Original Research
Oct 2018

Background: Negative bias toward patients with obesity is an ethical challenge in patient care. Several interventions to mitigate medical students’ negative weight bias have been tried but none with an explicit focus on ethics. Here we describe first-year medical students’ attitudes toward obesity and our effort to improve their attitudes through an innovative ethics session embedded within the required course, “Obesity, Nutrition, and Behavior Change,” at Johns Hopkins University School of Medicine.
Methods: Precourse survey data were collected from 6 first-year cohorts (2012-2017). Before the ethics session, students take the Implicit Association Test (IAT) to measure implicit weight bias. During the session, students discuss their classmates’ personal struggles with weight, beliefs about causes of obesity, and the IAT results. They also watch and discuss video clips from the TV show House depicting negative weight bias. In addition, the 2017 cohort was surveyed 4 months later to evaluate the impact of different components of the session on students’ self-reported attitudes.
Results: All students responded to the precourse survey. Across cohorts, IAT results revealed that 70% of students held a thin preference, 18% were neutral and 12% held a fat preference. Forty-seven percent had personally struggled with weight loss. While most students thought obesity is a disease (89%) or behavioral (88%), 74% thought it results from ignorance, and 28% thought people with obesity are lazy. Among the 59 respondents to the follow-up survey, 30% reported improvement in their attitudes after the session. Over 40% thought it was useful to discuss students’ personal struggles with weight and the IAT and survey results, and over 70% thought the House video clips were useful.
Conclusions: Medical students have negative attitudes about obesity that are consistent over time. Providing opportunities for students to discuss their personal experiences and beliefs about obesity within an ethics framework and using popular media as a basis for discussion might improve their attitudes toward obesity.
Discriminatory attitudes toward patients with obesity is common among physicians—both among those who practice primary care and among those who specialize in treating obesity1-3—and medical students.4-8 Such negative attitudes—known as negative weight bias—adversely affect clinical practice and patient outcomes.9 Evidence indicates that negative weight bias can reduce access to surgery for obese patients,10 contribute to disrespectful attitudes among physicians,3 and decrease patient trust in physicians.11 Evidence also suggests that negative weight bias is associated with misperceptions about causes of obesity.12 Unfortunately, negatives attitudes, beliefs, and behaviors regarding obesity are perpetuated in patient care when medical students observe and copy the behaviors of physicians who model negative weight bias. Several studies indicate that personal experiences with weight also contribute to medical students’ negative attitudes and beliefs.13-15 Perhaps counterintuitively, evidence suggests that medical students who themselves have successively struggled with overweight or obesity are more likely to hold negative attitudes toward patients with obesity than their counterparts who have regained lost weight.13 Of particular concern is that medical students do not seem aware of their negative biases.16
Several interventions to address and mitigate negative weight bias among physicians and medical students have been developed and evaluated but with mixed results.17-26 With few exceptions,25,27 educational research designed to combat negative weight bias uses standard curricular interventions such as didactic presentations, role playing, and standardized patients.18-24,26 To our knowledge, none of these interventions has explicitly highlighted negative weight bias as an ethical challenge in caring for patients who struggle with obesity. In our first-year medical curriculum, we had an opportunity to incorporate an innovative ethics session within our required course, “Obesity, Nutrition, and Behavior Change.” Embedded in that course is a 90-minute small group session on ethics and professionalism in the care of patients with obesity. This session is designed to provide students with an opportunity to reflect on their own weight biases and explore the link between negative attitudes toward obesity and unethical or unprofessional behavior. Here, we describe attitudes and beliefs about weight among several cohorts of medical students and how our innovative ethics session addresses them.
