Medicine and Society
Mar 2025
Peer-Reviewed
Surgeons might experience regret after interventions for high-risk patients who have poor outcomes, even when no errors occurred. Some regret experiences stem from incomplete communications or miscommunications about options, expectations, or prognoses. Experiences of regret, and even moral distress, might be mitigated when surgeons share key surgical care decisions with patients or their surrogates and draw on strategies for communicating well about patients’ serious illnesses or injuries. Shared decision-making is a communication framework whose principles may contribute to mitigation of surgeon regret.
Regret is a widely acknowledged yet poorly understood influence on health care decision-making. Regret can occur as a result of incomplete communications or miscommunications during the decision-making process, and it can potentially live on as a source of distress and bias in clinicians’ future decision-making conversations with other patients. Thus, regret can both result from the decision-making process and influence future clinical decisions. While decisional regret among patients is relatively well studied,1,2 there are few studies that assess factors that contribute to clinicians’ regret experiences.3,4 In high-stakes situations, surgical decision-making can be complex, and a poor outcome can have substantial consequences for surgeons, patients, and other key stakeholders in surgical decisions, even in the absence of error.
Surgeons may experience regret for different reasons in the setting of a poor outcome: because of the outcome itself, the clinical option chosen, the role they played, or the process through which a decision was made. Although these types of regret may be distinct, some are related to each other via common psychological mechanisms (eg, justification in the face of a poor outcome).5 Traditional discussions at morbidity and mortality conferences focus heavily on techniques utilized during surgery or on which option was chosen (ie, factors related to outcome regret and option regret) rather than on issues related to process or role regret. It is for these categories of regret that robust shared decision-making (SDM) may provide the most benefit.
SDM is a physician-patient communication process that emphasizes collaboration between patient and physician in reaching decisions. It is an increasingly utilized framework for decision-making in serious illness, including surgical situations. While robust SDM may not prevent a patient from having a poor outcome, I hypothesize that it might contribute to mitigating surgeon regret when poor outcomes do occur.
Studies of surgeon regret in surgical decision-making have focused on option regret. Some studies assessing surgeon regret utilize scales that classify regret as that of commission or omission.3,4 This classification breaks down regret by the decision that was made: regret of commission occurs as the result of a decision to perform surgery; regret of omission results from a decision against operative intervention. Regrets related to omission may be more difficult to study, as these cases are less likely to be presented at morbidity and mortality conferences or in written work submitted for peer review. This distinction is useful for organizing our thinking about situations in which regret can occur, but it relies on which decision was made and does not address process regret. It’s reasonable to believe that robust SDM may play a role in mitigating the degree of process-related regret and even moral distress that surgeons experience when poor outcomes occur.
The collaborative nature of SDM stresses placement of equal value on patients communicating values and goals and on physicians sharing information about clinical context, medical evidence, and expected outcomes. Together, a decision is made based on a mutual exchange of information among patient, family, physician, and other stakeholders involved in the decision.6 When studied in context of surgical decision-making, SDM has been shown to improve decision quality and patient preparation and to decrease conflict.7 Its impact on postoperative regret of patients or surgeons in the setting of a poor outcome, however, has not been well studied. Nevertheless, it stands to reason that engaging in a thorough SDM process may provide benefits in lessening the likelihood of surgeon regret in scenarios with a poor outcome. To understand why, we need to first think about what exactly SDM is, how it might differ from what we routinely do as part of surgical practice, and what impact this process could have on regret in the context of a poor outcome.
