Medicine and Society
Nov 2024
Peer-Reviewed

Bereavement counseling is often offered as a referral following an adverse event or after identification of lingering grief. This article proposes the value of prospective bereavement counseling when a person can reasonably anticipate loss to support anticipatory grief and facilitate supportive continuous care planning for patients experiencing loss. This article positions bereavement counseling as care aimed at finding peace by offering a framework of dimensions of peace, opportunities to foster peace in clinically important moments, and guiding questions to facilitate this clinical outcome in health care settings.
The scope of bereavement counseling for peace need not be limited to death and end-of-life or palliative care. It also encompasses non-death loss, ambiguous loss, and anticipatory grief.1,2,3 For example, someone with dementia might have experienced numerous non-death losses—which also affect their loved ones—prior to experiencing the death of a loved one. The value of prospective bereavement counseling is its recognition that grief begins the moment that loss becomes a possibility, thereby offering health professionals multiple opportunities to foster peace in health care. This article discusses dimensions of peace in health care, opportunities to foster peace in clinically important moments, and questions clinicians can ask patients to help facilitate this clinical outcome.
Peace—understood as an ethos, a sentiment, a state, a feeling—is a challenging concept to operationalize, but, for the purposes of this article, it might be useful to view the concept of peace as encapsulating the following dimensions: an absence of conflict; an emotional and psychological state of being peaceful; an environment that represents peacefulness; a state of being in harmony (relational and systemic); and existential alignment of values with goals of care for quality of life.
Clinicians and health care workers likewise have multifaceted roles: as champions and co-creators of peacefulness; as mediators of conflicts; as promoters of peace as a goal of care; as co-collaborators with patients, their loved ones, and staff to achieve meaningful goals of care; and as educators and advocates working toward systemic shifts.
Here, the focus is on opportunities to foster peace in clinical moments, rather than focusing on specific patient populations.
The following represent clinically significant moments—critical and often emotionally charged—in which hope, trust, fragility, compassion, and uncertainty collide.
Noticing opportunities for peace. Sometimes a critical moment can be as simple as noticing and asking the patient, “Are you at peace?” This clinically important, open-ended question about what is important to the patient for holistic quality of life and care4,5,6,7 is more specific than asking, “How are you feeling?”
Breaking bad news.8,9,10 Having to break bad news is an unavoidable task when the situation is medically futile (ie, no reasonable benefit of treatment is possible) or when the risks of treatment significantly outweigh the benefits. The ethical duty to do no harm is often met with a tsunami of emotions upon the patient’s hearing words such as “I’m sorry, there nothing more to be done.” Objectively speaking, “nothing more” is not precisely accurate language—there are still things to be done in working toward different goals of care, although such language is sometimes necessary for the reality of the bad news to cognitively register for the patient. Bereavement counseling at this juncture would offer supportive management of shock and distress and facilitate the patient’s acceptance of the current reality.
Trust and therapeutic alliance.5,8,9,10,11 Moments that are ripe for shock, emotional magnitude, feelings of devastation, and an implied sense of defeat also give birth to loss and resulting grief. These are also critical moments for therapeutic alliance. How we handle these critical moments fosters clinical trust or distrust and peace or emotional dysregulation. Patients can be sensitive to perceived dismissal of their heightened emotions. Timely collaborative care with psychosocial health professionals can bolster trust and peace—like a cocoon in the midst of chaos.
Perceived failed intervention and recalibration.1,2,3,4,5,6,7,12,13,14 What is really happening in these moments is that the (original) goals of care have changed. Referrals to supportive counseling allow a platform for calibrating a readjustment of expectations. Such moments involve having to make an abrupt U-turn from the original goals to the prospective goals of care. When the patient sets quality-of-life care goals and receives multidisciplinary primary care soon after the loss, the fostering of peace is underway. Such multidisciplinary primary care might entail having a point-of-care person on the team to discuss issues that arise, plant seeds for adjustment to the new normal, and attend to anticipatory grief work and management of future regrets. Hospice and palliative care, oncology, and many specialties that routinely encounter loss already follow a dual-track approach: managing anticipation of death and maximizing quality of life.
