Case and Commentary
Nov 2022
Peer-Reviewed

The Centers for Medicare and Medicaid Services mandates physicians’ responsibility for making sure that reimbursement for services physicians provide to patients is accurate and appropriate. Yet the shift of physician practice ownership to various employment models has amplified a dilemma. Physicians working as employees for some US health care companies might not know about services billed in their name, much less be able to review or contest when, which, to whom, or at what costs services were billed. Although such practices violate legal standards, many employed physicians are now accountable without transparency or agency. This commentary on a case considers this set of problems in contemporary billing and reimbursement structure and practice.
Dr L completed residency training 4 years ago and continues to pay down a balance of over $300 000 in loans used to finance college and medical education. Dr L practices medicine as an employee of Urban Health Care (UHC). Upon hire, Dr L was required to agree to grant UHC exclusive rights to bill for, collect, and retain reimbursement payments for Dr L’s professional services. The agreement does not indemnify Dr L for erroneous or fraudulent billing by UHC on Dr L’s behalf but does specify that UHC report speed and efficiency productivity targets called work relative value units (wRVUs) to Dr L, which inform Dr L’s performance reviews, incentives, and compensation.
Dr L recently noticed that salary deposits during the last few months do not seem to track with wRVU productivity reported by UHC. Dr L has also been asked by UHC billing staff, with increasing frequency during these months, to revise documentation of some services to some patients. Dr L asks other physician colleagues about their experiences with UHC’s billing practices and finds that several suspect that UHC is upcoding services they have provided to patients. Dr L learns that a few who have questioned UHC about this apparent irregularity have been terminated or had their hours reduced. One colleague expressed frustration, “We’re personally and professionally liable for the accuracy of bills sent in our names, yet we can’t question UHC without reprisal.” The Centers for Medicare and Medicaid Services (CMS) Medical Learning Network posts instructions for reporting suspected fraudulent or erroneous billing,1 but none of Dr L’s colleagues have yet done so.
Dr L wonders whether to contact CMS.
Society’s contract with clinicians requires that they provide complex health care services it cannot otherwise obtain and expects that they will be truthful,1 “competent, altruistic, and moral”2 in executing such services. Society accordingly grants health professions, especially medicine, status and privilege. In billing and claims submissions, specifically, the CMS Medicare Learning Network expresses another social contract expectation: “Medicare and other Federal health care programs rely on physicians’ medical judgment to treat patients with appropriate, medically necessary services, and to submit accurate claims for Medicare-covered health care items and services” (italics added).3 CMS regulations were written when most physicians practiced independently and exercised direct control over those who did their billing. Now, however, only one-third of physicians younger than 40 years of age own their labor.4 Clinician agency is generally confined to the point of service, and clinicians’ authority in claims matters has been surrendered to billing departments of health care organizations that employ them. Although the Physician Self-Referral Law names physicians, the regulations apply to all health care billing entities that have financial conflicts of interest.5 Despite significant changes to the health care system over the last 2 decades, the social contract remains in place, and we do well to remember that physicians “have a legitimate right to expect to work in a system which supports, not subverts, the traditional values of the healer and the professional.”2
Yet “the traditional values of … the professional” may not be supported in a system in which physicians are responsible for accurate Medicare claims submitted by their employers. According to the Office of Inspector General (OIG), US Department of Human Services:
Payers trust you, as a physician, to provide necessary, cost-effective, and quality care. You exert significant influence over what services your patients receive, you control the documentation describing what services they actually received, and your documentation serves as the basis for bills sent to insurers for services you provided. The Government’s payment of claims is generally based solely on your representations in the claims documents.
Because the Government invests so much trust in physicians on the front end, Congress provided powerful criminal, civil, and administrative enforcement tools for instances when unscrupulous providers abuse that trust…. When you submit a claim for services performed for a Medicare or Medicaid beneficiary, you are filing a bill with the Federal Government and certifying that you have earned the payment requested and complied with the billing requirements.6
Unless physicians have access to and time to review billing and claims data connected to their names, they cannot identify irregularity, error, or fraud for which they are legally liable.
This dogma implies that clinicians are not indemnified when erroneous or fraudulent claims are submitted to payers in their name by their employers. Yet, unless they own their practice, most physicians will rarely, if ever, see what is billed for or submitted for payment in their name. The result is an untenable situation in which physicians are responsible for the accuracy of billing—without transparency, agency, or authority over it—in what is known as the double-bind paradox.
