Original Research
May 2023
Peer-Reviewed
Background: Classroom-based interprofessional education (IPE) has been shown to improve medical students’ understanding of IPE competencies, but less is known about how those skills apply in clinical environments. This study assesses an IPE session’s influence on medical students’ interactions with cross-disciplinary colleagues during their pediatrics clerkship.
Methods: Medical, nursing, and pharmacy students in pediatrics clinical rotations participated in an hour-long, virtual classroom-based small-group IPE activity in which they answered questions about a hypothetical case of a febrile neonate’s course of hospitalization. Each student received answers to these questions given to students from other professions, such that answering the questions from the perspective of their own profession required the students to share and gather information from other students in their group. After the session, students completed retrospective pre- and postsession self-assessments of their achievement of IPE session objectives, which were analyzed using the Wilcoxon signed-rank test. They also participated in focused interviews that were analyzed qualitatively to explore the session’s influence on their clinical experiences.
Results: Medical students’ retrospective pre- and postsession self-assessment ratings differed significantly, indicating improvement in students’ IPE competencies. However, interviews revealed that less than one-third of medical students applied IPE skills during their clerkship due to lack of autonomy and confidence.
Conclusions: The IPE session’s influence on medical students’ interprofessional collaboration was minimal and suggests that classroom-based IPE has limited impact on students’ interprofessional collaboration in the clinical learning environment. This finding suggests the need for intentional, clinically integrated IPE activities.
One purpose of interprofessional education (IPE) is to prepare students to participate in interprofessional collaborative practice, which requires them to meet the 4 core IPE competencies, as set forth by the Interprofessional Education Collaborative (IPEC): (1) contributing to an environment of shared values and ethics for interprofessional practice; (2) understanding the roles and responsibilities of members of the health care team; (3) supporting a team approach to care via interprofessional communication; and (4) collaborating effectively within the health care team.1 IPE produces measurable improvements in students’ abilities to meet the IPEC competencies, as it has been shown to increase students’ understanding of the importance of communication and teamwork to patient care,2,3 their understanding of their roles and responsibilities,2,3,4 and their ability to function within the health care team.5 Additionally, IPE promotes positive impressions of and interactions among professions.6
IPE can take place in various settings, including in-person or virtual classrooms, simulation centers, clinics or hospitals, and community sites.7,8 In medical school, formal IPE is often included in preclinical classroom instruction and activities with students from other health professions.9 Although previous studies have highlighted the value of IPE in clinical settings,10,11,12 many medical schools do not formally include IPE in clerkships.13,14,15 Once students are on their clinical rotations, the belief is that they will continue to learn collaborative practice by being on health care teams and coexisting with other health care students and professionals.16 Yet students from different professions training at the same clinical site often work and learn in their respective professional silos,17 making it less likely that they will have opportunities to learn about, from, and with one another.18 Previous studies have shown that classroom-based IPE is effective in improving students’ self-assessed understanding of IPE principles and attitudes toward interprofessional collaboration.9,19,20,21 However, translating theoretical IPE classroom-based knowledge into practical clinical skills remains a challenge, and measuring the real-world impact of classroom-based IPE sessions is a significant knowledge gap.9,19,20,21
To increase interprofessional socialization, we developed and implemented an IPE session for medical, nursing, and pharmacy students who were doing their pediatrics clinical rotations at the same children’s hospital at the same time and used self-assessments and interviews to evaluate the session. The aim of this mixed-methods study was to assess the impact of a classroom-based IPE session on medical students’ self-reported confidence with respect to the 4 IPEC competencies, as well as to assess their application of those competencies in working with different health care professionals during their pediatrics clerkship.
Participants. Thirty third-year medical students who participated in 1 of 3 identical IPE sessions from June 2021 to August 2021 at the beginning of their inpatient pediatrics clerkship (at the same clinical site) were included in the study, with 23 partaking in follow-up interviews. While session feedback and evaluation information were collected from nursing and pharmacy students for educational quality purposes, those data were not included in this study, as institutional review board (IRB) approval was specifically for data from the medical students. Because the nursing and pharmacy students in each of the 3 identical sessions were usually from several different institutions, obtaining IRB approval to collect and analyze data from these participants was not feasible. As a result, this study is a focused analysis of the session’s impact on third-year medical students.
