State of the Art and Science
Jul 2005
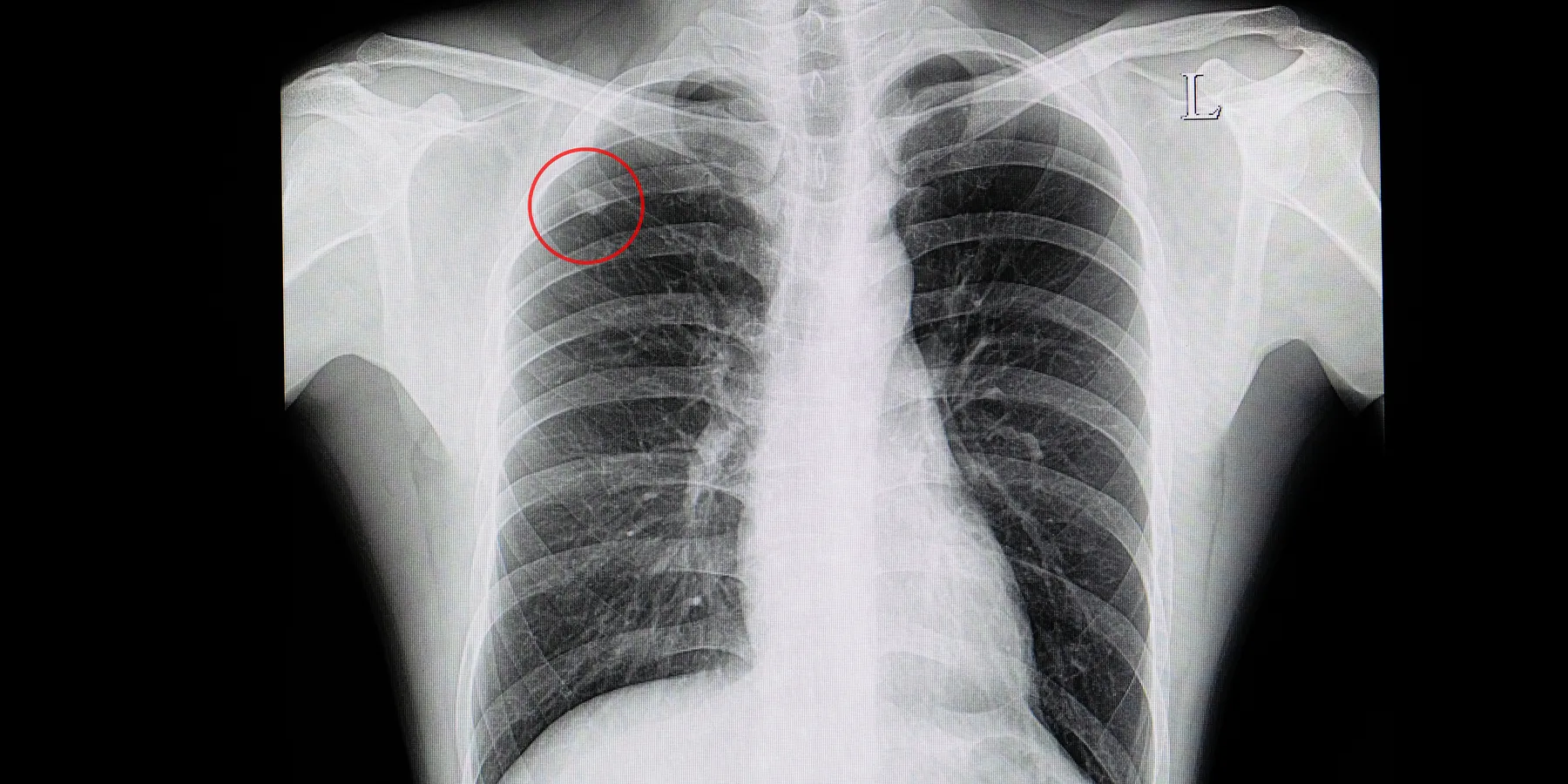
A solitary pulmonary nodule (SPN) is a single, spherical lesion that is less than 3 cm in diameter and completely surrounded by lung parenchyma.
The incidence of a SPN on plain chest radiographs ranges from 0.09 percent to 0.2 percent.1 With the increase in chest CT scans for a variety of reasons, more SPNs are being found that would have gone undetected on plain chest radiographs. Some SPNs require evaluation or treatment and some can be monitored over time and re-imaged. When should a clinician evaluate and treat a SPN by bronchoscopy, needle biopsy, or surgical excision?
The evaluation of a SPN balances the probability that the lesion is malignant and the need to detect malignancy at the earliest stage against the cost, complications, sensitivity, and specificity of various diagnostic approaches and the desire to avoid invasive strategies in patients with benign disease or comorbidities that predispose them to complications. And, of course, patient preferences weigh in. Given these considerations, this article proposes a general approach to evaluating patients with a SPN.