System navigation and referrals for future care planning. Bereavement is not time or location dependent—the readiness to attend to loss and grief can be experienced some time after the precipitating event. The introduction of bereavement counseling and referrals allows resources to be placed within reach and to be taken up as and when needed. For most patients and loved ones, having these referrals in hand reduces the psychological burden of having to navigate systems on their own later.
The initial referrals will follow different care pathways based on whether death is anticipated, such as in palliative care, or due to an unexpected traumatic event. Similarly, referrals can be expected to differ based on who the referral is for (eg, adult vs child, patient vs loved one). At this stage, the goal is not so much “prescribing” peace as building a scaffold to support the transition to other avenues for continued healing.
Constructing clinical outcomes for existential aspects of healing is a challenge. However, as an exemplar, the bereavement counseling community took the existential concept of meaning-making4 (transforming sorrow into purpose) and created a constructivist therapy methodology, replete with skills, tools, and outcomes, and backed by research.
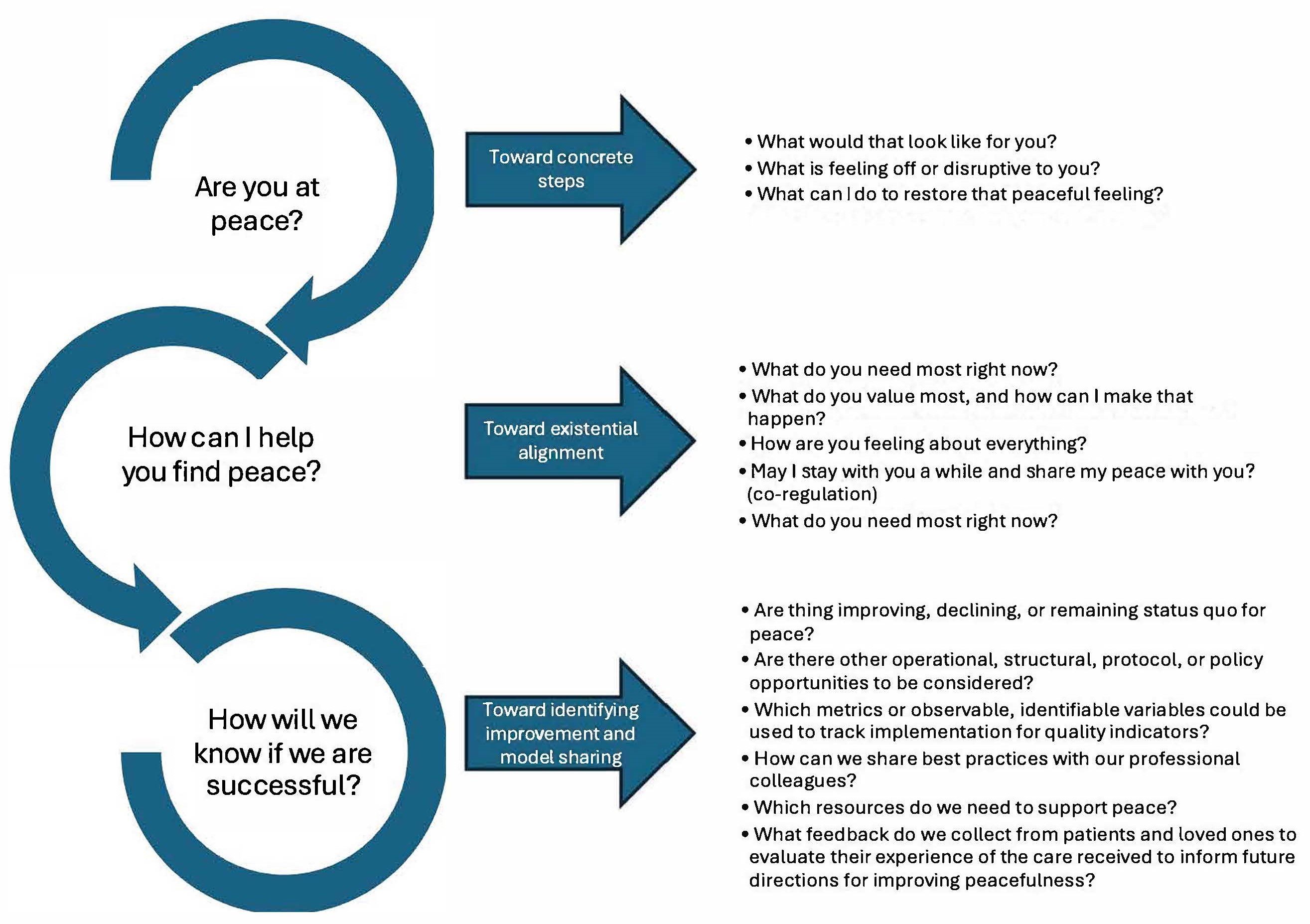
Treating peace as a constructed clinical outcome based on the proposed multifaceted dimensions would enable development of a curriculum for teaching compassionate clinical skills. Theoretical concepts like peace can be translated into goal-oriented questions in practice that target what the patient needs. In particular, health professionals can identify actionable steps during clinically important moments by eliciting input from patients about what is meaningful to them—their values, hopes, and expectations—to foster peace. Too many questions can become burdensome, however; so, to foster peace, health professionals must distill the complexity of peace into questions that elicit information relevant to actionable goals, as proposed in the Figure.
Figure. Guiding Questions for Translating Peace Into Goals of Clinical Practice