Procedure. We created an hour-long, virtual classroom-based small-group IPE activity, which required students to collaborate in order to successfully work through a hypothetical clinical case of a febrile neonate’s hospital course. The IPE activity was conducted 3 times with different small groups, consisting of 4 to 5 students, who were a mixture of medical, nursing, and pharmacy students, as well as a faculty facilitator from one of those professions whose role was to observe the students’ interactions. Students were each given a version of the case from the perspective of their respective professions, which exemplified the roles and responsibilities of their profession in caring for this patient. Each version of the case study contained different questions that students were required to answer. The answers to these questions were included in the information given to the students from other professions, such that, in order to answer these questions, students needed to share and gather information from the other students in their group. This arrangement effectively required students to communicate and collaborate interprofessionally. Once the students had completed the session, the facilitator held a debriefing on their experiences, exploring what went well and the challenges of the activity within the context of the 4 IPE competencies.
Immediately following the IPE session, students completed a retrospective pre- and postsession self-assessment on the following session objectives that coincide with the IPEC competencies: (1) communicate information with health care team members in a way that is mutually understandable, (2) engage health professionals in shared problem solving, (3) recognize how the skills and knowledge of other health professionals complement and overlap with each other, and (4) reflect on how individual and team performance could be improved. Before and after the session, students rated their ability on each of these skills from low (1) to high (5) on a 5-point Likert scale, which provided a quantitative assessment of students’ self-assessed learning following IPE sessions.22
At the end of the 4-week inpatient pediatrics clerkship, medical students were invited to participate in brief interviews to further assess their experience of the IPE session and how it affected their interprofessional interactions during the clerkship. Interviews were conducted with 2 to 3 students at a time by the same member of the research team to maintain consistency. Questions that were asked included (1) What were the key takeaways that you learned during the session? (2) What was your perception of interprofessional collaboration prior to participating in the session? (3) How did the IPE session affect your understanding of roles and responsibilities on the health care team? (4) Did the IPE session change your ability to collaborate or your confidence in collaborating with other health care professionals? If so, how? (5) What aspects of the IPE session were helpful, and what aspects of the IPE session could be improved? Interviews were recorded using an audio recorder. Interview recordings were then transcribed verbatim, and recordings were subsequently deleted to protect students’ anonymity.
Data analysis. Retrospective pre- and postsession self-assessment data for the 3 sessions were pooled and analyzed using the Wilcoxon signed-rank test. Interviews were transcribed, codified, and analyzed by the first author (M.C.P.) using qualitative content analysis. Keywords, phrases, and ideas identified in students’ interview responses were color coded in interview transcripts. Interview transcripts were analyzed individually to highlight the keywords, phrases, and ideas that were repeatedly emphasized by students. Thus, the analysis facilitated the identification of common themes from students’ interview responses.
Retrospective pre- and postsession self-assessment. The distributions of students’ pooled pre- and postsession self-assessment responses from the 3 sessions are displayed in the Figure. Retrospective pre- and postsession self-assessment ratings differed significantly, indicating students’ increased confidence in their interprofessional communication skills (objective 1), team-based problem-solving skills (objective 2), understanding of roles and responsibilities (objective 3), and ability to reflect on performance for improvement (objective 4) (p < 0.01 for all objectives).
