Policy Forum
Jan 2022
Peer-Reviewed
Integrating primary and oral health care is critical to improving population health and addressing health inequity exacerbated by the COVID-19 pandemic. Leaders of the patient-centered medical home (PCMH) movement focused on building consensus for the PCMH model among diverse stakeholders in order to enhance infrastructure investment, care innovation, and payment reforms that support access and equity. This article offers 5 lessons from the PCMH movement to inform primary and oral health care integration.
Consumers want primary care that is accessible, comprehensive, coordinated, and responsive to overall health and well-being and that integrates oral and behavioral services.1 However, despite the fact that comprehensive primary care improves population health and reduces inequity,2,3,4 this care is hard for patients to find because of siloed payment, insurance, and delivery streams. The COVID-19 pandemic has further weakened primary care and exacerbated inequity.5,6 Yet primary care innovators who have built momentum over the last decade might still help increase access to comprehensive care by creating patient-centered medical homes (PCMHs)7 that can connect silos. PCMHs offer advanced primary care models that do the following:
PCMHs have been widely adopted by commercial health plans, states, and federally qualified health centers (FQHCs). As of 2010, 44 states and the District of Columbia had passed 330 laws to support and incentivize medical homes.8 White and Twiddy reported in 2017 that 45% of family physicians practice in a PCMH,9 and the American Medical Association showed that 32% of physicians in 2018 participated in a medical home.10,11
The 2007 Joint Principles of the PCMH, which guided the development of this advanced primary care model, were updated in the 2017 Shared Principles of Primary Care12,13 (see Figure 1), now embraced by over 350 organizations.14
Figure 1. Shared Principles of Primary Carea

a Adapted from Epperly T, Bechtel C, Sweeney R, et al.12
Each principle is germane to primary and oral health care integration. The principle of comprehensive and equitable care deserves particular attention here, since it encourages disease prevention and intervention strategies’ inclusion of general medical, mental health, and oral health services, as well as social determinants of health, which are often overlooked and undervalued in siloed service delivery streams. In 2013, the Substance Abuse and Mental Health Services Administration-Health Resources and Services Administration Center for Integrated Health Solutions created a framework of 6 levels of integrated health care (see Figure 2).15,16
Figure 2. A Standard Framework for Levels of Integrated Health Carea

a Reproduced from Heath B, Wise Romero P, and Reynolds K.16
Models of care based on this framework included co-located dental hygienists or full-service dental clinics but didn’t offer system-wide integration of whole-person care. Most ambulatory visits in the United States are to primary care clinicians,17 which is no wonder, since 61 million people live in dental health professional shortage areas (HPSA) and 124 million live in mental HPSAs.18
The following data suggest that primary care equipped to meet patients’ needs holistically must offer a range of services (eg, screening, education, interventions, appropriate referrals) in general medicine, mental health, and oral health.
General medical, mental health, and oral health care integration can be guided by 5 lessons from the adoption of PCMHs.
Lesson 1: compile evidence. Evidence offers exemplars of implementation successes and failures, which can enable articulation of shared values that spur engagement, motivate communication and consensus, and forge innovation in education, policy, advocacy, and research. In mental health, for example, the IMPACT study, published in 2002, provided evidence that late-life depression intervention in primary care settings reduced depressive symptoms relative to usual care,30 which led the National Council for Community Behavioral Healthcare to define mental health roles for PCMHs in 2009.31 In 2010, the Milbank Memorial Fund published Evolving Models of Behavioral Health Integration in Primary Care,32 which described how to nationally scale mental health integration to improve depression intervention outcomes,33,34 increase adherence,35 and support quality of life.36