This approach offers several benefits. Inviting patient input fosters clinician beneficence, enhances patient dignity and autonomy, and can reduce potential harms arising from misalignment of goals of care and patient values. In a world focused on aggressive intervention, meeting the need for existential healing promotes both peace and effective resource allocation. Positive outcomes of health care that promotes peace include continuity of care, interdisciplinary collaboration, integration of evolving goals of care into the care plan, warm therapeutic referrals to community care for patients and their loved ones, and the perception by patients and their loved ones that clinicians have gone above and beyond what was expected. For clinicians, positive outcomes of health care that promotes peace include sharing of emotionally intensive clinical duties, creation of a buffer against compassion fatigue and vicarious trauma from continual exposure to loss, and acknowledgement of the toll of bearing witness. Peace in health care cannot ignore the needs of care professionals.
Although most of the foregoing discussion has been on clinically important moments as opportunities for fostering peace at the level of the patient-clinician relationship, the actual implementation of the framework hinges on operational support from institutions and systems that value the clinical significance of compassionate interventions.
The number of clinicians experiencing burnout, who are frustrated by their unrecognized and undercompensated labor in fostering peace and compassion, might compel scholars to refine outcomes metrics to champion a vision of peace. Specifically, some of the metrics important to health administrators, such as those related to quality improvement, staff burnout, patient satisfaction, and fundraising, might be relevant for fostering peace.
The promotion of peace in health care extends beyond a single definition of what peace is or ought to look like in multiple dimensions, just as health is more than the absence of illness or disease. Thus, the goal of peace is an affirmation of positive existence.
Harris DL, ed. Non-Death Loss and Grief: Context and Clinical Implications. Routledge; 2019.
Gorman E. Grief from a broader perspective: nonnite loss, ambiguous loss, and chronic sorrow. In: Harris DL, ed. Counting Our Losses: Reflecting on Change, Loss, and Transition in Everyday Life. Routledge; 2011:1-13.
Pauline B, Boss P. Ambiguous Loss: Learning to Live With Unresolved Grief. Harvard University Press; 2009.
Selman L, Speck P, Gysels M, et al. “Peace” and “life worthwhile” as measures of spiritual well-being in African palliative care: a mixed-methods study. Health Qual Life Outcomes. 2013;11(1):94.