Figure. Distributions of Pooled Pre- and Postsession Self-Assessment Ratings on 4 Objectives
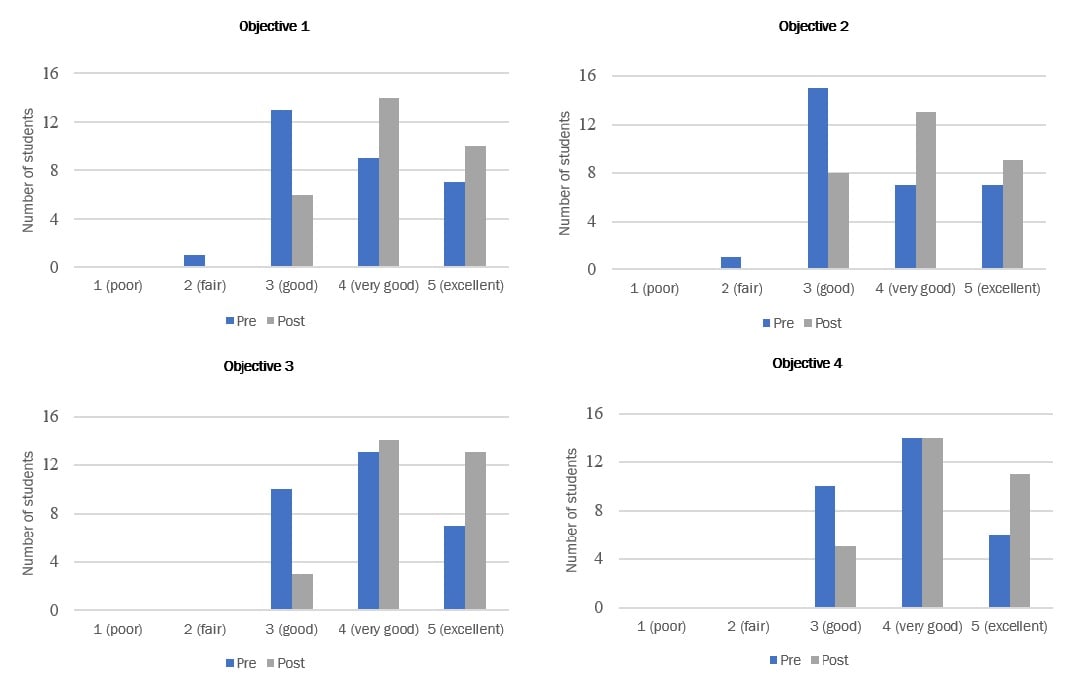
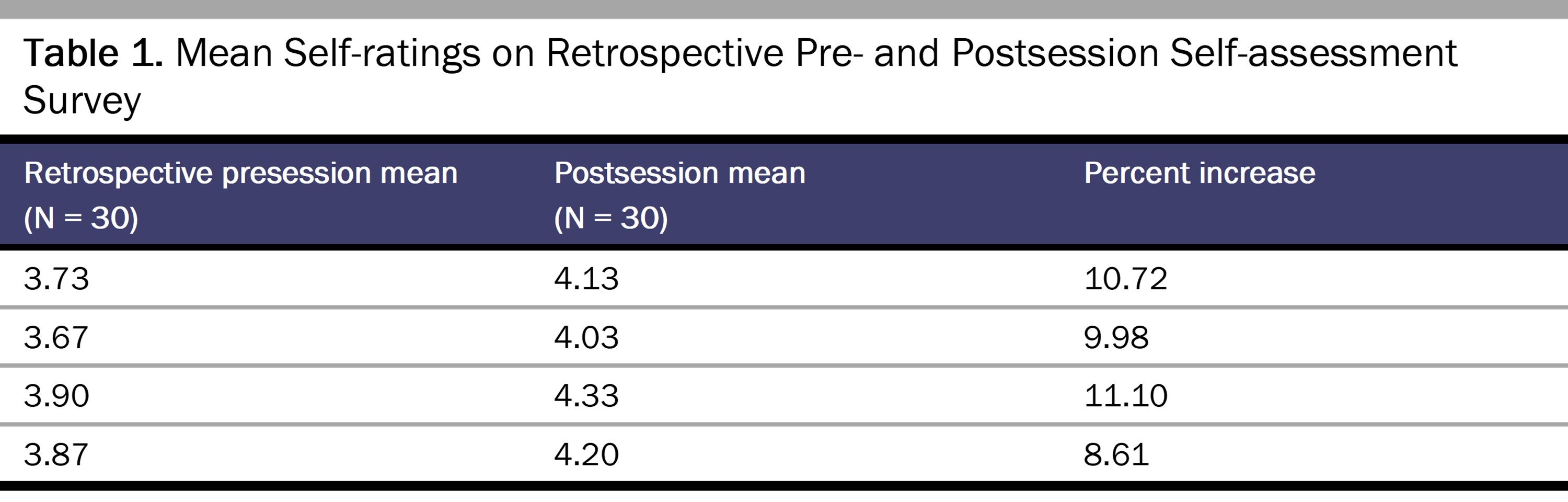
Table 1 displays the mean pre- and postsession self-assessment ratings pooled over the 3 sessions.
