Health Law
Apr 2015

People are always looking for a single magic bullet that will totally change everything. There is no single magic bullet.
–Temple Grandin, autism reform advocate [1]
“Economic burden,” “regulatory maze,” and “lawyer’s paradise” are a sample of the epithets lobbed against the Americans with Disabilities Act (ADA) before it was signed into law in 1990 [2-4]. A quarter-century later, similar doomsday-like forecasts plague efforts to assist disenfranchised people with autism spectrum disorder (ASD), a condition that has since skyrocketed in prevalence [5-7]. Though regulations to assist those with ASD have moved to the forefront of state and federal policy discussions, ASD initiatives compete with other pressing health care spending concerns to gain access to a finite amount of governmental resources. Satisfying the demand for high-quality, cost-effective ASD care requires well-researched, well-defined state and federal spending parameters that emphasize long-term patient outcomes as well as sustainable net gains.
In light of a growing national awareness about ASD in children, the latest regulations from the Centers for Medicare and Medicaid Services (CMS) have added applied behavior analysis (ABA) to the list of treatment modalities covered by Medicaid for those under age 21 [8]. Now, physicians and health care professionals in all states can code ABA as federally mandated early and periodic screening, diagnostic, and treatment services (EPSDT) [8, 9]. Many state legislatures have enacted autism-specific insurance mandates that require for-profit, commercial, health maintenance organization (HMO), and nonprofit health insurance companies regulated by the state to pay for medically necessary and evidence-based autism treatments for certain groups of people [10-37]. Of course, some state laws set forth more comprehensive and clearly defined eligibility and coverage criteria than others. Most state mandates require coverage until the patient reaches a certain age, usually in the range of 19 through 22 years [10-38].
Some forward-thinking policymakers are taking reform one step further by enacting groundbreaking ASD-specific Medicaid programs that not only expand the scope of services available to Medicaid beneficiaries with ASD, but also offer services like respite care and limited reimbursements to family member caretakers [8, 39]. New federal laws create financial incentives for direct care by the family members of those with ASD by encouraging states to provide services to benefit the caregivers [8, 39]. Until recently, the notion of third parties—people other than the patient—receiving dollars from a patient’s private or governmental insurance program was a rarity. During the last decade, the most common form of spending on third-party welfare was generally for mental health and grief counseling for the immediate family members of hospice patients [40-44]. This coverage of education, counseling, and medical social services acknowledges that one family member’s health concerns can impact the well-being of the rest of the family [40].
The practice of valuing family members as part of a patient’s unit of care can be applied to long-term care for ASD. After all, family member caretakers are, oftentimes, responsible for the day-to-day care of patients with ASD. For the good of families, patients, and the country’s fiscal situation, we must continue to encourage family member involvement in caring for people with ASD, promote home or community-based care and, as appropriate, reduce reliance on overburdened Medicaid state plan and waiver programs. Since family members are often primary caregivers for people with ASD (particularly young children), it follows that, when a family caregiver’s mental or physical health declines, patient outcomes can suffer. Maintaining a focus on clearly defined reimbursements, ASD-specific education, training, and other meaningful benefits for family member caregivers can increase families’ direct involvement in ASD-specific care and, in turn, improve patient outcomes. Moreover, it can lower overall health care costs and help state and federal policymakers to balance competing budget expenditure priorities in the long term.
To gain a more comprehensive view of the overarching economic impact of ASD, we must first acknowledge that the dynamics of ASD-related actions and omissions in health care reform cannot reasonably be considered in an economic vacuum. The predominant hurdle facing policymakers who wish to implement ASD insurance reforms is a dearth of overall resources. The country’s fiscal situation is straitened primarily by three factors: (1) health care spending disproportional to the economy’s annual output, or gross domestic product (GDP); (2) rapid growth in the population of elderly people (which drives up health care spending, particularly for long-term care of those covered by Medicare and Medicaid); and (3) large state and federal budget deficits. The Congressional Budget Office (CBO) identifies health care spending growth as one of the core fiscal challenges facing our government [45]. If current trends hold, by 2050 government health care spending will claim one-third of the GDP [46]. The US Census Bureau estimates that, in the not-too-distant future, the number of elderly people in the US will be twice what it is now [47]. If current government spending practices remain essentially unchanged, the federal debt held by the public will exceed 100 percent of the GDP in just 25 years [46]. According to government researchers, the federal government will have to ultimately raise taxes, cut spending for benefits and services, or both to create sustainable, long-term financing plans [48]. Some might argue that the scarcity of resources for ASD-specific reforms, on its face, suggests a solution that solely reduces services and coverage. Yet specific, pinpointed spending devoted to early intervention and support for caregivers today will, in fact, lower costs in the long run. We can empower patients and their families to improve and maintain their health now so these same people do not require far more costly health care services later in life.