A nascent evidence base for oral health integration is being formed from insurance claims data on positive outcomes for at-risk patients who received combined medical and dental care.37,38,39 Since 2009, the National Interprofessional Initiative on Oral Health (NIIOH) has convened diverse stakeholders to create a framework for integrating oral health care into primary care. NIIOH also participated in the US Health Resources and Services Administration’s consensus process that defined core clinical oral health competencies for primary care clinicians.40 NIIOH continues to support Smiles for Life,41 a free online primary care oral health curriculum, and the Oral Health Delivery Framework,42,43 which offers sample workflows for stepwise, incremental integration of oral health into primary care (see Figure 3). The Primary Care Collaborative (PCC) also convened diverse leaders to report on oral health care and primary care integration with a view to compiling and disseminating exemplar oral health integration models.44
Figure 3. Oral Health Delivery Frameworka
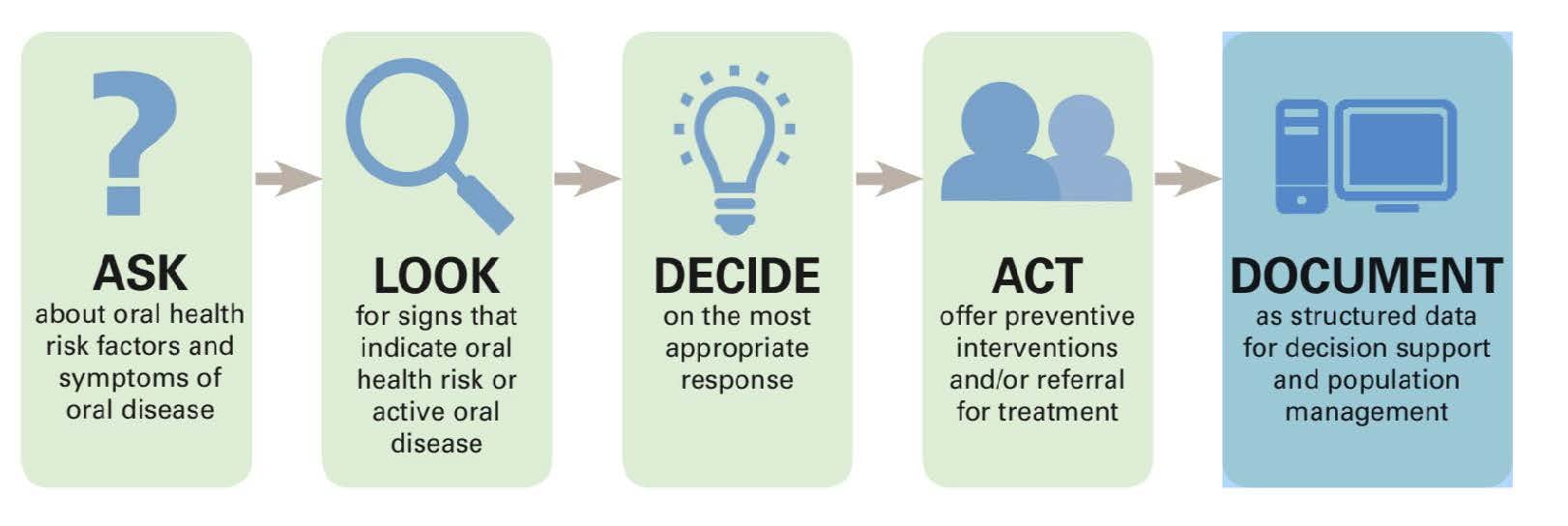
a Reproduced from Hummel J, Phillips KE, Holt B, Hayes C.43 Reprinted by permission of Jeffrey Hummel.
Lesson 2: collaborate. Care delivery innovations affect a range of stakeholders (eg, payers, policymakers, clinicians) with competing interests. Inclusive co-creation of a shared vision of the future state of health care generates buy-in, and buy-in makes for easier implementation. The PCC’s team-based advocacy efforts, for example, have generated widespread adoption of PCMHs by federal and state agencies and insurers.45 Together with the National Alliance of Healthcare Purchaser Coalitions and the Pacific Business Group on Health, the PCC released 7 new attributes of advanced primary care models that align shared principles, including mental health integration.46 Similar collaborative effort could be replicated for oral health integration.
Lesson 3: reform both service delivery and payment streams. Although PCMHs have demonstrated some improvements in cost and quality, many experts believe that the model is underpowered because payment structures do not support team-based care.47 Primary care is still largely fee-for-service and makes up only 5% to 7% of total US health care spending,48,49,50 so organizations’ investment in primary care is low. More than 60% of primary care practices’ revenue must come from prospective payments in order to substantially reform care delivery without fiscal loss.51 Reliance on fee-for-service hampers practices’ capacity to offer comprehensive services via cross-disciplinary teams.52 To help practices with financial obstacles to integration, the AIMS Center for Advancing Integrated Mental Health Solutions53 offers resources (eg, bundled payment models, collaborative care codes) for managing fiscal demands of mental health integration. Texas, for example, began contracting with Medicaid to integrate services and reduce fragmented care.54 Reformers need examples of financially successful integration models to co-locate oral health and primary care in FQHCs and bundle benefits in some Taft-Hartley plans.55
Lesson 4: motivate equity. Initially, the value proposition of PCMH focused more on cost than quality, but both are key to promoting equity, particularly as we emerge from the COVID-19 pandemic. Before the pandemic, one-third of US adults lacked dental insurance,56 and Americans with low incomes or without health insurance were less likely to have visited a dentist within a year.57,58 Before the pandemic, Black and Brown communities had lower rates of annual dental visits and higher rates of tooth decay and tooth loss.59,60,61 The COVID-19 pandemic has likely worsened these outcomes, as many lost employer-sponsored insurance that included some coverage of dental services.62,63,64
Lesson 5: invest in metrics infrastructure. As with organizational transitions to PCMHs, infrastructure investments are prerequisites for integration. Most primary care electronic health record (EHR) systems lack oral health fields, which impedes interoperability, data and analytics collection, care coordination, and key performance indicator tracking and reporting needed to ensure value-based care and payment. Public and private insurers can help incentivize organizational investment in EHR architecture that enables innovation and integration. Of 1100 metrics endorsed by the National Quality Forum’s Quality Positioning System, we identified 122 primary care metrics and 9 oral health metrics.65 A standardized and reliable measure of caries, for example, is essential to meaningful integration of oral health into primary care.