The potential cause of a solitary pulmonary nodule that is of most concern is cancer. For this reason, the initial differential diagnosis is often divided into 2 broad categories: benign and malignant. While numerous studies have attempted to predict the likelihood that a SPN is cancerous, the data have to be interpreted in lieu of the specific patient population studied. Ultimately, predicting malignancy remains an inexact science. The most common method uses a Bayesian approach in which pretest probability is assessed by clinical evaluation and modified by the results of a number of newer diagnostic tests.
Patient factors associated with an increased likelihood of malignancy include older age, a history of smoking, and a history of prior malignancy.2,3
Radiographic characteristics that have been proposed as useful when making an assessment include:
Diagnostic options include monitoring with serial radiographs, obtaining a PET scan, performing bronchoscopy or transthoracic needle aspiration, and resecting the lesion by thoracotomy or video-assisted thoracoscopy.
Watchful waiting with serial CT scans is the least invasive approach, but observing a lesion increases the risk that a metastasis might occur if the lesion is malignant, or that an infectious disease will worsen or spread to others. Generally, observation with repeated imaging is reserved for patients who are thought to have a very low risk of malignancy, those with comorbid conditions for whom more invasive approaches would increase the risk of complication or death, and those who choose this approach for personal reasons. Patients who opt for watchful waiting and serial roentgenographic monitoring should have a chest CT every 3 months for the first year and every 6 months for the following year unless the lesion grows. If no change in size occurs over the 2 years then no further follow-up is needed.
Bronchoscopy has a lower rate of complications (eg, pneumothorax, hemorrhage, death) than transthoracic needle aspiration biopsy, but also has a lower yield. The yield is greater when the SPN is in direct proximity to a bronchus, when the nodule is > 2 cm in diameter, and when the chest CT indicates that a bronchus leads to the nodule. Ultrathin bronchoscopy allows the surgeon to direct the bronchoscope as far as the ninth generation bronchus.1
Transthoracic needle aspiration biopsy is done under CT guidance and has an excellent diagnostic yield with a positive predictive value of 98.6 percent and a negative predictive value of 96.6 percent. The diagnostic yield for lesions smaller than 2 cm is approximately 60 percent (as compared to 10 percent with bronchoscopy). The complication rate, however, is 30 percent (as compared to 5 percent for bronchoscopy).1
Thoracotomy done either by video assistance or by direct visualization (open) has a mortality rate of 0.5-5.3 percent.4
PET scans seem to have a greater ability than CT scans to detect occult metastatic disease, improve accuracy of stage classification, and increase the sensitivity of finding mediastinal lymphadenopathy with metastases. One study suggests that PET scanning is also cost-effective in these specific patient subsets:
1. Patients believed to be at low risk for malignancy by clinical evaluation but who have radiographic findings that are of concern for malignancy.
2. Patients believed to be at high risk for malignancy by clinical evaluation but who have radiographic findings that are consistent with a benign condition.
3. Patients believed to be at high risk for malignancy by clinical evaluation who also have a high predicted surgical morbidity or mortality and who are reluctant to pursue more invasive testing.5
After presence of a SPN has been confirmed, a number of potential management strategies may be pursued. In all strategies, the first step should be to review all prior chest radiographs. Unless the lesion is visible on films taken more than 2 years earlier, the nodule should be evaluated further (assuming the patient desires such an approach). Although SPNs from a few benign conditions can enlarge over time, an enlarging lesion must be considered malignant. A chest CT enables the size, location, and density of the lesion to be determined with the greatest sensitivity and specificity. Assuming the lesion does not have any markers of malignancy, individual patient considerations should assist with the plan for subsequent evaluation and treatment. In addition, the risk factors associated with both benign and malignant diagnoses will help guide and facilitate discussions with the patient so that he or she can fully participate in the decision making process.
It should be noted that patients with histories of previous tuberculosis exposure and those residing in areas where coccidiodomycosis or histoplasmosis is endemic might benefit from needle aspiration or bronchoscopy (with or without bronchoalveolar lavage) inasmuch they will have an increased pretest probability of having 1 of these infections.
Patients whose SPNs are not thought to have an infectious etiology will also need to be evaluated for potential neoplastic causes using one of the previously described diagnostic approaches. Any approach should weigh the risks and benefits to the patient and consider the patient's individual wishes and needs.
A pulmonologist should be consulted if the generalist has questions about the best diagnostic approach or if the primary care physician believes that a diagnostic procedure such as bronchoscopy, transbronchial biopsy, or bronchoalveolar lavage is needed. Pulmonologists may also be able to better advise patients regarding the risks and benefits of various approaches. When percutaneous aspiration biopsies are necessary, they are usually performed by invasive radiologists.
If an SPN is growing, or if a patient prefers to have it removed without additional testing and is a viable candidate for surgery, he or she should be referred to a thoracic surgeon.