ASD insurance reforms often impact the scope of services required for all health insurance plan types available to people with ASD. These include government-subsidized plans in the state marketplace exchanges, the Children’s Health Insurance Program (CHIP), Medicaid, private health insurance, and self-funded programs. Since 2001, ASD insurance reform laws have been enacted either by legislation or administrative mandates in 39 states and the District of Columbia (see figure 1) [49-51]. These laws provide varying degrees of services to people with ASD and are often limited by age classifications and “maximum benefit amounts” (annual payment limits for covered services). Nearly half of children and youth with ASD have private health insurance coverage [52], one-third of all children and youth with ASD are covered by Medicaid and CHIP, and 17.7 percent are dual enrollees in governmental and private health insurance (see figure 2) [52]. Eighty-six percent of Americans live in a state with some ASD reform statutes or administrative regulations, but more than 54 million people live in states without explicit ASD-specific state laws that clarify the breadth, length, and eligibility details for coverage beyond the federally mandated baselines for ASD care (see figure 3) [52, 53].
Figure 1. Enactments of State Autism Laws by Year (2001-2014)
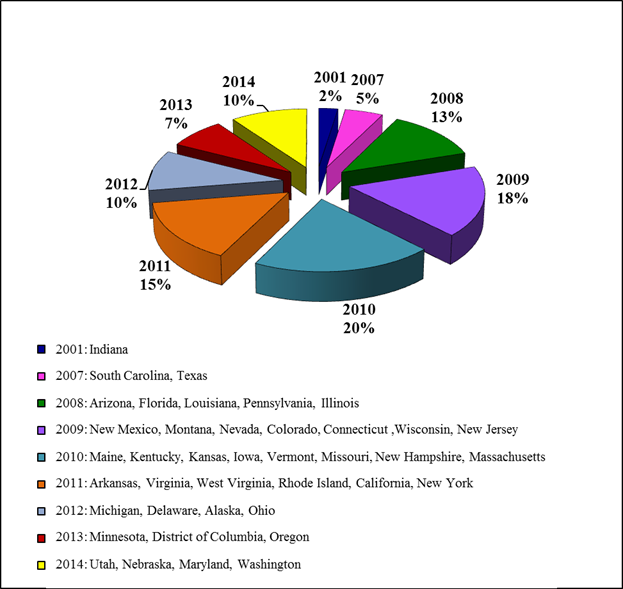
Data include autism spectrum disorder reforms enacted either by statute or by administrative mandate [49-51].
Figure 2. Health Insurance Coverage for Children and Youth With Autism Spectrum Disorder and Other Special Health Care Needs [52]
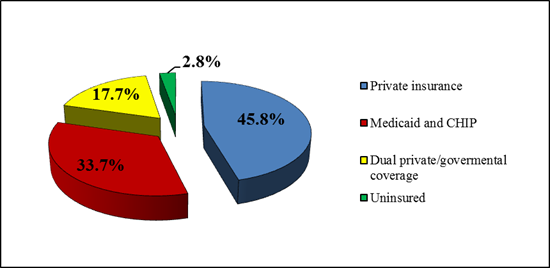
Figure 3. Autism Insurance Reform and the US Population
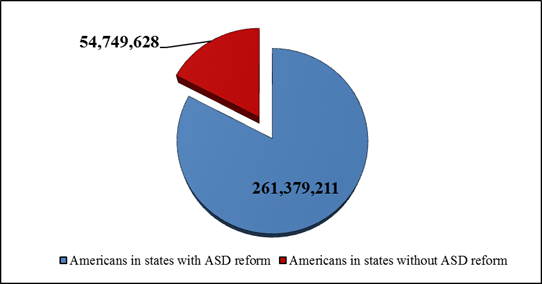
Autism spectrum disorder (ASD) insurance reform includes any ASD-specific insurance reform law that has been enacted either by legislation or by administrative mandate in 39 states and the District of Columbia [52, 53].