Equitable care of patients and communities requires integrating mental health and oral health into primary care. We envision comprehensive, patient-centered service delivery streams that prioritize prevention, value, and national scalability of standard-of-care exemplars that we all want and deserve.
Community Catalyst. In their words: consumers’ vision for a person-centered primary care system. Center for Consumer Engagement and Health Innovation. November 2019. Accessed March 4, 2021. https://www.healthinnovation.org/resources/publications/body/In-Their-Words-Consumers-Vision-for-a-Person-Centered-Primary-Care-System.pdf
Berkowitz SA, Cené CW, Chatterjee A. Covid-19 and health equity—time to think big. N Engl J Med. 2020;383(12):e76.
Egede LE, Walker RJ. Structural racism, social risk factors, and Covid-19—a dangerous convergence for Black Americans. N Engl J Med. 2020;383(12):e77.
American Academy of Family Physicians; American Academy of Pediatrics; American College of Physicians; American Osteopathic Association. Joint principles of the patient-centered medical home. March 2007. Accessed October 19, 2020. https://www.aafp.org/dam/AAFP/documents/practice_management/pcmh/initiatives/PCMHJoint.pdf
Bernstein J, Chollet D, Peikes D, Peterson GG. Medical homes: will they improve primary care? Math Policy Res. 2010;6:1-5. Accessed August 17, 2021. https://www.pcpcc.org/sites/default/files/resources/Medical%20Homes%20Will%20They%20Improve%20Primary%20Care.pdf
Rama A. Payment and delivery in 2018: participation in medical homes and accountable care organizations on the rise while fee-for-service revenue remains stable. American Medical Association; 2019. Accessed August 17, 2021. https://www.ama-assn.org/system/files/2019-09/prp-care-delivery-payment-models-2018.pdf
Rama A. Payment and delivery in 2016: the prevalence of medical homes, accountable care organizations, and payment methods reported by physicians. American Medical Association; 2017. Accessed November 10, 2021. https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/health-policy/prp-medical-home-aco-payment.pdf
Shared principles of primary care FAQ. Primary Care Collaborative. Accessed August 24, 2021. https://www.pcpcc.org/content/shared-principles-primary-care-faq
Shared principles signers. Primary Care Collaborative. Accessed June 17, 2021. https://www.pcpcc.org/principles/signers
Heath B, Wise Romero P, Reynolds K. A standard framework for levels of integrated healthcare. SAMHSA-HRSA Center for Integrated Health Solutions; April 2013. Accessed November 10, 2021. https://www.pcpcc.org/sites/default/files/resources/SAMHSA-HRSA%202013%20Framework%20for%20Levels%20of%20Integrated%20Healthcare.pdf
Rui P, Okeyode T. National Ambulatory Medical Care Survey: 2016 national summary tables. Centers for Disease Control and Prevention. Accessed November 10, 2021. https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2016_namcs_web_tables.pdf
Shortage areas. Health Resources and Services Administration. Updated November 9, 2021. Accessed November 10, 2021. https://data.hrsa.gov/topics/health-workforce/shortage-areas
Periodontal disease fact sheet. American Academy of Periodontology.
Michalowicz BS, Hodges JS, DiAngelis AJ, et al; OPT Study. Treatment of periodontal disease and the risk of preterm birth. N Engl J Med. 2006;355(18):1885-1894.
Robinson P, Reiter J. Behavioral Consultation and Primary Care: A Guide to Integrating Services. Springer; 2016.
Substance Abuse and Mental Health Services Administration. Mental and substance use disorder treatment for people with physical and cognitive disabilities. HHS publication PEP19-02-00-002. 2019. Accessed August 17, 2021. https://store.samhsa.gov/sites/default/files/d7/priv/pep19-02-00-002_508_022620.pdf
Wall T, Nasseh K, Vujicic M; Health Policy Institute. Majority of dental-related emergency department visits lack urgency and can be diverted to dental offices. American Dental Association; August 2014.
