Medical Education
Sep 2019
Peer-Reviewed

Much has been written about the need for participants on global health service-learning experiences to contemplate ethical features of their involvement. This literature tends to neglect the role of self-interest in global engagement, however. This article explores how awareness of one’s own interests is critical to successfully engaging in global health experiences and proposes how US-based health professions students and trainees can practice critical self-exploration. Six themes beginning with the letter I (identity, ideology, ignorance, imagination, intention, and investment) are introduced as guides to nourish conscientious, collaborative global health learning and practice.
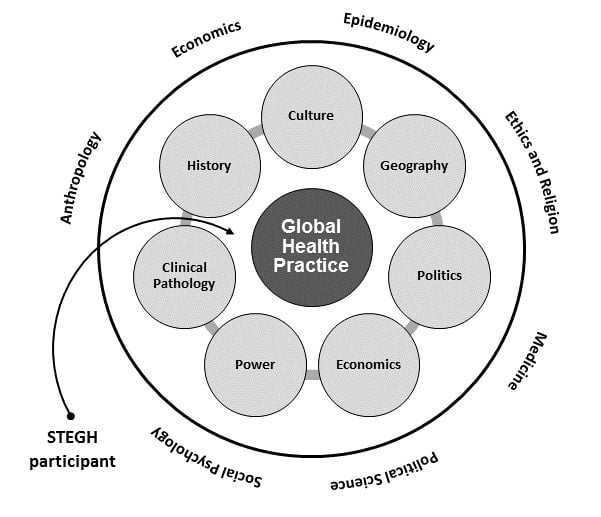
The work of global health is complex.1 It is as much about the study and application of anthropology, economics, political science, and psychology as about physiology and pharmaceuticals.2 It is as much about pathologies of power and good governance as about emerging infectious diseases.3,4,5 It is as much about relationships as about medical science.6 Opportunities for US-based health professions students and trainees to examine these complexities often come in the form of short-term experiences in global health (STEGHs)—service-learning immersions in international and domestic settings of need (see Figure 1).
Figure 1. Complexity in Global Health Practice—Representative Considerations and Areas of Study for Participants/Learners on STEGHs
Much has been written about the need for participants in service-learning experiences to contemplate the ethics of their involvement,7,8,9 but this focus commonly ignores the ways in which self-awareness is integrally intertwined with the concept of global health.10 Self-awareness is the ability to recognize and appreciate one’s perspectives—understandings, values, and biases—in relation to the complicated interpersonal and material worlds in which one lives.11 These perspectives are borne of experiential histories and acquired knowledge that give meaning to thoughts and actions.12 Insofar as STEGHs expose students and trainees to clinical and cultural environments markedly different than those to which they are accustomed, STEGHs create opportunities to cultivate self-awareness and, ultimately, foster mutually beneficial relationships that are relatively free of exploitation.