Measures. Prior to the ethics session, students are required to take the online Implicit Association Test (IAT) on attitudes toward weight. The IAT measures the strength of associations between concepts (eg, people with obesity) and evaluations (eg, good, bad) or stereotypes (eg, lazy).28 Students then complete an anonymous online survey using the Blackboard platform in which they document their personal struggles with weight, their knowledge and beliefs about the causes of obesity, and their IAT results (see table 1).
| Yes/No Questions |
|---|
| Have you ever struggled with your weight? |
| Have you ever sought help with weight control issues? |
| Are any of your family members/close friends overweight? |
| Likert Scale Questionsa |
| Obesity is a disease |
| Obesity is behavioral (due to overeating) |
| Obesity results from poverty (inability to afford healthy food) |
| Obesity results from ignorance (lack of education/information about healthy eating) |
| Obese people are lazy/weak-willed |
| Obesity is primarily genetic/inherited |
| IAT Preferences |
| Strong/Moderate/Slight automatic preference for thin people |
| Little to no automatic preference between fat and thin people |
| Strong/Moderate/Slight automatic preference for fat people |
| a Questions take the form, “To what extent do you agree with the following statement?” Single-choice responses are “strongly agree,” “somewhat agree,” “somewhat disagree,” “strongly disagree.” |
Sample. Precourse data were collected from 6 first-year medical student cohorts of approximately 120 students each (range, 108 to 119) between 2012 and 2017. The class sizes were as follows: 2012 (N = 109), 2013 (N = 110), 2014 (N = 115), 2015 (N = 118), 2016 (N = 115), 2017 (N = 110). Each cohort was subdivided into 6 small groups of 20 students.
Intervention. Each small group is facilitated by an experienced faculty member with expertise in bioethics who shares his or her own experiences with weight to model self-disclosure. The facilitators are aware of the sensitive nature of this topic and reassure students that they do not have to share a personal story if they are uncomfortable doing so. At the beginning of the small group session, students are asked to discuss their own struggles with weight. The discussion of personal experiences is then followed by a review and discussion of their class’ and the previous class’ survey data including IAT results and beliefs about causes of obesity. Finally, students watch and discuss video clips from 2 episodes of the TV show House, each of which centers on a patient with obesity—one an adult male and one a preteen girl—in the order in which the group chooses. The episodes involve both senior physicians and residents. Facilitators then engage the students in discussion of particular ethics and professionalism themes depicted in the videos, such as (1) disrespectful behavior on the part of senior physicians and the tendency of residents and fellows—ie, younger people in the hierarchy—not to object when they hear their superiors make offensive comments, and sometimes even laugh, about patients with obesity; (2) disagreement among residents about the appropriateness of providing treatment to patients whom they think have personal responsibility for their health problems; (3) tendency toward victim blaming among some characters in the video clips; (4) questions about whether morbid obesity ought to be considered a disability; and (5) challenges physicians face when caring for patients they perceive as “difficult” because the patients’ preferences for care differ from what the physician believes is in the patients’ best interests.
An overall course evaluation is distributed every year, but only the most recent cohort of students were asked to assess the “ethics and professionalism” session. This last cohort was surveyed 4 months after the course to ascertain students’ impressions of the different components of the ethics session and the impact each component had on their self-reported attitudes toward obesity. This survey was conducted during another course that first-year students attend using the iClicker Student Response System.
This study was deemed exempt from Institutional Review Board review by Johns Hopkins University.
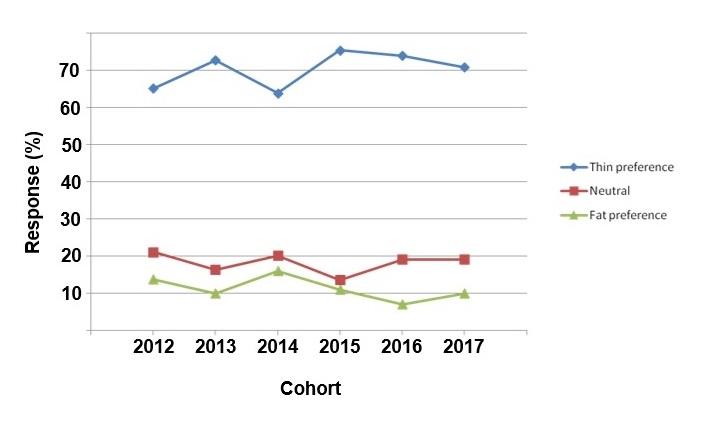
Pre-session survey. Because the IAT and the anonymous survey were required assignments for the group discussion on ethics and obesity, compliance was nearly 100% for each of the 6 cohorts. Fifty percent of the total respondents were male and 49% were female (1% declined to answer). Across cohorts, 70% of students had a thin preference (range, 64% to 74%), and only 11% of students had a fat preference (range, 7% to 16%). Eighteen percent of students had no preference (range, 14% to 21%). Over the 6 years of data collection, there were no obvious trends (see figure 1). Minor fluctuations, such as the dip in thin preference in 2014, were not thought to reflect a meaningful difference in attitudes.