The Code of Federal Regulations (CFR) carries the force and effect of federal law, mandating that, in circumstances in which clinicians assign billing responsibility to an employer or external vendor for reimbursable services rendered to patients insured by Medicare, they have unrestricted access to claims data submitted in their names.7 Yet health care organizations operating in competitive markets have staked out negotiated billing rates as “trade secrets,” even though “to date, no court has definitively held that negotiated rates between health care [organizations] and insurers constitute trade secrets.”8 In this environment, clinicians are unable to ascertain the downstream value of services they render because such knowledge might undermine their organizations’ competitive advantage in specific health care marketplaces. Clinicians are thus put in a double-bind: they have responsibility to ensure the accuracy of bills and claims submitted in their name, but their agency and authority to do so is undermined by de facto trade secret protection practices in everyday payment and billing operations in the US health care sector. This double-bind is worsened by improper billing and reprisals.
Improper billing. Perhaps the lack of transparency would be less of an ethical and financial problem were there not so many ways to bill and code improperly. Upcoding is one kind of improper billing practice that happens when the complexity of services rendered is exaggerated. Less common are overtly false claims that impose phantom charges (ie, for services never rendered), bills for services not clinically indicated, duplicate charges, unbundled charges for a group of services that are standardly billed together, or excessive quantities of itemizable charges.3,9 Unless physicians have access to and time to review billing and claims data connected to their names, they cannot identify irregularity, error, or fraud for which they are legally liable, according to 2021 CDC guidance.3
Reprisals and moral injury. Even with whistleblower and due process protections, physicians who have refused to sign off on charts of patients seen by another clinician for whom reimbursement rates are lower (eg, physician assistants) have reported retaliation (eg, losing hospital privileges or being removed from a clinical schedule).10 Minutes of a 2021 American College of Emergency Physicians Board meeting reported that physicians who speak up regarding inappropriate billing concerns face high risk of career-jeopardizing reprisals and only rarely resort to legal action against their employers.11 Literature on reprisal is sparse, however, so the extent of the problem is difficult to quantify. When professionals have responsibilities but work in environments in which they lack agency or control in executing their responsibilities, such as ensuring billing accuracy, they can suffer moral injury.12 This issue is of tremendous ethical importance. Improvement of systems that create such double-binds can be key to mitigating the widely documented and numerous harms of moral injury. In what follows, we canvass relevant information and options for clinicians faced with their employers’ nontransparent billing and claims practices.
Currently, CMS recommends that physicians address potential concerns about billing fraud or errors by following the OIG’s Health Care Fraud Self-Disclosure Protocol.3 The term self-disclosure might be an artifact from the era when physicians were directly responsible for their own billing. The Figure also lists other options delineated in the resource.
Figure. Centers for Medicare and Medicaid Services Recommendations to Address Suspected Personal or Organizational Billing Fraud
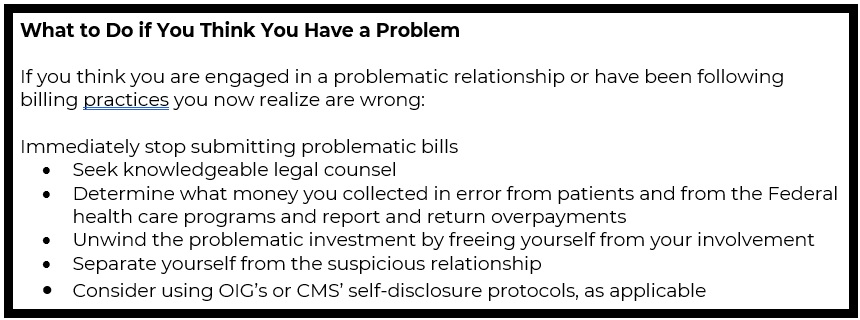
Reproduced from Medicare Learning Network.3
A clinician denied access to billing and claims information can notify the OIG or CMS. If a clinician’s organization does not comply with a clinician’s request for review access, it cannot receive Medicare claims reimbursement funds until the issue is resolved.13 Given the evidence of reprisals discussed above, self-disclosure to a federal agency requires courage, and clinicians should be aware that unemployment or reprisals are risks of disclosure.