Under the Individuals with Disabilities Education Act (IDEA), states must provide early ASD intervention treatment to certain children under age three even if they do not have a formal ASD diagnosis [54]. Children must be deemed “at risk” for developmental delays to be eligible for these services [55]. Recognizing that those with ASD are likely to respond best to medical interventions performed while they are young, ASD reform advocates have long balked at health insurance providers’ annual caps on the number of covered office visits [55]. Once patients exhaust the limited number of yearly treatments or office visits covered by their carriers, they and their families are often forced to rely on counselors and special needs programs within their state’s public school system for ongoing ASD-specific care. In an effort to provide more progressive and effective ASD care, some states have eliminated annual caps and included a catchall provision in their statutes requiring that patients with ASD receive all medically necessary and evidence-based care as determined by a licensed physician [10, 14, 31, 34-38, 56-60. To date, only Delaware and Arkansas specifically list medical equipment as a covered item for patients with ASD [10, 56]. While certain state laws expand covered mental health care beyond that received from psychiatrists and psychologists, only a few include specific mention of which services from other specialists like certified nurse practitioners or clinical social workers are covered [14, 59, 60].
Enacted in 1965, Medicaid offers government funding to help eligible populations with limited resources receive medical care [61, 62]. Covered demographics include people with disabilities who qualify for the Supplemental Security Income (SSI) program [63, 64]. Someone seeking Medicaid coverage of ASD-related services must meet certain income requirements and be registered as a person with a Social Security Administration-classified disability [64]. Medicaid eligibility rules and covered services vary from state to state because, though eligibility and the scope of services covered are based on federal requirements, federal law grants states considerable leeway to decide how best to operate their programs. States can elect to expand health care services and coverage beyond the federally set minimum requirements. Medicaid includes long-term care services provided at home, such as visiting nurses and assistance with the activities of daily living [65]. Unlike Medicare, Medicaid is more likely to pay for custodial care at home or in a skilled nursing facility [65].
In July 2014, autism advocates won a hard-fought battle to include applied behavior analysis (ABA) as a Medicaid-covered treatment option for those under age 21. CMS confirmed that all states must offer ABA as one of the treatment modalities for eligible people under Medicaid’s comprehensive and preventative EPSDT provision [8]. This was a significant victory, since 51 percent of children or youth with ASD are covered by either Medicaid, CHIP, or a combination of private and public health insurance [52, 66].
The rub is that ASD patients under 21 and on Medicaid can only obtain ABA services after “medical necessity”—the scope of which can vary from provider to provider and state to state—is shown [67]. In September 2014, CMS clarified its earlier statements about ASD-specific coverage, stating that states are obligated to provide all “medically necessary services available for the treatment of ASD” to Medicaid beneficiaries from birth to age 21 [9]. Baseline federal considerations for satisfying EPSDT’s requirement that states provide medically necessary services include: (1) assessing and identifying problems early; (2) checking children’s health at periodic, age-appropriate intervals; (3) providing physical, mental, developmental, dental, hearing, vision, and other screening tests to detect potential problems; (4) performing diagnostic tests to follow up when a risk is identified; and (5) treatment to control, correct, or reduce identified health problems [67]. To determine the required frequency for periodic screening of patients on Medicaid, clinicians must apply “reasonable standards of medical practice” for the particular patient [67].
Medicaid programs can pay for home and community-based services (HCBS) for people with ASD through the state plan as well as through Medicaid waivers [68]. Historically, Medicaid reimbursement standards favored state programs that covered people with disabilities in institutions but not people with the same disabilities living at home [68]. This is sometimes referred to as Medicaid’s “institutional bias” [69]. It remains a state’s choice whether to expand HCBS coverage to patients up to age 21 using Medicaid waivers, which “waive” the general requirement that Medicaid services be provided in an institution and allow the recipient to receive comparable services in a home or community setting [68, 70, 71].
