Medicine and Society
Mar 2024
Peer-Reviewed

Inpatient psychiatric units should be therapeutic environments that support dignity and recovery. When adverse outcomes (eg, self-harm, violence) happen in these settings, clinicians and administrators can face litigation and other pressures to prioritize risk management over supporting patients’ access to personal belongings, exercise equipment, and private spaces. This article describes these downward pressures toward sparser, controlling environments in inpatient psychiatric settings as a safety funnel and suggests strategies for balancing safety, humanity, and recovery in these contexts.
Inpatient psychiatric units are supposed to offer therapeutic environments for patients to recover from severe psychiatric symptoms. As far back as 1847, Thomas Story Kirkbride, a US physician, published “Remarks on the Construction and Arrangements of Hospitals for the Insane.”1,2 This treatise focused on all aspects of the design and organization of hospitals for people with mental illness,2,3 such that, as Tomes argues, “every detail, from the design of the window frames to the table settings in the ward dining rooms, had to be arranged to sustain the impression that here was an institution where patients received kind and competent care.”1,3 Long-term psychiatric hospitals in the United States and elsewhere, often referred to as asylums, occasionally had sprawling facilities with acres of land, gardens, chapels, or other amenities for engendering tranquility among the inhabitants.4,5,6
Although large, often state-run, facilities played a considerable role in the care of people with mental illness into the 20th century, by mid-century, increased public awareness of the conditions inside certain facilities, growing emphasis on patients’ rights, and other developments led to a shift away from these types of facilities toward community-based care.7,8 In parallel, the goal of psychiatric hospitalization shifted from long-term psychiatric and custodial care to short-term stabilization.7,9 The evolution of inpatient psychiatric settings toward brief stays has coincided with increased clinical and legal emphasis on promoting safety and preventing adverse events. This article describes the downward pressures toward sparser, controlling environments—what we refer to as the safety funnel—in inpatient psychiatric care. Given potential counter-therapeutic effects of this phenomenon, this article suggests how to balance safety, humanity, and recovery in these clinical settings.
Adverse events, such as self-harm, violence, harassment, and privacy breaches, can occur in inpatient psychiatric settings and can harm patients, staff, and others. For example, pooled estimates based on international data indicate that approximately 147 suicides occur per 100 000 psychiatric inpatient years,10 with one study finding a rate of suicide among psychiatric inpatients that was nearly 50 times greater than in the general population.11,12 In the United States, estimates suggest that approximately 30 to 50 patients receiving inpatient psychiatric care die by suicide each year.13 International estimates suggest that anywhere from 4% to 70% of patients on psychiatric units engage in some degree of nonsuicidal self-injury (eg, cutting, head banging).14 Even with environmental interventions (eg, reducing ligature points), monitoring (eg, placing high-risk patients under staff observation), and other precautions to decrease risks of self-harm, self-injury remains a challenge for staff tasked with caring for patients hospitalized for acute psychiatric symptoms.13,15
Violence may also occur in inpatient psychiatric facilities. A 2015 systematic review examining violence in inpatient psychiatric settings found that approximately 17% of patients committed at least one act of physical violence when data were pooled across roughly 24 000 patients in 35 studies from high-income countries.16 In addition to perpetrating violence, patients may experience physical injury, fear, difficulty recovering from psychiatric symptoms, and other complications related to violent victimization from peers or staff; moreover, inpatient psychiatric staff also face these challenges. According to a 2021 systematic review, approximately 25% to 85% of survey respondents working in inpatient psychiatric facilities in the United States reported experiencing physical aggression in the year prior to the survey.17