Figure 1. IAT Results
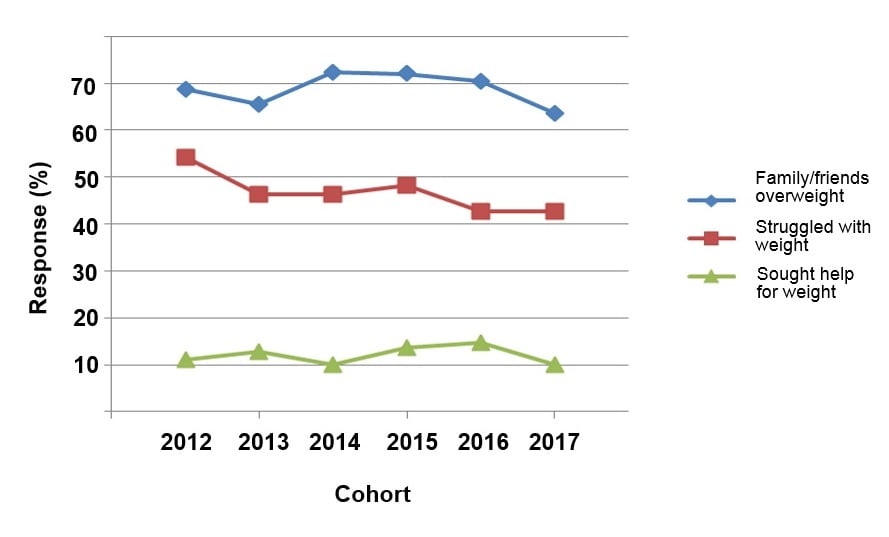
The survey taken by students after completing the IAT was designed to assess their own experiences with obesity and their beliefs about causes of obesity (see table 1). As shown in figure 2, weight problems were common. Across cohorts, 47% of students reported that they had at one time struggled with their weight (range, 43% to 54%), but only 12% had ever sought help with weight control issues (range, 10% to 15%). The majority of students (69%) reported that they had either family members or friends with obesity (range, 64% to 72%).
Figure 2. Personal Experience With Weight
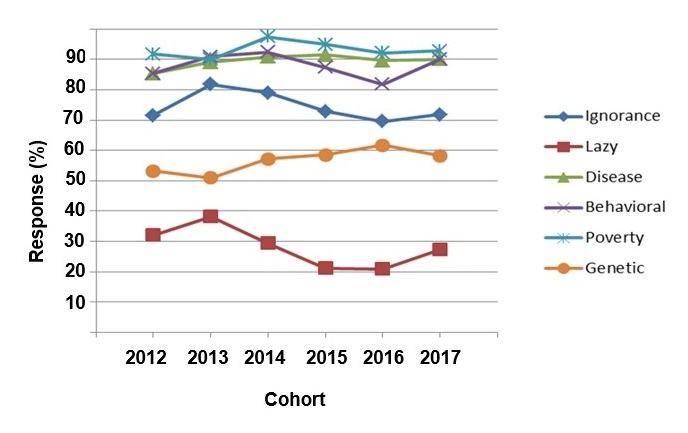
Students were also asked whether they agreed or disagreed with 6 statements regarding the etiology of obesity (see table 1, Likert scale questions). Across cohorts, 89% of students agreed or strongly agreed that obesity is a disease (range, 85% to 92%), and 89% of students believed it was behavioral (range, 82% to 92%). At the same time, over 90% of students agreed or strongly agreed that obesity results from poverty (range, 90% to 97%), and 57% believed that obesity is primarily genetic (range, 51% to 62%). Finally, 74% of students agreed or strongly agreed that ignorance contributes to obesity (range, 70% to 79%), and 28% had the opinion that people with obesity were lazy (range, 21% to 38%). While there were some fluctuations across cohorts, there was no strong trends (see figure 3).
