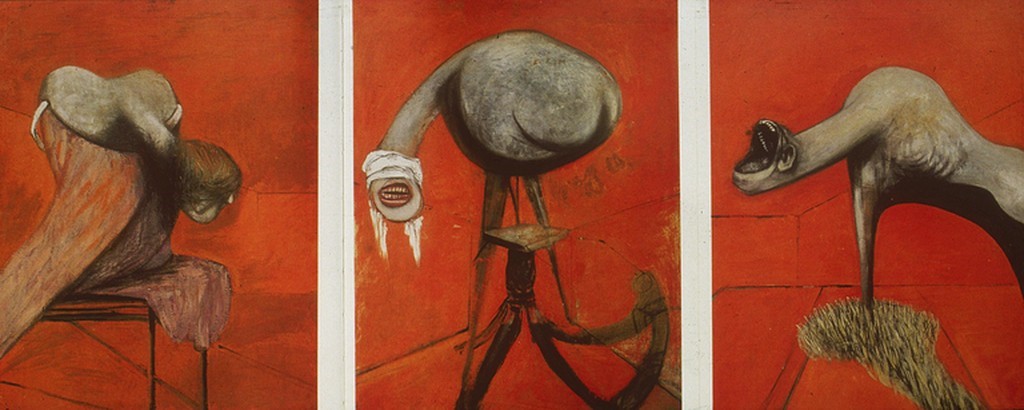
© The Estate of Francis Bacon. All rights reserved. DACS, London/Artists Rights Society, New York 2022.
Bacon’s work captivated Deleuze, who used it as a conceptual launching pad for his theory of art and sensation. The silent vocalization of the monstrous flesh that Bacon portrays draws the viewer with its intensity and depiction of a near-otherworldly (yet human) form. What is this vocalization, and why can it make us feel both vulnerable and finite, amplifying our awareness of suffering in ourselves and others? Deleuze writes of Bacon’s art:
The mouth … turns all meat into a head without a face. It is no longer a particular organ, but the hole through which the entire body escapes, and from which the flesh descends…. This is what Bacon calls the Scream, in the immense pity that the meat invokes.12
This pity is an affective response of compassion, spurred by personal identification with the grotesque form of the “meat.” Bacon depicts a space where, as Deleuze writes: “Man becomes animal, but not without the animal becoming spirit at the same time, the spirit of man.… It is never a combination of forms, but rather the common fact: the common fact of man and animal.”12 Ceaselessly pursuing the root of all corporeal solidarity, he goes from body to flesh and, finally, to meat: “Meat is the common zone of man and the beast … a state where the painter identifies with the objects of his horror and his compassion,”12 because “he goes to the butcher’s shop as if it were a church, with the meat as the crucified victim.”12 Invocation of the meat as “crucified victim” sacralizes, and thereby humanizes, all flesh—be it animal or human. Humanization of all flesh affirms its value and maintains our gaze—rescuing it from the dehumanization and abstraction that it undergoes. Far from being a mere reduction of flesh to the inhuman, Bacon’s work elicits compassion and solidarity—hard-won through horror and close attention—qualities that shared vulnerability in flesh brings into existence. For Deleuze, Bacon’s artwork is “of a very special violence,” which manifests a certain “zone of indiscernibility”12 that blurs the distinctions we draw between flesh: it is both human and nonhuman, alive and dead, healthy and suffering. To focus on these images is to sink into our own corporeal vulnerability and meditate on our past, present, or future sufferings.
What has all this to do with health care ethics? Medicine cannot be ethical if it does not prioritize an unflinching focus on suffering bodies over and against our inborn tendency to turn away, especially from the bodies of the poor. Because disease makes its own “preferential option for the poor,”5 any moral system of healing must be well acquainted with suffering, smells, sickness, and death—even if it also means blurring the distinction between the (healthy, put-together) us and the (needy, dependent) them via the spirited solidarity of all meat.