Postclerkship follow-up interviews. Keywords, phrases, and ideas were identified in interview responses of 23 students and summarized in 6 key themes, several of which focus on students’ experience during the session (see Table 2). Specifically, 91.30% of students reported that the case-based format was beneficial, as it was engaging, encouraged collaboration, and provided a clinical context to IPE. However, 30.43% of students felt that the IPE sessions repeated content from previous IPE sessions, and 30.43% of students also said that their experience during the session was dependent on the level of engagement from other students. In addition, 91.30% of students reported that the virtual platform negatively impacted their experience because it was difficult to replicate clinical communication virtually, and several students reported that an in-person session would have been more effective. Students also reported improvements in their mastery of IPE core compentencies, specifically in their knowledge of roles and responsibilities (69.57%) and practice of interprofessional communication (56.52%).
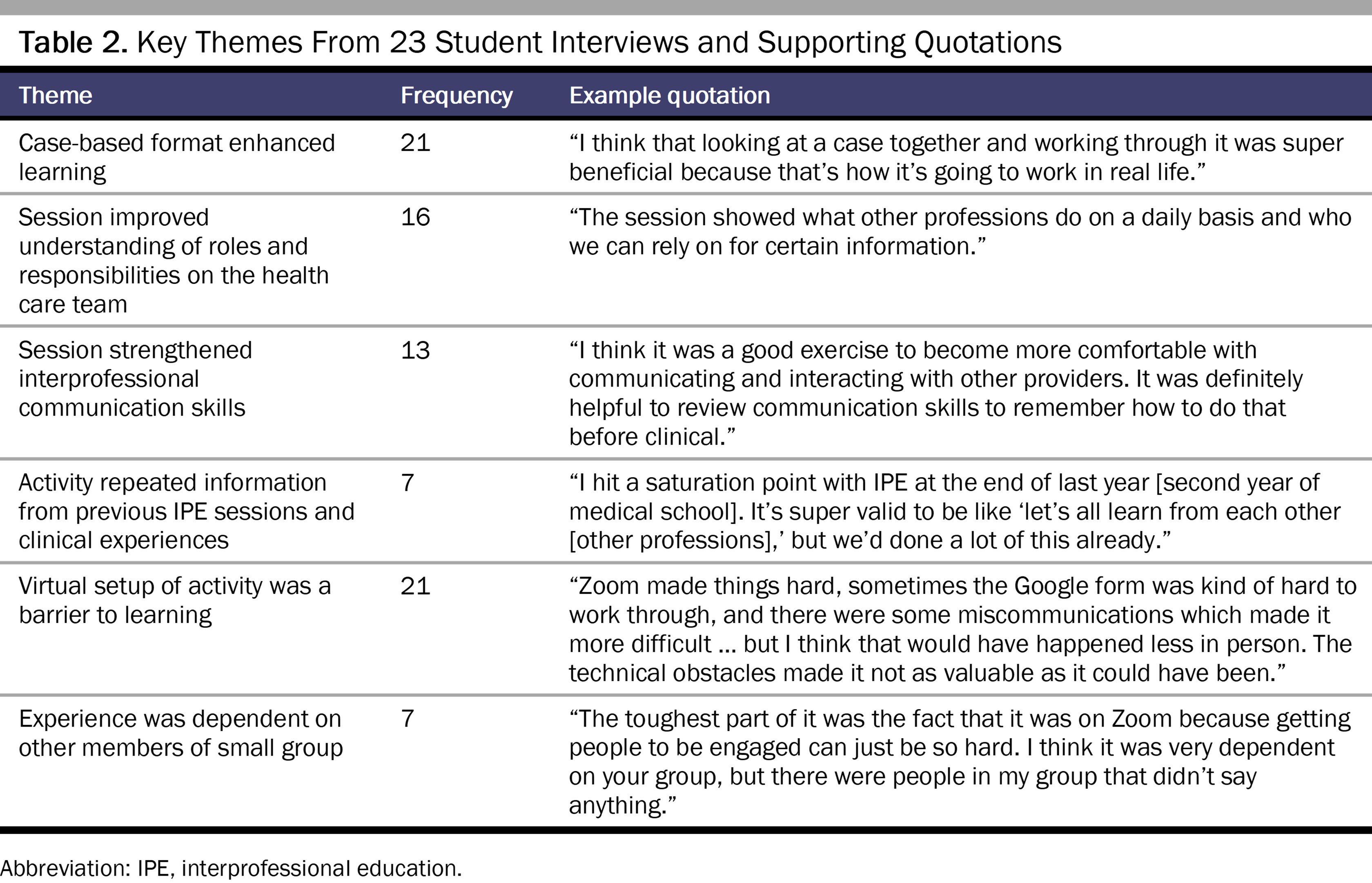
Only 7 of the 23 students who were interviewed said they applied these skills during their clerkship, however. Some students said they were unable to apply these interprofessional collaboration skills during the rotation due to lack of autonomy early in their clinical training, lack of confidence as new members of the health care team, and adjustment to the clinical learning environment.