Thirty-two states currently offer ASD-specific Medicaid waivers (often called “1915(c)” waivers) [70-72]. Standard services include but are not limited to case management, homemaker or home health services, personal care, adult day health services, habilitation (to help a person learn, improve, or keep skills for daily living), and respite care. States can also propose other types of services that may assist in diverting and/or transitioning patients from institutional settings into their homes and communities [70]. As the National Council of Disabilities (NDC) explains, the evidence overwhelmingly suggests that “people with disabilities living in small family-scale settings that they control are more likely to experience positive personal outcomes” than people living in larger settings that they do not control [72]. According to the NDC and National Core Indicators (NCI) studies, people with disabilities who live with a biological family caregiver (or a host family) generally have better decision-making abilities, personal well-being, and satisfaction than those living in an agency setting [72, 73].
Although HCBS Medicaid waiver programs can offer much-needed assistance, they are rife with problems. Many of the states that offer them cap the number of people who can receive waivers, leading to long government waiting lists. Also, the Medicaid waivers generally cannot enable reimbursement of guardians, parents, or spouses of waiver recipients for providing service, although county waiver agencies may choose to reimburse those persons using other funding sources [74]. Due to tremendous waiting lists in most states, a patient is unlikely to get a Medicaid waiver during the period immediately following diagnosis, when medical interventions would be most effective.
The Supreme Court has acknowledged that the care of people with disabilities is the “special obligation” of government [75]. Despite this ruling, as indicated above, federal, state, and municipal governments are struggling to adequately address their populations’ ASD-related needs because of stretched state budgets, the exploding costs of health care, and increasing demands for health care services (particularly from the aging Baby Boomer generation and previously uninsured people who are now covered under the Affordable Care Act). Many people with ASD have difficulty obtaining adequate health insurance, and interventions offered through private clinicians and other out-of-pocket service providers can place an enormous financial burden on families.
So, in December 2014, Congress attempted to mitigate some of these concerns by passing the Achieving a Better Life Experience (ABLE) Act, which recognizes that living with a disability is often associated with added costs [76]. Congress amended the federal tax code to allow people with disabilities (with an age of onset up to 26 years old) and their families to create tax-exempt savings accounts modeled on tax-free college savings accounts [76]. The funds can be used for quality-of-life expenses other than health care, such as education, housing, transportation, employment training, community-based support services, assistive technology, and financial planning [76]. Because ABLE savings accounts are not considered legal assets, they encourage greater financial independence for people with disabilities without affecting their eligibility for supplemental security income (SSI), Medicaid, or other critical public benefits.
In August 2014, Congress passed the Autism Collaboration, Accountability, Research, Education, and Support Act (Autism CARES), which focuses on autism education, early detection, and intervention and includes funding to “provide evidence-based interventions for children with autism spectrum disorder” [39]. Under the law, Congress is obligated to pay only for these activities “subject to the availability of appropriations” [39]. The statute allows the federal government to make assistance provisions conditional on the state’s creation of a lead agency to coordinate ASD education, early detection, and intervention initiatives [39]. In addition, the statute specifically requires lead agencies to assist “family members, guardians, advocates, or authorized representatives” by providing “comprehensive culturally competent” information about state and local ASD services in the form of useful phone numbers, websites, or mailed literature [39]. Interestingly, the statute specifically mentions that available supports “may include respite care for caregivers of individuals with an autism spectrum disorder” [39].
Until recently, federal laws have carved out only a small number of instances in which government-sponsored health insurance must pay for services provided to a patient’s family member. For instance, Medicaid will cover comprehensive bereavement services for families of hospice patients, including services in home and community-based settings [10, 11, 77]. CMS has confirmed that the government prioritizes meeting the physical, emotional, and spiritual needs of both the patient and the patient’s family in an effort to minimize the “stress and problems that arise from the terminal illness [and] related conditions” [78]. Views are shifting to recognize family member caretakers as part of the patient’s unit of care. Policymakers are expanding this line of thought to ASD in recognition that ASD diagnoses can affect an entire family, not just the patient.