Absent self-awareness, US health professions students and trainees on STEGHs can project cultural insensitivity,13 act in ways that perpetuate patterns of domination,14 or unwittingly sabotage well-laid plans for implementing appropriate health care interventions.15 They could also underestimate the difficulty of creating equitable partnerships and promoting social change given significant differences in power, capital, and culture that exist around the world.16 Indeed, for students and trainees on STEGHs, self-awareness can be a defense against cultural ignorance or a lack of empathy and can help foster global humility.17
Nonetheless, simply participating in a STEGH does not guarantee growth in self-awareness and may even reinforce harmful preconceptions and prejudices. Pre- and post-STEGH educational sessions can help ameliorate such untoward consequences,18 just as writing narrative essays and attending to ethical guidelines for global health experiences can aid in personal and professional development.19,20,21,22,23 However, the key to growing self-awareness in relation to global health is critical self-exploration—the mindful, imaginative, and enduring practice of identifying and challenging one’s assumptions and actions in light of new information arising from exposure to new surroundings and the passage of time.24,25,26 On the basis of my more than 30 years’ work as a clinician-educator serving in US safety-net clinics and on several international engagements, I contend that developing self-awareness by practicing critical self-exploration is crucial for health professions students and trainees taking part in STEGHs.27
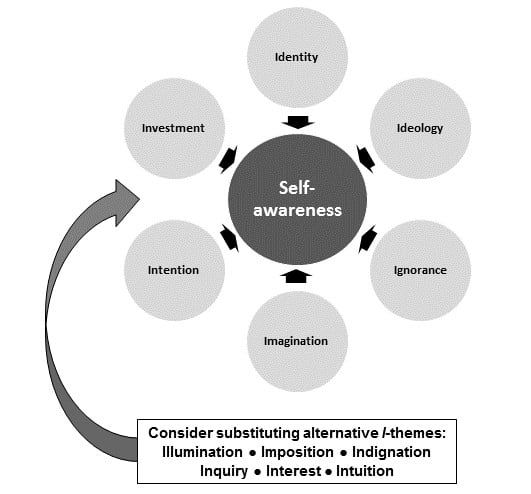
To encourage activities aimed at critical self-exploration in the context of STEGHs, I suggest 6 themes for use as reflective prompts: identity, ideology, ignorance, imagination, intention, and investment. These themes have emerged from experiences and conversations I have had and observations I have made along my professional path.
Each theme begins with the letter I to emphasize self-reflection as a critical component of professional development,28 cultural competency,29 and the transmission of knowledge30 (see Figure 2). Each builds on the concept of social construction,31 the idea that what we authentically bring to interpersonal encounters and how we interact in these encounters help us learn both individually and in community with others.32 Each theme is paired with several self-reflective questions informed by the framework of appreciative inquiry, an asset-based approach that promotes successful interactions in challenging environments.33
Figure 2. I-Themes for Developing Self-awareness as Participants in Short-term Global Health Experiences
Identity. Identity can be defined as the distinguishing character or personality of an individual. In the context of STEGHs, identity is linked to one’s relational “footprint” and, accordingly, encompasses such interpersonal qualities as reciprocity, generosity, and presence.34 In the context of global health, questions that speak to building and maintaining an authentic identity35 that fosters the compassion and insight essential to equitable, collegial, and supportive relationships include the following:
Ideology. Ideology can be defined as a system of beliefs that prescribe how people in a group are typically expected to act. Ideologies are typically religious, economic, or political in nature and may manifest as projections of power.36 Across boundaries of culture and geography, ideologies often compete with each other. As such, it is worthwhile to ask the following questions:
Ignorance. Ignorance is a lack of information or the state of being uninformed. It is a major factor in people’s inability to appreciate how societal forces create and perpetuate adverse social determinants such as poverty,37 racism,38 gender discrimination,39 and globalization.40 The following 4 questions can help circumscribe the limits of one’s knowledge and awareness.
Imagination. Imagination can be defined as the ability to be creative and resourceful or as the capacity to use creativity in the service of adaptability. Both traits are essential in many areas of the world where accessible medical care is lacking. This reality suggests 4 questions:
Intention. Intention can be defined as the purpose that underlies actions. It includes aspects of forethought and planning as part of the process that moves people to act. Exploring one’s intention in participating in STEGHs is especially important for positioning one’s objectives on the spectrum between learning and service (ie, between enhancing open-minded understanding and achieving purposeful outcomes). Intention suggests several questions, especially when one is faced with clinical concerns beyond the scope of one’s previous training.
Investment. Investment can be defined as devoting time, effort, and energy to undertakings with the expectation of worthwhile results. Expectations of STEGHs vary, depending on how much one is willing and able to contribute. Reasonable questions include the following:
The use of these I-themed questions to promote self-awareness is appropriate before, during, and after participation in STEGHs. As with any educational activity that may well touch on emotional issues, care must be taken to create a safe space for learners to disclose deeply personal concerns.44 Many pedagogical modalities—among them narrative writing exercises,45 prospective case-study discussions,46 presentation of relevant movies or film clips,47 and even interactive online courses48—can be used to initiate self-exploration using the above questions. However, simply encouraging STEGH participants to share their personal reflections as they arise may be the most effective method to stimulate the growth of self-awareness.49 Such critical incident learning, cultivated by STEGH participants’ sense of curiosity, suspension of immediate judgment, and mindful attention to experience,50 can occur individually with supportive mentors or in groups with peers.