Effective IPE is critical at all stages of medical education to prepare students to be collaborative members of the health care team. The classroom-based IPE session we developed for medical students during their pediatrics clerkship built upon foundational IPE sessions they received during their preclinical years. Overall, the sessions seemed to be effective in improving students’ self-assessed ability to meet specific IPEC competencies but had less impact on students’ application of the competencies during their clerkship.
In the postsession surveys, students more highly rated their postsession ability to meet session objectives, especially the IPEC core competencies of interprofessional communication and understanding of roles and responsibilities. When asked about these learning improvements during follow-up interviews, students highlighted the case-based format of the IPE session as a major strength that enhanced their learning. Students further reported that the format encouraged collaboration among students from different professions, making the session more engaging, which was especially beneficial given the inherent challenges of maintaining student engagement on virtual learning platforms.23,24,25
Despite students’ self-reported learning improvements following the IPE sessions, follow-up interviews also highlighted several reasons why less than one-third of medical students who participated in the interviews felt that the IPE session influenced their interprofessional interactions during their pediatrics clerkship. First, many students reported that the virtual platform was not ideal and that in-person sessions would have better facilitated socialization, perhaps by prompting increased recognition when students saw each other again in the hospital. Second, several students felt that the session repeated the preclinical IPE curriculum, as it was still a classroom-based activity, although it occurred during the clerkship. This finding suggests that IPE in the clinical learning environment needs to have a clinically authentic context and be integrated into patient care.
Given that this study included third-year medical students who were just beginning their clinical education, the timing of IPE sessions may have also contributed to their lack of impact. Students voiced feeling a lack of autonomy and confidence in reaching out to other professionals without direction from interns and residents. They also reported being too overwhelmed by their own new role and responsibilities to be able to figure out how to work with other professionals on the health care team. One student summarized this sentiment by saying, “Once I’m in a position to keep my head above water, it [interprofessional communication] will happen more naturally.” The additional cognitive load from the IPE session may have made it too much for students to internalize and apply the competencies so early on in their clinical training. It would be interesting to see if students who participated in the IPE session later in their clincial training have a different impression of its applicability and of their own abilities to incorporate interprofessional collaboration skills more readily.
This study has several limitations that can be improved upon in future studies. First, the sample size was determined based on the number of students who participated in the IPE sessions rather than the number needed for achieving adequate statistical power. Additionally, this study focused on the experiences of third-year medical students only. Previous studies have found that nursing and pharmacy students benefit from IPE sessions through increased understanding of their own and other professionals’ roles and responsibilities and improved attitudes toward interprofessional collaboration.26,27 Therefore, nursing and pharmacy students’ experiences with clinically integrated classroom-based IPE sessions, such as the one highlighted in this study, should be included in future studies for comparison. Finally, this study primarily relied on self-reported measures. While self-assessment is a critical component of medical education,28,29 the results may not always align with objective assessments.30 Including objective measurements, such as direct observation, in an assessment is important to better understand interprofessional interactions.
