State of the Art and Science
Apr 2025
Peer-Reviewed
Surgical research involving patients who are incarcerated is fraught with ethical, logistical, and practical questions. This article first considers important moments in the history of research with people who are incarcerated and suggests how they have contributed to evolution in human subject research ethics and regulation. This article also examines the problem of limited data about surgical disease burden and describes barriers to enrolling individuals who are incarcerated in surgical clinical trials, including study exclusion criteria and clinician-investigator bias. Finally, this article recommends strategies for balancing human research subject protections with the need for equitable enrollment in surgical clinical trials, especially later-phase trials in which benefit is more likely than in early-phase trials.
During the mid-20th century, people who were incarcerated were subjects of medical experimentation without their comprehensive understanding, especially in drug development trials, possibly in exchange for leniency or parole reevaluation.1,2,3,4,5,6 In response to Nazi human experimentation, the Nuremberg Code of 1947 established ethical standards for human experimentation, emphasizing informed consent, minimal suffering, and absence of coercion.7 Although never formally adopted by any international agency, the Nuremberg Code became the foundation for subsequent ethical standards.8
During the 1960s, the majority of non-federally funded phase 1 pharmaceutical trials utilized individuals who were incarcerated as primary subjects,9 raising significant concerns about exploitation.9,10,11 Federal regulations were finally enacted after headlines broke in 1972 about the 4 decades-long US Public Health Service Untreated Syphilis Study at Tuskegee, Alabama, and at other locations; revelations about these studies also led to the creation of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research.12,13 The commission noted that research in correctional settings presented problems related to coercion and autonomous consent.14 The National Commission’s report (published in 1976) led to the adoption in 1978 of regulations (45 CFR 46 Subpart C), which set specific protections for prisoners, including limited permissible research types, risk-benefit assessments, mandatory informed consent, and independent review by institutional review boards (IRBs), with the further requirement that an IRB member be a “prisoner” or a knowledgeable “prisoner representative.”15 Increased oversight of human subject research involving individuals who are incarcerated created a gradual shift from unethical research practices to the near exclusion of such individuals from potentially beneficial clinical research.3,16
The 1979 Belmont Report established ethical principles,17 codified in 1991 as the Common Rule, which requires IRB review and approval for human subject research.8,18 However, the additional safeguards of 45 CFR 46 Subpart C created regulatory barriers to the inclusion of individuals who are incarcerated in studies of carceral populations’ health that, over time, led to gaps in incarceration-related health data.19 Specialized IRB approvals and lengthy review and approval processes discourage researchers from enrolling individuals who are incarcerated, and the requirement to prespecify such participants discourages inclusion of those who are incarcerated during a study due to the need for additional IRB notifications.20 These challenges lead to flawed estimates of racial and ethnic health inequity, especially given the disproportionate incarceration of minority groups.21
Most national databases used for surgical outcomes research do not track incarceration status, which makes it difficult to extrapolate the surgical disease burden of individuals who are incarcerated.22,23,24 Beyond complex ethical and regulatory challenges, conducting large-scale studies on individuals who are incarcerated presents considerable logistical difficulties. These include data-sharing agreements with individual state and federal corrections departments as well as privately run facilities, each with its own restrictions. In many cases, these institutions might be reluctant to cooperate with research that could reveal data potentially reflecting negatively on their institutions, making access and collaboration even more difficult.
Some researchers have suggested using a “don’t screen, don’t exclude” approach, which allows patients who are incarcerated to be included in studies whose subjects are not limited to this patient population without additional screening to meet regulations.25 By not screening for incarceration status, researchers circumvent the extra regulatory requirements, which would otherwise delay the research process or necessitate special approvals. However, this shortcut also means that specific health issues related to incarceration might go unaddressed, thereby maintaining gaps in incarceration-related health data.
The only true data point regarding national surgical disease burden of individuals who are incarcerated came in the 1997 Bureau of Justice survey, which featured only one question regarding the need for surgery during incarceration and hence lacked specifics on diagnosis, procedures, or outcomes.26 Rather than addressing these gaps in future surveys, the most recent Bureau of Justice survey from 2016 opted to exclude all inquiries related to surgery among the incarcerated population.27 Without accurate data, advocacy to improve the standard of care proves more challenging.28
A few studies have attempted to estimate the local surgical disease burden of individuals who are incarcerated. In Florida’s largest county, nearly a quarter of inmate deaths were attributable to acute surgical diseases or traumatic injuries, yet only a third of individuals who died received surgical care.29 In California, the incidence of surgical disease in 2012-2014 among individuals who were incarcerated was comparable to the general population, but these individuals had high rates of complicated presentations and low rates of surgical intervention.30 These studies highlight the disparities in access to surgical care and outcomes for individuals who are incarcerated, underscoring the need for a national review to address these issues.