Atchison KA, Rozier RG, Weintraub JA. Integration of oral health and primary care: communication, coordination, and referral. NAM Perspect. October 8, 2018. Accessed November 10, 2021. https://nnoha.org/nnoha-content/uploads/2019/12/Integration-of-Oral-Health-and-Primary-Care.pdf
Unützer J, Katon W, Callahan CM, et al; IMPACT Investigators. Improving mood-promoting access to collaborative treatment. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA. 2002;288(22):2836-2845.
Mauer BJ. Behavioral health/primary care integration and the person-centered healthcare home. National Council for Community Behavioral Healthcare; April 2009. Accessed October 7, 2020. https://www.thenationalcouncil.org/wp-content/uploads/2018/10/BehavioralHealthandPrimaryCareIntegrationandthePCMH-2009.pdf?daf=375ateTbd56
Collins C, Hewson D, Munger R, Wade T. Evolving Models of Behavioral Health Integration in Primary Care. Milbank Memorial Fund; 2010. Accessed October 19, 2020. https://www.milbank.org/wp-content/uploads/2016/04/EvolvingCare.pdf
Tice JA, Ollendorf DA, Reed SJ, Shore KK, Weissberg J, Pearson SD. Integrating Behavioral Health Into Primary Care: A Technology Assessment. Institute for Clinical and Economic Review; 2015. Accessed November 10, 2021. https://collections.nlm.nih.gov/master/borndig/101679435/Integrating%20Behavioral%20Health%20into%20Primary%20Care.pdf
Community Guide (Guide to Community Preventive Services). Mental health. Accessed October 11, 2020. https://www.thecommunityguide.org/topic/mental-health
US Department of Health and Human Services. Integration of oral health and primary care practice. Health Resources and Services Administration; February 2014. Accessed November 10, 2021. https://www.hrsa.gov/sites/default/files/oralhealth/integrationoforalhealth.pdf
About us. National Interprofessional Initiative on Oral Health. Accessed August 17, 2021. https://www.niioh.org/content/about-us
Hummel J, Phillips KE, Holt B, Hayes C. Oral health: an essential component of primary care. Qualis Health; June 2015. Accessed March 6, 2021. http://www.safetynetmedicalhome.org/sites/default/files/White-Paper-Oral-Health-Primary-Care.pdf
Primary Care Collaborative. Innovations in oral health and primary care integration: alignment with the shared principles of primary care. January 2021. Accessed July 7, 2021. https://www.pcpcc.org/sites/default/files/resources/PCC_Oral_Health_Primary_Care_Integration.pdf
Palino D, Ramey B. Trusted Healers: Dr Paul Grundy and the Global Healthcare Crusade. Köehler Books; 2019.
PCC, National Alliance of Healthcare Purchaser Coalitions and Purchaser Business Group on Health Announce new attributes of advanced primary care. News release. Primary Care Collaborative; December 1, 2020. Accessed July 7, 2021. https://www.pcpcc.org/2020/11/24/pcc-national-alliance-healthcare-purchaser-coalitions-and-purchaser-business-group-health
Kempski A, Greiner AC. Primary care spending: high stakes, low investment. Primary Care Collaborative; 2020. Accessed July 7, 2021. https://www.pcpcc.org/sites/default/files/resources/PCC_Primary_Care_Spending_2020.pdf
AIMS Center. Billing and financing: behavioral health integration and collaborative care. University of Washington. Accessed March 6, 2021. https://aims.uw.edu/collaborative-care/financing-strategies-behavioral-health-integration-and-collaborative-care
Wells R, Breckenridge ED, Ajaz S, et al. Integrating primary care into community mental health centers in Texas, USA: results of a case study investigation. Int J Integr Care. 2019;19(4):1.
Taft-Hartley and federal plans. CIGNA®. Accessed June 30, 2021. https://www.cigna.com/employers-brokers/who-we-serve/taft-hartley
Reinberg S. Even before the pandemic, one-third of US adults went without dental care. US News and World Report. July 9, 2021. Accessed August 30, 2021. https://www.usnews.com/news/health-news/articles/2021-07-09/even-before-pandemic-one-third-of-us-adults-went-without-dental-care
Lutfiyya MN, Gross AJ, Soffe B, Lipsky MS. Dental care utilization: examining the associations between health services deficits and not having a dental visit in past 12 months. BMC Public Health. 2019;19:265.
Brian Z, Weintraub JA. Oral health and COVID-19: increasing the need for prevention and access. Prev Chronic Dis. 2020;17:E82.
Quality Positioning System. National Quality Forum. Accessed October 4, 2020. https://www.qualityforum.org/QPS/QPSTool.aspx?m=1286&e=1