Figure 3. Beliefs About Causes of Obesity
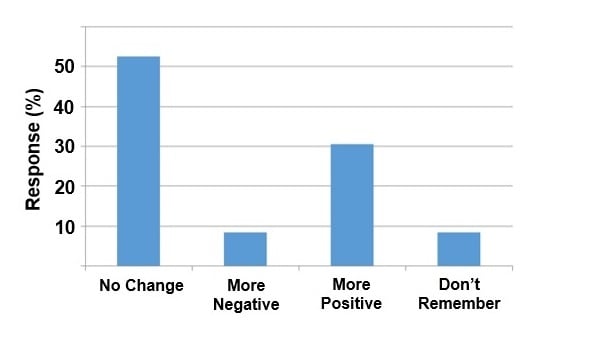
Follow-up survey. Approximately half of the 2017 cohort (n = 59) responded to the follow-up survey conducted in class using the iClicker system. Although 53% of respondents reported that their attitudes toward obesity did not change 4 months after the session, 30% reported positive change in their attitudes, and 10% reported more negative attitudes (see figure 4).
Figure 4. Self-Reported Changes in Attitudes Toward Obesity After Ethics Session
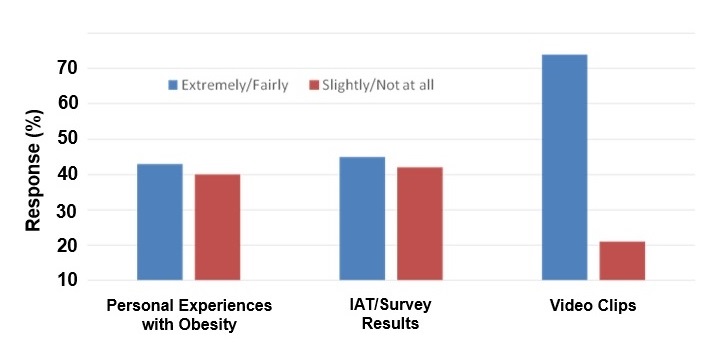
When asked what aspects of the session were particularly meaningful or useful, over 40% of all respondents thought discussing their personal struggles with weight (n = 24) and their class’ IAT and survey results (n = 26) was extremely or fairly useful (see figure 5). Over 70% of respondents thought the House video clips were extremely or fairly meaningful.
Figure 5. Students’ Perceptions of How Meaningful/Useful Was Each Component of the Ethics Session
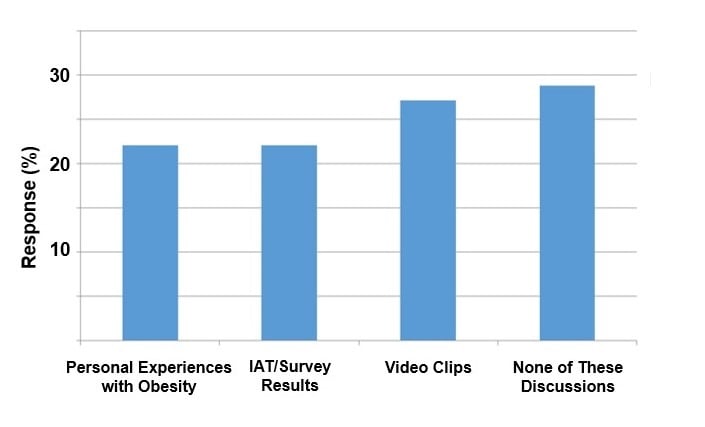
Consistent with these findings, more students reported that the video clips were influential in changing their attitudes toward obesity than discussions about their classmates’ personal struggles with weight or IAT and survey results (see figure 6).
Figure 6. Impressions of Which Discussion Influenced Attitude Change the Most
Our study contributes to the growing literature on negative weight bias among medical students in a few ways. First, our IAT results confirm the well-described phenomenon that medical students, like physicians, hold strong negative biases against obesity and patients with obesity.4-8 In addition, ours is the first study to demonstrate, at least at one institution, that attitudes about obesity and beliefs about causes of obesity remained stable over 6 cohorts of first-year medical students, despite increased attention to the obesity epidemic in the literature and mass media.