Focusing federally funded research on issues affecting individuals who are incarcerated is essential to ensure that they do not disproportionately bear research burdens without receiving corresponding benefits.31 While the necessary protections for ethical research involving this population are well established, the main challenge lies in securing the financial and personnel resources to implement these safeguards effectively. Doing so requires strong advocacy and political will, both of which are lacking due to the marginalized status of this population. We believe that the absence of consensus among researchers on the importance of improving health care and research in correctional settings leads policy makers to view these initiatives as controversial, resulting in a lower priority for funding and support.
One potential solution involves fostering partnerships among correctional facilities, academic institutions, and health care systems to create a framework whereby research is seamlessly integrated into the routine care of individuals who are incarcerated. This model could be adapted from research practices in veterans’ hospitals, where health care and clinical research are closely aligned. This approach would ensure ethically conducted studies that are directly relevant to the surgical needs of the incarcerated population.
Conducting surgical research involving individuals who are incarcerated presents several unique ethical challenges. The findings of one study suggest that the rate of health literacy among such individuals is low, which limits their understanding of procedures and treatment options, thereby complicating their ability to provide informed consent for research studies.32 Moreover, surgical choices among patients who are incarcerated might be influenced by external factors beyond a mere assessment of risks and benefits.33 For instance, individuals might opt for surgery or enroll in research studies primarily to avoid returning to prison. The presence of guards during surgical consultations restricts privacy and might intimidate patients, hindering open communication. Limited access to family members for support further deprives individuals who are incarcerated of valuable input during decision-making. These factors collectively impede their comprehension and ability to freely consent to surgical research participation.
Surgical research also necessitates postoperative assessments, but changes in imprisonment status can affect study eligibility. Individuals initially enrolled while incarcerated might be released or transferred, hindering follow-up appointments, while those previously ineligible to enroll might become eligible during follow-up. Researchers often exclude this population due to the challenges of meeting regulatory requirements, but this default exclusion raises costs and decreases the effectiveness of clinical trials, ultimately jeopardizing the interests of vulnerable individuals.25
In cases of trauma, “exception from informed consent” allows retrospective consent to be obtained from patients or their families. However, difficulties in contacting family members can result in the exclusion of individuals who are incarcerated from trials requiring immediate randomization and intervention, which might have been why such individuals were excluded from a trial of prehospital plasma administration.34 This exclusion might contribute to worse outcomes in patients who are incarcerated, but data on the topic remain scarce.
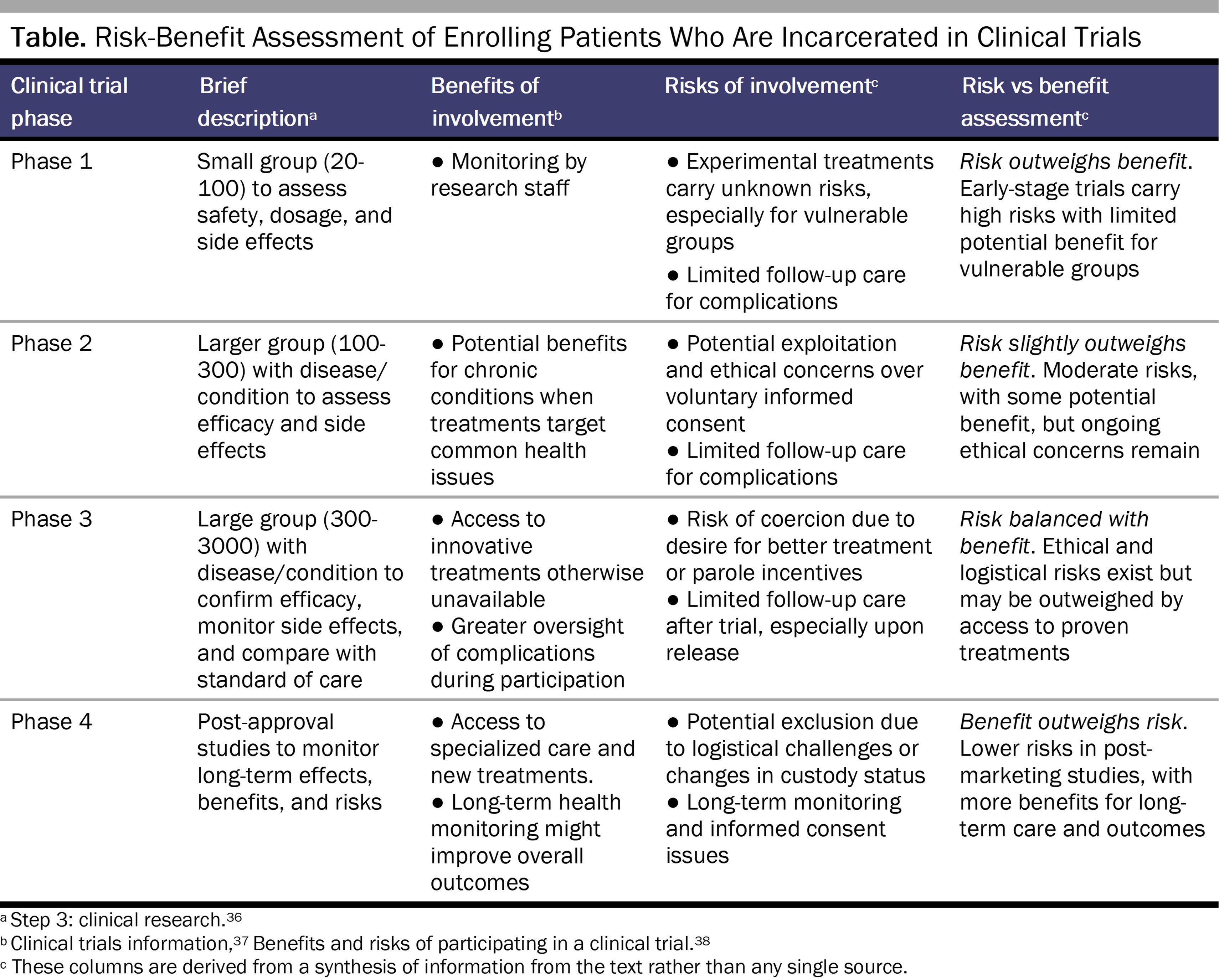