To enable family members to better assist their loved ones with ASD and become part of the government’s cost savings solution, states must prioritize caretaker education and training mechanisms to assist with patients’ and families’ physical, emotional, and spiritual needs. Common sense dictates that able family caregivers can help prevent health declines, which are both medically devastating and terribly expensive. Caring for patients with ASD and their caregivers not only improves the development and long-term health of the patients, but also decreases their institutionalization and stress-based health complications for family member caretakers. These actions will, in turn, decrease overall health care spending and reliance on government-sponsored programs.
To encourage long-term savings on lifelong care for patients with ASD, state and federal policies must continue to prioritize early diagnosis and intervention spending now to avoid more costly services for diminished patient outcomes in the future. The Centers for Disease Control (CDC) state that the unwanted symptoms of ASD, particularly in their early stages, can be mitigated and the earlier a child can receive the proper treatment, the better [55]. Rationing medically necessary and evidence-based treatments when children are young (and most likely to benefit from intensive therapy) is a poor long-term strategy for managing health care costs. Laws that limit a child’s access to health insurance coverage for ASD treatments now will engender substantially higher costs for care in the future. Costs will be substantially lowered when children with ASD can benefit from treatments and, as adults, function independently or semi-independently in a home or community setting.
Common sense further dictates that, if family members are brought into the fold of the patient care unit—educated, trained, and medically supported to avoid their own health declines—they can help to mitigate the need for more costly intensive therapies (including institutionalization) for their loved ones with ASD. The National Research Council states: “Education, both directly of children, and of parents…is currently the primary form of treatment for autistic spectrum disorders” (emphasis added) [79]. Without equivocation, dollars spent today to educate, support, and empower family member caregivers—those in the front lines of the fight to improve the well-being of people with ASD—will yield durable medical and economic benefits.
We can continue to build on this knowledge with meaningful ASD reforms at the federal, state, and country levels by focusing on four primary goals:
Despite remarkable advances in medical science surrounding ASD, the amount of public money to devote to ASD care remains controversial [80]. Two fundamental and weighty questions persist: (1) where is government money best spent to accomplish this goal and (2) how much spending is necessary? To create fiscally responsible action plans that focus on achieving and maintaining sustainable, long-term results, we must construct meaningful data sets by melding evidence-based research from multiple disciplines including medicine, mental health, economics, accounting, sociology, policy, and law. Until silos are broken down and professionals in many disciplines are willing to work together in ways they perhaps never have before, ASD will unduly challenge the lives of patients and those who love and care for them.
Autism Research Institute. Advocacy & resources: interview with Dr. Temple Grandin. http://www.autism.com/advocacy_grandin_interview. Accessed March 2, 2015.
Holmes SA. Rights bill for disabled is sent to Bush. New York Times. July 14, 1990. http://www.nytimes.com/1990/07/14/us/rights-bill-for-disabled-is-sent-to-bush.html. Accessed March 2, 2015.
Ball W. Should the Senate approve the Americans with Disabilities Act of 1989? Congressional Digest. 1989;68(12):309.
Rasky SF. Senate adopts sweeping measure to protect rights of the disabled. New York Times. September 8, 1989. http://www.nytimes.com/1989/09/08/us/senate-adopts-sweeping-measure-to-protect-rights-of-the-disabled.html. Accessed March 2, 2015.
Autism and Developmental Disabilities Monitoring Network Surveillance Year 2006 Principal Investigators; Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorders—Autism and Developmental Disabilities Monitoring Network, United States, 2006. MMWR Surveill Summ. 2009;58(10):1-20.
Centers for Disease Control and Prevention. 10 things to know about new autism data. http://www.cdc.gov/features/dsautismdata/. March 31, 2014. Accessed March 2, 2015.
Autism Speaks. Facts about autism. http://www.autismspeaks.org/what-autism/facts-about-autism. Accessed March 2, 2015.