Suffering. The founding of the hospital was one such place where close attention to suffering bodies gave rise to a new moral ethos for medical practitioners, thereby creating a new institutional form and sustainable culture of care. Individual askesis led to lasting social change. In Asia Minor in the 4th century CE, St Basil the Great founded his City of Mercy (later known as the Basilead)—the institutional genesis of the hospital form—which offered professional medical care, a centralized location, overnight stays, and nursing, all of which were free for all. His close companion St Gregory of Nazianzus explains this community’s ethos of care, while criticizing Greco-Roman culture for its avoidance of the sick and its equation of illness with social worthlessness. In a fundraising speech, he describes the plight of those with the “sacred disease” of leprosy:
No one would believe who has not seen it: human beings alive yet dead, disfigured in almost every part of their bodies, barely recognizable for who they once were or where they came from; or rather, the pitiful wreckage of what had once been human beings. By way of identification they keep calling out the names of their mothers and fathers, brothers, and places of origin: “I am the son of so-and-so. So-and-so is my mother. This is my name. You used to be a close friend of mine.” And this they do because they cannot be identified from the way they used to look…. Who know[s] whether they should grieve more for the limbs they have lost or for those they have left[?]13
Are these leprous bodies not Bacon’s screaming forms? Gregory gives grisly detail to enjoin his audience to remember “the fact that we are flesh and compassed in a lowly body, and we are so derelict in our obligation to look after our fellow man that we actually believe that avoiding these people assures the well-being of our own persons.”13 This foundational ethos of attention amidst dehumanization reaffirms that we are bound together in one body, and the weal and woe of one affects all.
Restraints. A more contemporary example involves the use of force in medicine. While some use of physical and chemical restraints unfortunately remains necessary,14 it is nevertheless the case that their (over)use is increasingly being called into question. The burden of force in clinical settings falls disproportionately on minoritized patients,15 and, undoubtedly, the poor; it also reflects underfunding (via unsafe staffing ratios) and continues the carceral logic of health care. Indeed, there has been a growing movement known as abolition medicine in academic and activist spaces that is challenging this logic and imagining new possibilities.16,17
What is the role of images and their transforming power here? With respect to restraints, perhaps visuals depicting patients’ distress at their restraints would be instructive, as physicians are apt to leave the room, put in the orders, and let others do the “dirty work”—at best, to minimize voyeurism and, at worst, to escape discomfort with what is happening. This response could be contrasted with the “positive” example of Tony Robert-Fleury’s famous 1876 painting, Pinel Freeing the Insane, a classic study of liberation from (medical) restraint.18
Torture. The furthest extremes of contemporary US physicians’ inappropriate engagement with violence, however, are their documented participation in modern capital punishment and participation in torture during the War on Terror.19 Public reports and deeply disturbing photos going back to the early years of the War on Terror helped galvanize public consciousness.20 CIA-run “black sites” (secret prisons) were sites of deep medical complicity with violence, where a “‘board-certified physician’ was in the room for every session of waterboarding”19 and where medical officers participated in “rectal rehydration” of patients who refused oral intake (a practice Physicians for Human Rights has called “sexual assault masquerading as medical treatment.”)21 Perhaps via images of such terrible deeds, Bataille’s “pure violence of the image itself” would effect a “laceration” of our personal—indeed, professional—identity, shattering both our self-preoccupation as well as our assumed benevolence, and spurring viewers to contend ever more forcefully for a holistically healing profession.
To take another example of how images of torture can lead to activism, in 2006, medical professionals in North Carolina caused a decade-long pause in executions after professional organizations prohibited participation and ceased working with the state Department of Corrections; at roughly the same time, a documentary (filmed in 2005) was produced by the Death Penalty Photography Project giving a behind-the-scenes look at North Carolina’s death row.22
While it is difficult to neatly draw lines of causation, visual exposure to the reality of terrible suffering seems to have strengthened protests against medicine’s involvement in such violence. Just as the early Christian focus on the suffering body led to a burst of institutional creativity, so these modern images of suffering also instill personal conviction and motivate institutional change, revealing the inextricable connections between internal and external transformation.
As intimate witnesses to suffering not unlike Basil the Great, Gregory of Nazianzus, or modern viewers of images of torture or capital punishment, we—as the result of our askesis—might similarly strive for a new moral ethos centered on social responsibility, justice, and equity in health care. To insistently gaze upon broken bodies reminds us of the fact of suffering and compels us to prioritize life over and against our desire to run away from suffering and our fears of dependence and death. This task is especially necessary in a profession like medicine, which has drawn primarily from privileged groups for its membership.