While research participation might provide patient-subjects’ access to specialized interventions, it also introduces unique risks at various stages of clinical trials (see Table). Early-phase studies can expose patient-subjects to undue risk without known benefits, while later-phase studies might offer novel treatments that have already been tested for safety. Inclusion of individuals who are incarcerated in studies not involving drug testing raises additional risk-benefit considerations. For example, enhanced recovery studies typically result in shorter hospital stay and improved outcomes,35 with the trade-off that the few patients who develop complications will do so after discharge, and these complications might go unaddressed in the correctional setting. Similarly, longitudinal studies offer the benefit of consistent health monitoring and care for chronic conditions, but, for patients who are incarcerated, they also can be the cause of disruptions in access to care due to changes in custody status.
For surgeons who act as both caregivers and researchers, when patients look to them for advice on the best treatment options, it is crucial to ensure shared decision-making in which a clear distinction is made between clinical advice and research-related information. The inherent limitations on autonomy within carceral settings are compounded by power imbalances between individuals who are incarcerated and surgeons, raising concerns about coercion during treatment selection.39
Surgical researchers must also studiously avoid undervaluing potentially beneficial studies due to preconceived biases regarding the ability of patients who are incarcerated to adhere to treatment regimens and follow-up protocols.40,41,42 These biases often originate from assumptions about the challenging correctional environment and concerns about patients’ access to ongoing medical care after the research is concluded. Additionally, there might be apprehension about the logistical complexities involved in coordinating follow-up appointments. This reluctance can perpetuate the underrepresentation of such individuals in surgical research, further exacerbating disparities in health care access and outcomes.
While attempting to prevent exploitation of individuals who are incarcerated, the extra federal protections currently in place limit their access to research benefits. Regulatory and logistical barriers to research perpetuate unaddressed gaps in access to surgical care. However, lowering these barriers risks compromising protections for patients experiencing incarceration, who are particularly vulnerable to exploitation and coercion. Despite limited data, regional studies have revealed surgical care disparities among such individuals, necessitating national attention. Ethical considerations for surgical researchers include ensuring informed consent, addressing power imbalances, and mitigating biases while prioritizing patient autonomy. In order to promote equity in surgical research, researchers must safeguard the rights of those who are incarcerated through ethically sound protocols while fostering trust and informed decision-making.
Advisory Committee on Human Radiation Experiments. Chapter 9: the Oregon and Washington experiments. In: Final Report of the Advisory Committee on Human Radiation Experiments. US Government Printing Office; 1995. Accessed February 7, 2025. https://ehss.energy.gov/ohre/roadmap/achre/chap9_2.html
Harcourt BE. Making willing bodies: manufacturing consent among prisoners and soldiers, creating human subjects, patriots, and everyday citizens—the University of Chicago malaria experiments on prisoners at Statesville Penitentiary. University of Chicago John M. Olin Program in Law and Economics working paper 544. February 2011. Revised May 2011. Accessed November 19, 2024. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=1758829
Harkness JM; The Green Committee. Nuremberg and the issue of wartime experiments on US prisoners. JAMA. 1996;276(20):1672-1675.