Mann C. Clarification of Medicaid coverage of services to children with autism. Centers for Medicare and Medicaid Services. http://www.medicaid.gov/Federal-Policy-Guidance/Downloads/CIB-07-07-14.pdf. Accessed March 2, 2015.
Centers for Medicare and Medicaid Services. Medicaid and CHIP FAQs: services to address autism. http://medicaid.gov/federal-policy-guidance/downloads/faq-09-24-2014.pdf. September 2014. Accessed March 2, 2015.
Del Code Ann tit 18, sec 3361.
Fla Stat Ann sec 627.6686.
Ill Comp Stat ch 215, sec 5/356z.14.
Iowa Code sec 514C.28.
Kan Stat Ann sec 75-6524.
Kan Stat Ann sec 40-2,103.
Kan Stat Ann sec 40-19C09.
Ky Rev Stat sec 304.17A-142.
Ky Rev Stat sec 304.17A-143.
La Rev Stat Ann sec 22-1050.
2012 Mich Pub Acts, Act 99.
2012 Mich Pub Acts, Act 100.
2012 Mich Pub Acts, Act 101.
Minn Stat sec 62A-3094.
Mont Code Ann sec 33-22-515.
Neb Rev Stat sec 44-7,106.
Neb Rev Stat sec 689A.0435.
NM Stat Ann sec 59A-22-49.
NM Stat Ann sec 59A-23-7.9.
NM Stat Ann sec 59A-46-50.
NM Stat Ann sec 59A-47-45.
Or Rev Stat sec 743A.190.
Pa Cons Stat tit 40, sec 764h.
RI Gen Laws sec 20.11.
SC Code Ann sec 38-71-280.
W Va Code sec 5-16B-6e.
W Va Code sec 33-16-3v.
W Va Code sec 33-24-7k.
W Va Code sec 33-25A-8j.
Pub Law No. 113-157, 128 stat 1831.
Centers for Medicare and Medicaid Services. Medicare Hospice Benefits. http://www.medicare.gov/Pubs/pdf/02154.pdf. Accessed February 28, 2015.
Social Security Act sec 1905(a)(4)(B), 42 USC sec 1396d(a)(4B) (2012).
Public Health Service Act sec 399CC(g), Autism education, early detection and intervention, 42 USC sec 280i-1(a) (2012).
Social Security Act sec 1861(dd)(2), 42 USC section 1395x (2012).
Social Security Act sec 1867, 42 USC sec 1395(dd)(2) (2012).
Congressional Budget Office. Health care. https://www.cbo.gov/topics/health-care. Accessed February 18, 2015.
Congressional Budget Office. The 2014 Long-Term Budget Outlook. Congressional Budget Office; 2014:1. https://www.cbo.gov/sites/default/files/45471-Long-TermBudgetOutlook_7-29.pdf. Accessed March 2, 2015.
Vincent GK, Velkoff VA. The next four decades: the older population in the United States: 2010 to 2050: population estimates and projections. US Census Bureau; May 2010. http://www.census.gov/prod/2010pubs/p25-1138.pdf. Accessed March 2, 2015.
Social Security Advisory Board. The Unsustainable Cost of Health Care. http://www.ssab.gov/documents/TheUnsustainableCostofHealthCare_graphics.pdf. September 2009. Accessed March 2, 2015.
Autism Speaks. FAQs: state autism insurance reform laws. http://www.autismspeaks.org/advocacy/insurance/faqs-state-autism-insurance-reform-laws. Accessed November 1, 2014.
Gov. Kasich signs directive mandating coverage for autism. NBC4 Columbus. January 9, 2013. http://www.nbc4i.com/story/20752009/gov-kasich-signs-directive-mandating-coverage-for-autism. Accessed March 2, 2015.
National Conference for State Legislatures. Insurance coverage for autism. http://www.ncsl.org/research/health/autism-and-insurance-coverage-state-laws.aspx. August 2012. Accessed March 2, 2015.
Centers for Disease Control and Prevention. 2009-2010 national survey of children with special health care needs. http://www.cdc.gov/nchs/slaits/cshcn.htm. Accessed November 1, 2014.
US Census Bureau. US and world population clock. http://www.census.gov/popclock/. Accessed December 14, 2014.