Overall, this study builds on existing literature that supports the value of classroom-based IPE sessions in improving students’ self-assessed understanding of interprofessional collaboration. This study also highlights the limited impact that a classroom-based IPE session has on medical students’ interactions with other health care professionals, despite the session bringing together different health care professions students, some of whom are working in the same clinical setting. Location (in person vs virtual), timing, and integration of IPE into clinical care are all important factors in the impact of IPE on interprofessional collaboration.
Interprofessional Education Collaborative. Core competencies for interprofessional collaborative practice: 2016 update. Interprofessional Education Collaborative; 2016. Accessed August 1, 2022. https://ipec.memberclicks.net/assets/2016-Update.pdf
Homeyer S, Hoffmann W, Hingst P, Oppermann RF, Dreier-Wolfgramm A. Effects of interprofessional education for medical and nursing students: enablers, barriers and expectations for optimizing future interprofessional collaboration—a qualitative study. BMC Nurs. 2018;17:13.
Darlow B, Coleman K, McKinlay E, et al. The positive impact of interprofessional education: a controlled trial to evaluate a programme for health professional students. BMC Med Educ. 2015;15:98.
González Blum C, Richter R, Fuchs R, Sandeck F, Kunz K, Heermann S. Interprofessional education in medical and physiotherapy studies for future collaboration. Ann Anat. 2022;240:151850.
van Diggele C, Roberts C, Burgess A, Mellis C. Interprofessional education: tips for design and implementation. BMC Med Educ. 2020;20(suppl 2):455.
Keshmiri F, Barghi TS. Interprofessional education in a community-based setting: an opportunity for interprofessional learning and collaboration. J Educ Health Promot. 2021;10:298.
Vuurberg G, Vos JAM, Christoph LH, de Vos R. The effectiveness of interprofessional classroom-based education in medical curricula: a systematic review. J Interprof Educ Pract. 2019;15:157-167.
Cant R, Morphet J, Hood K, Baulch J, Gilbee A, Sandry K. Teaching teamwork: an evaluation of an interprofessional training ward placement for health care students. Adv Med Educ Pract. 2014;5:197-204.
Barone MA, Bannister S, Dudas RA. Interprofessional education in pediatric clerkships: a survey of pediatric educators in North America. J Interprof Educ Pract. 2017;6:61-65.
Kalb KA, O’Conner-Von S. Strategies in education: breaking down silos, building up teams. J Cathol Health Assoc U S. May-June 2012. Accessed August 1, 2022. https://www.chausa.org/publications/health-progress/article/may-june-2012/strategies-in-education-breaking-down-silos-building-up-teams
Health Professions Networks Nursing and Midwifery Office, Department of Human Resources for Health. Framework for action on interprofessional education and collaborative practice. World Health Organization; 2010. Accessed June 29, 2022. http://apps.who.int/iris/bitstream/handle/10665/70185/WHO_HRH_HPN_10.3_eng.pdf;jsessionid=9D56AA5913830C3E80571CDE32B611C3?sequence=1
Anderson JE, Ateah C, Wener P, et al. Differences in pre-licensure interprofessional learning: classroom versus practice settings. J Res Interprof Pract Educ. 2011;2(1):10.22230/jripe.2011v2n1a54.
McCormack Tutt SA. Healthcare Students’ Abilities to Translate Interprofessional Education to Collaborative Practice. Dissertation. University of New England; 2019. Accessed June 27, 2022. https://dune.une.edu/cgi/viewcontent.cgi?article=1002&context=pt_facpubs
Teuwen C, van der Burgt S, Kusurkar R, Schreurs H, Daelmans H, Peerdeman S. How does interprofessional education influence students’ perceptions of collaboration in the clinical setting? A qualitative study. BMC Med Educ. 2022;22(1):325.
Wilcha RJ. Effectiveness of virtual medical teaching during the Covid-19 crisis: systematic review. JMIR Med Educ. 2020;6(2):e20963.
Simko LC, Rhodes DC, McGinnis KA, Fiedor J. Students’ perspectives on interprofessional teamwork before and after an interprofessional pain education course. Am J Pharm Educ. 2017;81(6):104.
Kennedy G, Rea JNM, Rea IM. Prompting medical students to self-assess their learning needs during the ageing and health module: a mixed methods study. Med Educ Online. 2019;24(1):1579558.