Various other adverse events may occur in inpatient psychiatric settings, ranging from breaches of privacy to sexual harassment.18,19 When self-injury, violence, or other adverse events occur in these settings, inpatient psychiatric staff and administrators may face punitive repercussions. Examples might include sanctions by regulatory agencies (eg, loss of accreditation by the Joint Commission, fines by the Occupational Safety and Health Administration), litigation by patients or their families, and litigation by staff, among other possibilities.20,21 According to a 1993 article, “the most common legal action involving psychiatric care is the failure to reasonably protect patients from harming themselves.”21
Adverse event frequency in inpatient psychiatric settings, combined with the threat of punitive actions (eg, regulatory sanctions, litigation), places pressure on inpatient psychiatric staff and administrators to prioritize managing risks of dangerousness over other therapeutic needs of patients (ie, characteristics and features of treatment that promote healing and recovery). For example, because hospitalized patients have attempted or completed suicide with shoelaces or belts in the past, inpatient psychiatric facilities may then develop policies restricting all patients from having these items.22 In response to patients drinking hand sanitizer to become intoxicated, staff members have restricted access to or removed hand sanitizer in psychiatric units to prevent further ingestion of these products.23,24 After investigating a psychiatric facility in Colorado for assaults on staff, among other unsafe work conditions, the Occupational Safety and Health Administration cited several workplace hazards in 2019 and suggested abatement methods, including redesigning nursing stations so that patients cannot access these workstations or items for weapons, such as “hole punchers, staplers, telephones, cords, pens, computers, computer peripherals, and other items.”20,25 Due to security and legal concerns, psychiatric units around the world have installed video surveillance to monitor or record patients and staff on these units.26 As one article about nursing in these environments noted: “Safety is not merely a consideration or goal, but the highest value.”27
Clinical staff and administrators in these settings should remain aware of the need to balance the risks of dangerousness in inpatient psychiatric facilities with the risks of creating dehumanizing and sterile environments that do not support recovery for patients with severe psychiatric needs. For instance, if a patient attempts strangulation with a privacy curtain in a shared room with a roommate, removing all curtains from shared patient rooms without any sort of replacement would entail considerable privacy drawbacks for patients sharing rooms28; nevertheless, it is difficult to measure loss of privacy associated with these types of changes. Similarly, if a patient uses exercise equipment to assault a peer or staff, removing all exercise equipment from patients could have deleterious effects on patients who rely on exercise for their mental and broader well-being.
Many safety measures in inpatient psychiatry, from locked doors to the sight of seclusion rooms, may frighten patients27—to such an extent that some former patients have described themselves as “survivors” of inpatient psychiatric care.29 Patients might experience considerable distress when they lose access to personal belongings or even basic privacy. And while hospitals may remove access to phones, cameras, and other devices that can compromise patient privacy,30 less is often done to mitigate the risk of privacy breaches when staff discuss patients’ personal history and mental health treatment in shared rooms and spaces.28
Therapeutic features of the built environment include the physical resources, structures, policies, and care for patients that provide the physical and emotional space for patients to access therapies to improve mental health and general well-being.31,32 However, features of the built environment may become so centered around safety that they hardly resemble the therapeutic spaces they were conceived to be, with several implications for health equity. Research suggests that racially and ethnically oppressed persons are often more likely to enter the health care system through “coercive agencies,”33 such as the juvenile justice system, child welfare system, and involuntary