Perhaps our usual fears of contagion, suffering, and death are the aspect of “normal” (ie, status quo) psychology that Bataille attempted to surmount in order to make an ethical life of solidarity possible. Yet to attain such a state, (trans)formational cultures, relationships, and institutions are necessary; the solidarity of all flesh that they enable has obvious implications not only for medicine but also for contemporary issues such as biosphere destruction and climate change.23 Bataille and Deleuze set up the problematic to which Francis Bacon and the origins of the hospital provide a possible solution: a close viewing of ghastly bodies that, paradoxically, pushes us towards a profound solidarity with all suffering flesh.
Divine Liturgy of St James. II, XVI. Accessed August 16, 2022. https://www.newadvent.org/fathers/0717.htm
Antiel RM, Kinghorn WA, Reed DA, Hafferty FW. Professionalism: etiquette or habitus? Mayo Clin Proc. 2013;88(7):651-652.
Eskow R. “Operation Coffeecup”: Reagan, the AMA, and the first “viral marketing” campaign ... against Medicare. HuffPost. April 10, 2007. Accessed April 20, 2021. https://www.huffingtonpost.com/rj-eskow/operation-coffeecup-reaga_b_45444.html
Farmer P. Pathologies of Power: Health, Human Rights, and the New War on the Poor. University of California Press; 2003.
Bataille G. Guilty. Kendall S, trans. Suny Press; 2011.
Glass A. Civil Rights march ends as “Bloody Sunday,” March 7, 1965. Politico. March 7, 2018. Accessed July 20, 2022. https://www.politico.com/story/2018/03/07/this-day-in-politics-march-7-1965-437394
Bacon F. Study After Velázquez's Portrait of Pope Innocent X, 1953. Oil on canvas, 60" x 46". Des Moines Art Center, Iowa.
Bacon F. Fragment of a Crucifixion, 1950. Oil, cotton wool and canvas, 55" x 42.7". Vanabbemuseum, Eindhoven, The Netherlands.
Bacon F. Three Studies for Figures at the Base of a Crucifixion, 1944. Oil and pastel on fiberboard, 2′ 5″ x 3′ 1″. Tate Gallery, London.
Deleuze G. Francis Bacon: The Logic of Sensation. Smith D, trans. Continuum; 2005.
St Gregory of Nazianzus. Select Orations. Vinson M, trans. Catholic University of America Press; 2003.
George CE. What might a good compassionate force protocol look like? AMA J Ethics. 2021;23(4):E326-E334.
Valtis YK, Stevenson KE, Murphy EM, et al. Race and ethnicity and the utilization of security responses in a hospital setting. J Gen Intern Med. Published online May 13, 2022.
Iwai Y, Khan ZH, DasGupta S. Abolition medicine. Lancet. 2020;396(10245):158-159.
Fee E, Brown TM. Freeing the insane. Am J Public Health. 2006;96(10):1743.
Rosenberg C. Guantánamo testimony exposes role of doctors in CIA interrogations. New York Times. January 27, 2020. Accessed July 14, 2022. https://www.nytimes.com/2020/01/27/us/politics/cia-black-site-doctors.html
Hersh S. Torture at Abu Ghraib. New Yorker. April 30, 2004. Accessed July 15, 2022. https://www.newyorker.com/magazine/2004/05/10/torture-at-abu-ghraib
CIA torture report highlights unnecessary medical procedure: rectal hydration and rectal feeding is not medically justified. News release. Physicians for Human Rights; December 10, 2014. Accessed July 15, 2022. https://phr.org/news/cia-torture-report-highlights-unnecessary-medical-procedure/
Langley S. Death Penalty Documentary: Execution Tour of NC Death Row. Death Penalty Photography Project; 2008. Accessed July 15, 2022. https://www.youtube.com/watch?v=AJFtAjzljGg
Kolbert E. The Sixth Extinction: An Unnatural History. Henry Holt & Co; 2014.