Of vital importance, these I-themes should neither be perceived as simply an inventory of competencies to be acquired nor taught as bullet points for rote acquisition.51,52 Coupled with an inquisitive stance vis-à-vis other people,53 they are prompts to learning through emergent reflection. Furthermore, they should not be seen as comprehensive in scope. Other I-themes are equally suitable (eg, illumination, imposition, indignation, inquiry, interest, or intuition), and non-I words pose assorted alternative themes for further inspiration. Lastly, none of the I-themes concerns solely international initiatives. Students and trainees might substitute local for global and consider how their points of view shape their personal and professional formations at home.17
STEGHs are one way for US health professions students and trainees to begin to appreciate the complex nature of the work of global health. By developing self-awareness through critical self-exploration, budding health professionals can maximize their ability to learn—conscientiously, collaboratively, and constantly—about this complexity. My hope is that these I-themes and corresponding questions will help participants in STEGHs in this endeavor, which is essential to enriching global health practice and advancing the health of the public.
Nichter M. Global Health: Why Cultural Perceptions, Social Representations, and Biopolitics Matter. Tucson, AZ: University of Arizona Press; 2008.
Farmer P. Pathologies of Power: Health, Human Rights, and the New War on the Poor. Berkeley, CA: University of California Press; 2003.
Farmer P, Kleinman A, Kim J, Basilico M. Reimagining Global Health: An Introduction. Berkeley, CA: University of California Press; 2013.
Ventres WB, Fort MP. Eyes wide open: an essay on developing an engaged awareness in global medicine and public health. BMC Int Health Hum Rights. 2014;14(1):29.
Ventres W, Wilson B. Rethinking goals: transforming short-term global health experiences into engagements. Acad Med. In press.
EIESL Project. EIESL (Ethics of International Engagement and Service-Learning) Project. http://ethicsofisl.ubc.ca/?page_id=65. Accessed November 24, 2018.
Crump JA, Sugarman J; Working Group on Ethics Guidelines for Global Health Training (WEIGHT). Ethics and best practice guidelines for training experiences in global health. Am J Trop Med Hyg. 2010;83(6):1178-1182.
DeCamp M, Rodriguez J, Hecht S, Barry M, Sugarman J. An ethics curriculum for short-term global health trainees. Global Health. 2013;9:5.
DeCamp M, Lehmann LS, Jaeel P, Horwitch C; ACP Ethics, Professionalism and Human Rights Committee. Ethical obligations regarding short-term global health clinical experiences: an American College of Physicians position paper. Ann Intern Med. 2018;168(9):651-657.
Frankel R, Beyt G. Appreciative inquiry: fostering positive culture. American Medical Association. https://edhub.ama-assn.org/steps-forward/module/2702691. Accessed February 21, 2019.
Walraven G. Health and Poverty: Global Health Problems and Solutions. London, UK: Earthscan; 2011.
Phillips SP. Defining and measuring gender: a social determinant of health whose time has come. Int J Equity Health. 2005;4(1):11.
Ventres W, Haq C. Toward a cultural consciousness of self in relationship: from “us and them” to “we.” Fam Med. 2014;46(9):691-695.
Ventres WB, Wilson CL. Beyond ethical and curricular guidelines in global health: attitudinal development on international service-learning trips. BMC Med Educ. 2015;15(1):68.
Jacquet GA, Umoren RA, Hayward AS, et al. The Practitioner’s Guide to Global Health: an interactive, online, open-access curriculum preparing medical learners for global health experiences. Med Educ Online. 2018;23(1):1503914.