hospitalization, than their White counterparts.34 Racially and ethnically oppressed patients are also at a greater risk of being placed in restraints in hospital settings, even when they do not differ from White patients in terms of histories of violence or number of violent acts committed.35,36,37 These findings are significant, given that racially and ethnically oppressed groups are also overrepresented in a number of criminal justice settings.38,39,40,41 Extreme safety measures in inpatient psychiatry may include bleak sterile environments, artificial lighting, limited windows, limited privacy, lack of access to personal belongings, and even bolted down beds in rooms with concrete or padded walls; as a result, some psychiatric facilities may resemble carceral settings more than hospital settings. When marginalized individuals are brought to hospitals by law enforcement and then enter inpatient psychiatric settings where safety and prevention are prioritized over all else, the similarities to carceral environments may contribute to their mistrust, trauma, and retraumatization.42
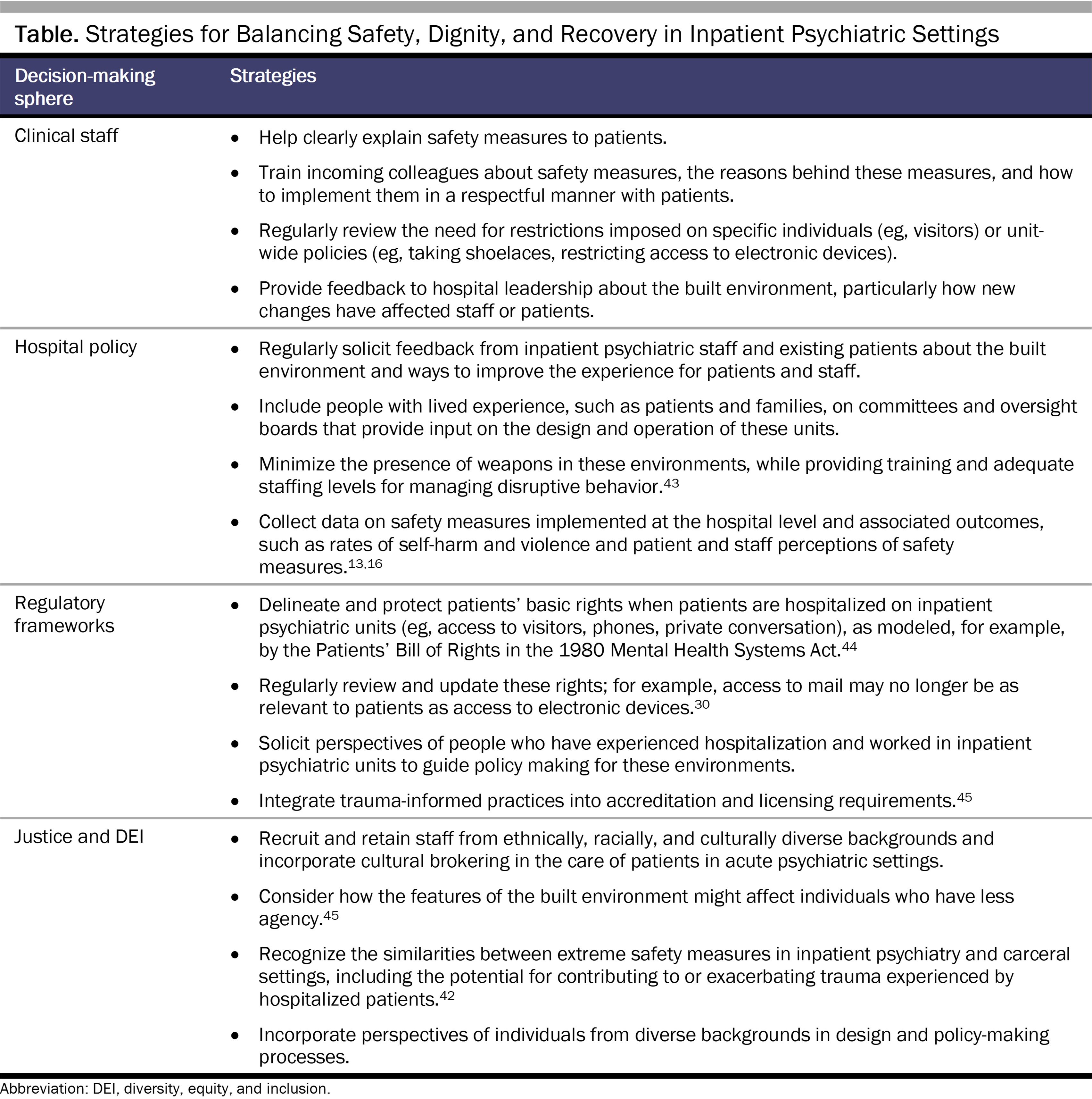
People involved in the design and operation of inpatient psychiatric settings, including clinical staff, hospital administrators, and policy makers, face considerable pressures to reduce the dangerousness of these environments; nevertheless, they must also remain committed to supporting the dignity and recovery of patients hospitalized in these settings. The Table lists different levels of decision making and examples of specific actions to balance safety, dignity, and recovery in inpatient psychiatric units. In particular, partnering with people with lived experience, such as by inviting current or former patients and their families to participate in design and policy making efforts related to inpatient psychiatric care, can integrate into the decision-making process a range of diverse voices and perspectives that can speak to the potential implications of proposed changes.
To guide these efforts, leaders should draw on measured outcomes related to the design and operation of psychiatric facilities to inform evidence-based practices in these environments. Too often, the care of psychiatric patients in inpatient psychiatric facilities is based more on convention and tradition than research or outcomes.46 Nevertheless, more data collection related to safety measures in inpatient psychiatric settings, including outcomes related to adverse events, as well as patient privacy, dignity, and equity, can potentially help facilities balance the risks of dangerousness and the risks of placing patients in dehumanizing environments.13,16,46 For example, the US Department of Veterans Affairs developed a Mental Health Environment of Care Checklist, which included architectural changes to improve inpatient safety, that a 2016 study reported was associated with long-term declines in inpatient suicides.47 However, the brief report did not include additional measures of patient, visitor, and staff perceptions of these changes. Similarly, researchers in Sweden studied design features to reduce violence in psychiatric wards, including not only increased safety measures (eg, designs to facilitate observation) but also stress reduction measures for patients (eg, access to gardens, nature window views, designs for low social density).48 The authors found that these measures were associated with a decreased proportion of patients receiving medication injections for aggression, but the study did not include additional measures of patient or staff perceptions of these features.48
Inpatient psychiatric environments are meant to be places of healing but can also entail risks to the safety and privacy of patients and staff who inhabit these environments. Avoiding the safety funnel is not easy or straightforward, as adverse events in these settings can be traumatic, frightening, and even life-altering. Self-harm, violence, and other adverse safety incidents can occur in other health care settings, such as emergency departments, general medical floors, and intensive care units. Nevertheless, patients and staff should not have to trade their dignity for safety when entering health care environments, including inpatient psychiatric units. Recognizing and addressing the safety funnel is essential for creating inpatient psychiatric facilities where inhabitants can feel not only safe and secure but also human.