In the case, Dr L’s and colleagues’ concerns about liability for irregular billing and claims submission done in their names by Urban Health Care is appropriate. In 2012, the OIG announced that physicians might be liable for false claims submitted by entities billing and receiving CMS payments in their names.14 Unfortunately, there is precedent for physician-owners of billing services being exposed to legal and financial liability (eg, fines) for false claims. In 1998, Emergency Physicians Billing Service (EPBS) and its leadership were found liable for false Medicare claims submitted to and collected by the billing company, which was owned by a physician. The federal government subsequently negotiated a settlement with 25 emergency physician practice groups that utilized EPBS to bill for services rendered by their clinicians.15 Although we do not know of a legal precedent for clinicians who rendered services (but were not owners) being held liable by a court of law for improper billing or claims practices, neither do we know of legal precedent absolving clinicians of liability for services improperly billed in their names.
In 2021, the American Medical Association (AMA) examined the issue of physician billing transparency in its Report of the Board of Trustees.16 First, the board recommended that that the AMA advocate for physicians to have “unrestricted access” to their billing records and associated patient medical records. Second, the board recommended that “the AMA adopt policy stating that, after termination of employment or other contractual arrangement, physicians should be given access to their billing records and associated medical records” so that they can defend themselves against any malpractice or other formal investigatory proceedings or claims brought against them. Third, the board recommended that the AMA “advocate for legislation or regulation to eliminate contractual language that bars or limits the treating physician’s access to his or her billing records and associated medical records, such as treating these records as trade secrets or proprietary.”16 Finally, the board cited policy advising that employers indemnify clinicians they employ from liability for erroneous, fraudulent, or otherwise inaccurate billing or claims submission when they are not at fault.
Additionally, federal, state, and organizational policies should promote billing transparency and at least be incentivized to (1) meet minimum requirements to share relevant proprietary information with clinician-employees who need to access billing and claims data submitted in their name or (2) transfer the full burden of billing and claims accuracy accountability to organizations.
Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 8th ed. Oxford University Press; 2019.
Medicare Learning Network. Medicare fraud & abuse: prevent, detect, report. Centers for Medicare and Medicaid Services; 2021. Accessed December 12, 2021. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/Fraud-Abuse-MLN4649244.pdf
Kane CK. Recent changes in physician practice arrangements: private practice dropped to less than 50 percent of physicians in 2020. American Medical Association; 2021. Accessed December 19, 2021. https://www.ama-assn.org/system/files/2021-05/2020-prp-physician-practice-arrangements.pdf
Definition of entity. US Department of Health and Human Services. December 31, 2020. Accessed June 24, 2022. https://www.hhs.gov/guidance/document/definition-entity
I. Physician relationships with payers. Office of Inspector General, US Department of Health and Human Services. Accessed December 20, 2021. https://oig.hhs.gov/compliance/physician-education/i-physician-relationships-with-payers/
Prohibition of reassignment claims by suppliers. 42 CFR §424.80 (1996).
Gudiksen KL, Chang SM, King JS. The secret of health care prices: why transparency is in the public interest. California Health Care Foundation; 2019. Accessed December 19, 2021. https://www.chcf.org/wp-content/uploads/2019/06/SecretHealthCarePrices.pdf
Tkacik M. Wall Street is pressing ER docs to fleece patients. Lever. October 27, 2021. Accessed July 28, 2022. https://www.levernews.com/er-organization-admits-to-the-evils-of-private-equity/
Action on 2020 resolutions. American College of Emergency Physicians. Accessed June 20, 2022. https://www.acep.org/what-we-believe/actions-on-council-resolutions/council/action-on-2020-resolutions/
Revocation of Right to Receive Assigned Benefits. 42 CFR §424.82 (2001).
OIG alerts physicians to exercise caution when reassigning their Medicare payments. News release. Office of Inspector General, US Department of Health and Human Services; February 8, 2012. Accessed June 20, 2022. https://oig.hhs.gov/compliance/alerts/guidance/20120208.pdf
Third-Party Billing Company Fraud: Assessing the Threat Posed to Medicare, Hearing Before the Subcommittee on Oversight and Investigations; Committee on Commerce, 106th Cong, 2nd Sess (2000). Accessed June 20, 2022. https://www.govinfo.gov/content/pkg/CHRG-106hhrg64027/html/CHRG-106hhrg64027.htm
Board of Trustees. Report 10-N-21: physician access to their medical and billing records (Resolution 226-A-19). American Medical Association; 2021. Accessed April 10, 2022. https://www.ama-assn.org/system/files/n21-handbook-addendum-ref-cmte-b.pdf