Advisory Committee on Human Radiation Experiments. Chapter 9: history of prison research regulation. In: Final Report of the Advisory Committee on Human Radiation Experiments. US Government Printing Office; 1995. Accessed February 7, 2025. https://ehss.energy.gov/ohre/roadmap/achre/chap9_4.html
Hornblum AM. NYC’s forgotten cancer scandal. New York Post. December 28, 2013. Accessed March 14, 2025. https://nypost.com/2013/12/28/nycs-forgotten-cancer-scandal/
Heller J. Syphilis victims in US study went untreated for 40 years. New York Times. July 26, 1972. Accessed November 15, 2024. https://www.nytimes.com/1972/07/26/archives/syphilis-victims-in-us-study-went-untreated-for-40-years-syphilis.html
National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. Report and Recommendations: Research Involving Prisoners. US Department of Health, Education, and Welfare; 1976.
Subpart C: additional protections pertaining to biomedical and behavioral research involving prisoners as subjects. Fed Regist. 1978;43(222):53655-53656.
Gostin LO, Vanchieri C, Pope A. The ethical framework for research involving prisoners. In: Gostin LO, Vanchieri C, Pope A, eds; Institute of Medicine. Ethical Considerations for Research Involving Prisoners. National Academies Press; 2007:chap 5.
Department of Health, Education, and Welfare; National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. The Belmont Report. Ethical principles and guidelines for the protection of human subjects of research. J Am Coll Dent. 2014;81(3):4-13.
Federal policy for the protection of human subjects; notices and rules. Fed Regist. 1991;56(117):28001-28032.
Greifinger R, ed. Public Health Behind Bars: From Prisons to Communities. Springer; 2007.
ACS National Surgical Quality Improvement Program. American College of Surgeons. Accessed May 24, 2024. https://www.facs.org/quality-programs/data-and-registries/acs-nsqip/
National cancer database. American College of Surgeons. Accessed May 24, 2024. https://www.facs.org/quality-programs/cancer-programs/national-cancer-database/
Healthcare Cost and Utilization Project (HCUP). Agency for Healthcare Research and Quality. May 2013. Reviewed July 2024. Accessed May 24, 2024. https://www.ahrq.gov/data/hcup/index.html
V1782: a health problem which required surgery? National Archive of Criminal Justice Data. Accessed May 23, 2024. https://www.icpsr.umich.edu/web/NACJD/studies/02598/datasets/0001/variables/V1782?archive=nacjd
Marushak LM, Bronson J, Alper M; Office of Justice Programs. Medical problems reported by prisoners: survey of prison inmates, 2016. US Department of Justice. June 2021. Accessed May 23, 2024. https://www.ojp.gov/library/publications/medical-problems-reported-prisoners-survey-prison-inmates-2016
Leech MM, Briggs A, Loehrer AP. Surgical diseases are common and complicated for criminal justice involved populations. J Surg Res. 2021;265:27-32.
Gostin LO, Vanchieri C, Pope A. Appendix B: the National Commission’s deliberations and findings. In: Gostin LO, Vanchieri C, Pope A, eds. Ethical Considerations for Research Involving Prisoners. National Academies Press; 2007:191-198.
Horkheimer S. Consent process best practices for special populations to reduce perceived pressure to participate in clinical trials. Clinical Researcher. July 19, 2021. Accessed October 1, 2024. https://acrpnet.org/2021/07/19/consent-process-best-practices-for-special-populations-to-reduce-perceived-pressure-to-participate-in-clinical-trials
Sperry JL, Guyette FX, Brown JB, et al; PAMPer Study Group. Prehospital plasma during air medical transport in trauma patients at risk for hemorrhagic shock. N Engl J Med. 2018;379(4):315-326.
Sauro KM, Smith C, Ibadin S, et al. Enhanced recovery after surgery guidelines and hospital length of stay, readmission, complications, and mortality: a meta-analysis of randomized clinical trials. JAMA Netw Open. 2024;7(6):e2417310.
Step 3: clinical research. US Food and Drug Administration. January 4, 2018. Accessed November 17, 2024. https://www.fda.gov/patients/drug-development-process/step-3-clinical-research
Clinical trials information. SCN2A Australia. Accessed November 17, 2024. https://scn2aaustralia.org/clinical-trials/
Benefits and risks of participating in a clinical trial. AbbVie Clinical Trials. Accessed November 17, 2024. https://www.abbvieclinicaltrials.com/resources/risks-and-benefits-of-participating-in-a-research-study/
Edge C, Stockley MR, Swabey ML, et al. Secondary care clinicians and staff have a key role in delivering equivalence of care for prisoners: a qualitative study of prisoners’ experiences. EClinicalMedicine. 2020;24:100416.
Frank JW, Wang EA, Nunez-Smith M, Lee H, Comfort M. Discrimination based on criminal record and healthcare utilization among men recently released from prison: a descriptive study. Health Justice. 2014;2(1):6.