Early intervention service provider, 34 CFR sec 303.12(c) (2014).
Centers for Disease Control and Prevention. Autism spectrum disorder (ASD): treatment. http://www.cdc.gov/ncbddd/autism/treatment.html. March 13, 2014. Accessed March 2, 2015.
2011 Ark Acts, Act 196.
Ind Code sec 27-8-14.2.
Va Code Ann sec 38.2-3418.17.
NH Rev Stat Ann sec 417-E:2.
Mass Gen Laws ch 32A, sec 25.
State plans for medical assistance, 42 USC sec 1396a(a)(10) (2012).
Hearne J, Topoleski J. An overview of the Medicaid program. http://www.cbo.gov/publication/44588. Congressional Budget Office. September 18, 2013. Accessed March 2, 2015.
US Department of Health and Human Services. Definition, medical assistance, Social Security Act sec 1905, 42 USC sec 1396d(a).
Social Security Administration. Supplemental security income: what is supplemental security income? http://www.ssa.gov/ssi/. Accessed November 15, 2014.
US Department of Health and Human Services Administration on Aging. Medicare. http://longtermcare.gov/medicare-medicaid-more/medicare/. Accessed February 26, 2015.
Association of Maternal and Child Health Programs. AMCHP issue brief: the Affordable Care Act and children and youth with autism spectrum disorder and other developmental disabilities. http://www.amchp.org/Policy-Advocacy/health-reform/resources/Documents/ACA_AutismFactSheet_5-3-12.pdf. May 2012. Accessed March 2, 2015.
US Department of Health and Human Services. Early and periodic screening, diagnostic, and treatment. http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Benefits/Early-and-Periodic-Screening-Diagnostic-and-Treatment.html. Accessed November 23, 2014.
Provisions Respecting Inapplicability and Waiver of Certain Requirements of This Title, Social Security Act sec 1915(c), 42 USC sec 1396a (2012).
Duckett MJ, Guy MR. Home and community-based services waivers.Health Care Financ Rev. 2000;22(1):123.
US Department of Health and Human Services. 1915(c) home & community-based waivers. Health Care Financ Rev. 2000;22(1):123-125.
L & M Policy Research. Appendix E: Medicaid 1915(c) ASD specific waivers. In: Autism Spectrum Disorders (ASD): State of the States of Services and Supports for People with ASD. January 24, 2014. http://www.medicaid.gov/medicaid-chip-program-information/by-topics/long-term-services-and-supports/downloads/asd-state-of-the-states-report.pdf. Accessed March 2, 2015.
National Council on Disability. Home and Community-Based Services: Creating Systems for Success at Home, at Work and in the Community. http://www.ncd.gov/publications/2015/02242015. February 24, 2015. Accessed March 2, 2015.
National Core Indicators. NCI performance indicators: evidence for new HCBS requirements and revised HCBS assurances: practical tools for states. http://www.nationalcoreindicators.org/upload/files/HCBS_Reqmts_and_CMS_Assurances_Crosswalk_with_NCI_May_2014_FINAL.pdf. May 29, 2014. Accessed March 2, 2015.
Wisconsin Department of Health Services. 4.06 Medicaid waivers: general limitations. Medicaid Waivers Manual: Allowable Services and Provider Requirements: Chapter IV – Allowable Services and Provider Requirements. https://www.dhs.wisconsin.gov/sites/default/files/legacy/bdds/waivermanual/waiverch04_10.pdf. January 2010. Accessed March 2, 2015.
Olmstead v LC, 527 US 581, 608 (1999).
ABLE Act of 2014, HR 647, 113th Cong (2014).
Hearne, Topoleski, 608.
CMS manual system: Pub. 100-07: provider certification. Centers for Medicare and Medicaid Services; 2010:2. https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R65SOMA.pdf. Accessed March 2, 2015.
Lord C, McGee J, eds; National Research Council. Educating Children with Autism. Washington, DC: National Academies Press; 2001:1.
Centers for Disease Control and Prevention. Autism spectrum disorder (ASD): data & statistics. http://www.cdc.gov/ncbddd/autism/data.html. Accessed February 26, 2015.




{kind=link}