Tomes NJ. A generous confidence: Thomas Story Kirkbride’s philosophy of asylum construction and management. In: Scull A, ed. Madhouses, Mad-Doctors, and Madmen: The Social History of Psychiatry in the Victorian Era. University of Pennsylvania Press; 1981:120-143.
Kirkbride TS. Remarks on the construction and arrangements of hospitals for the insane. TK & PG Collins; 1847. Accessed November 30, 2023. https://digirepo.nlm.nih.gov/ext/dw/101684545/PDF/101684545.pdf
Tomes N. The Art of Asylum-Keeping: Thomas Story Kirkbride and the Origins of American Psychiatry. University of Pennsylvania Press; 1984.
Chammas F, Januel D, Bouaziz N. Inpatient suicide in psychiatric settings: evaluation of current prevention measures. Front Psychiatry. 2022;13:997974.
Iozzino L, Ferrari C, Large M, Nielssen O, de Girolamo G. Prevalence and risk factors of violence by psychiatric acute inpatients: a systematic review and meta-analysis. PLoS One. 2015;10(6):e0128536.
Betterly H, Musselman M, Sorrentino R. Sexual assault in the inpatient psychiatric setting. Gen Hosp Psychiatry. 2023;82:7-13.
Hunt IM, Windfuhr K, Shaw J, Appleby L, Kapur N; National Confidential Inquiry into Suicide and Homicide. Ligature points and ligature types used by psychiatric inpatients who die by hanging: a national study. Crisis. 2012;33(2):87-94.
Jorge V, Curet K, Aly R, Gupta S, Gupta S, Hares H. Safety of alcohol-based hand sanitizers in behavioral health facilities. Am J Med Qual. 2021;36(5):372.
Violation detail. Occupational Safety and Health Administration, US Department of Labor. Accessed April 11, 2023. https://www.osha.gov/ords/imis/establishment.violation_detail?id=1364614.015&citation_id=01001
Slemon A, Jenkins E, Bungay V. Safety in psychiatric inpatient care: the impact of risk management culture on mental health nursing practice. Nurs Inq. 2017;24(4):e12199.
Adame AL, Morsey M, Bassman R, Yates K. A brief history of the psychiatric survivor movement. In: Exploring Identities of Psychiatric Survivor Therapists: Beyond Us and Them. Palgrave Macmillan; 2017:33-53.
Hansen HB, Jackson JF. Addiction, drug policy, and black clinical innovations. In: Griffith EE, Jones BE, Stewart AJ, eds. Black Mental Health: Patients, Providers, and Systems. American Psychiatric Association Publishing; 2019:309-319.
Punishment and prejudice: racial disparities in the war on drugs: key findings at a glance. Human Rights Watch. Accessed April 11, 2023. https://www.hrw.org/legacy/campaigns/drugs/war/key-facts.htm
Dudley RJ Jr. African Americans and the criminal justice system. In: Griffith EE, Jones BE, Stewart AJ, eds. Black Mental Health: Patients, Providers, and Systems. American Psychiatric Association Publishing; 2019:65-76.
Redfield SE, Nance JP; American Bar Association Coalition on Racial and Ethnic Justice; Criminal Justice Section; Council for Racial and Ethnic Diversity in the Educational Pipeline. The American Bar Association Joint Task Force on reversing the school-to-prison pipeline preliminary report. Univ Memphis Law Rev. 2016;47:1-179.
Janofsky JS, Alampay M, Bonnie R, et al; Council on Psychiatry and Law. Position statement on weapons use in hospitals and patient safety. American Psychiatric Association; 2018. Accessed August 31, 2023. https://www.psychiatry.org/getattachment/1f8dec1d-380b-464e-98f6-a169821d8dfa/Position-2018-Weapons-Use-in-Hospitals-and-Patient-Safety.pdf
Mental Health Systems Act, 42 USC §§9401-9523 (1980).
Ulrich RS, Bogren L, Gardiner SK, Lundin S. Psychiatric ward design can reduce aggressive behavior. J Environ Psychol. 2018;57:53-66.