Although the vast majority of our students understood that obesity is a disease with a behavioral component, a significant minority believed that laziness and ignorance play a part. This troubling finding is consistent with national data indicating that a large percentage of medical students believes lack of willpower is an important contributor to obesity.12
Our findings also add to the growing body of literature on educational interventions aimed at mitigating negative weight bias.17-26 The session in which we explore students’ negative attitudes toward patients with obesity is innovative in a few ways. First, it explicitly links negative weight bias to ethics. Other educational interventions designed to influence student attitudes have taken place in the context of nutrition counseling and clinical management of patients with obesity.26 By integrating ethics and professionalism objectives within the nutrition course, students are encouraged to think about the ways in which discriminatory attitudes and behaviors toward patients with obesity are unethical and unprofessional. Second, students are given the opportunity to reflect on their own attitudes and those of their classmates in real time. By seeing that negative attitudes are common among their classmates, students may be better able to acknowledge their own negative attitudes. Third, our study is the first to describe the use of a popular television series about medical care to stimulate discussion and reflection about weight bias. One other study suggests that films can be useful in reducing explicit but not implicit weight bias among medical trainees.25 In that study, students watched documentary films that included expert commentary about weight prejudice in health care. By contrast, our pedagogic strategy enabled students to observe, analyze, and either identify with or reject the behavior of various physician-characters. Evidence indicates that socialization during medical school—including observation of physician behaviors—exerts a powerful influence on both explicit and implicit biases.15 In our study, students seemed to value the use of, and attribute some level of attitude change to, innovative teaching tools like television and film. This finding is supported by evidence that television and movies can be effective in fostering humanistic, compassionate, and person-centered orientations in medical students.29
Our study has important limitations. We only collected data from first-year medical students at one medical school. One study of negative bias among medical students has been conducted on a nationally representative sample of medical students, albeit at only one point in time.5 The degree to which negative attitudes toward patients with obesity remain stable across student cohorts may vary across medical schools in other geographic locations or with admissions criteria and curricula that place a higher value on eliminating negative bias. Second, the limitations of Blackboard software precluded us from examining the relationships between respondents’ personal struggles with weight, their knowledge about obesity, their attitudes toward patients with obesity, and their demographic characteristics. Therefore, we cannot replicate the associations other studies of medical students have found between personal experiences with obesity, beliefs about the causes of obesity, and negative weight bias.13-16 Finally, our study was not specifically designed to evaluate the “ethics and professionalism” session and its impact on students’ attitudes toward obesity. If we had set out to do such a study, we would have collected postsession data from all cohorts immediately following the session and would have used more objective attitudinal measures than self-report.
These limitations, however, pave the path for innovative future research. We know that adequate nutrition education is lacking in US medical schools, despite recommendations from educators and professional societies, and that very few schools address weight bias.30-32 Providing students with an opportunity to discuss their personal experiences and beliefs about obesity within an ethics framework and using popular media as a basis for discussion might improve their attitudes. Future research should test these propositions in a prospective, systematic, and more representative study and explore the impact on weight prejudice of other humanities-oriented interventions such as literature, art, and written reflection.33 As medical schools grow increasingly attuned to students’ moral and professional development, consideration should be given to combining nutrition and ethics curricula in novel ways to mitigate negative weight bias among students.
Pantenburg B, Sikorski C, Luppa M, et al. Medical students’ attitudes towards overweight and obesity. PLoS One. 2012;7(11). doi:10.1371/journal.pone.0048113.
Andrade AD, Ruiz JG, Mintzer MJ, et al. Medical students’ attitudes toward obese patient avatars of different skin color. Stud Health Technol Inform. 2012;173:23-29.
Pillutla V, Maslen H, Savulescu J. Rationing elective surgery for smokers and obese patients: responsibility or prognosis? BMC Med Ethics. 2018;19:28. doi:10.1186/s12910-018-0272-7.
Miller DP Jr, Spangler JG, Vitolins MZ, et al. Are medical students aware of their anti-obesity bias? Acad Med. 2013;88(7):978-982.
Kushner RF, Zeiss DM, Feinglass JM, Yelen M. An obesity educational intervention for medical students addressing weight bias and communication skills using standardized patients. BMC Med Educ. 2014;14(1):53. doi:10.1186/1472-6920-14-53.
Harvard University. Project Implicit. https://implicit.harvard.edu/implicit. Published 2011. Accessed 30 April 2018.