SDM has been summarized using a “three-talk model” consisting of team talk, option talk, and decision talk (see Figure).8 Team talk refers to the focus on making a team-based decision that incorporates informed goals and preferences of the patient in the context of the clinical scenario. Option talk refers to discussing alternatives to the surgical plan and thoroughly discussing the risks and likely outcomes of all possible choices. Decision talk integrates team and option talk to arrive at a preference-based plan. Throughout this process, active listening and deliberation are relied upon to arrive at a decision that integrates the surgeon’s best medical knowledge and the patient’s knowledge about their preferences and goals.8
Figure. Three-Talk Model of Shared Decision-Making
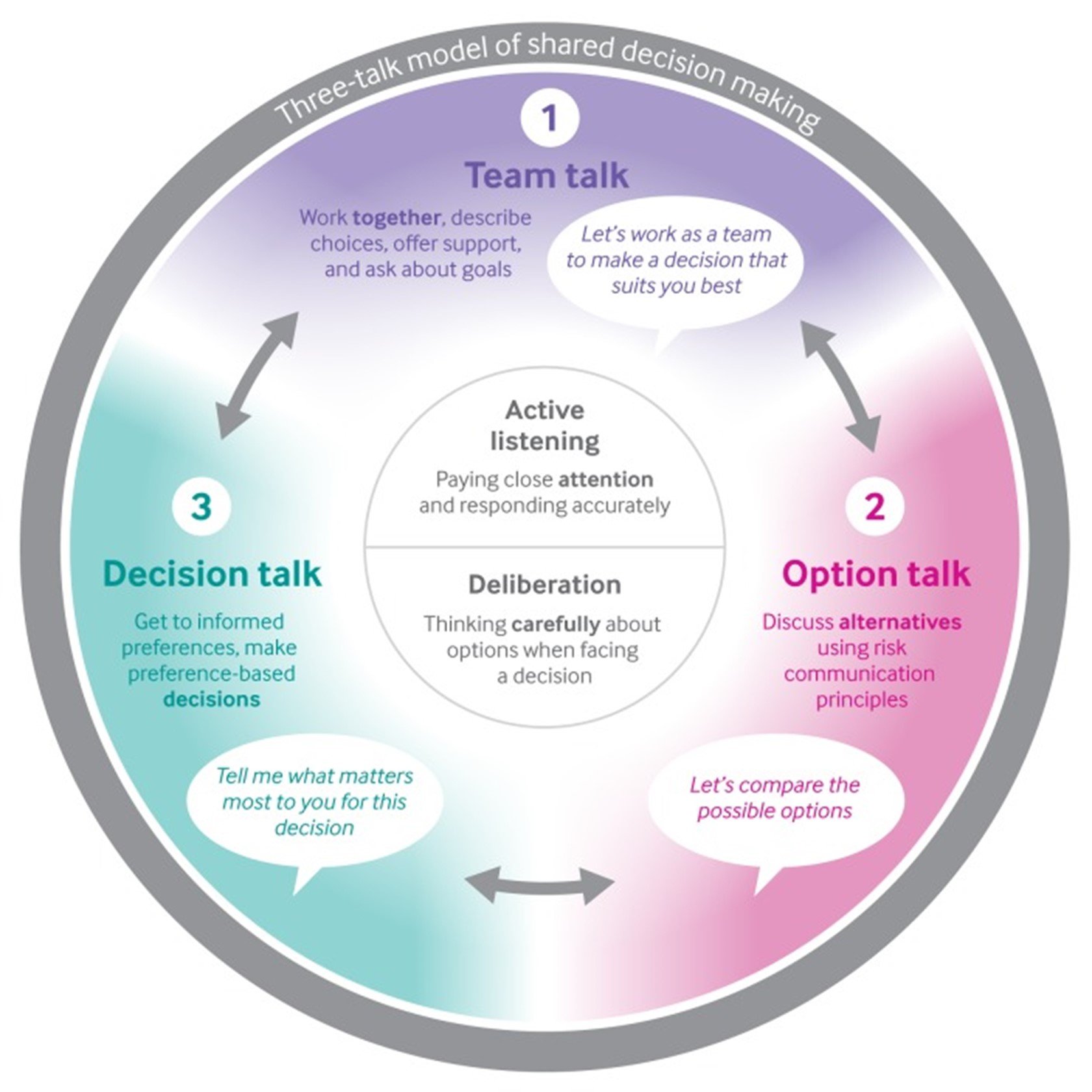
Reproduced from Elwyn G, Durand MA, Song J, et al.8 © 2017. Licensed under Creative Commons Attribution Noncommercial No Derivatives 4.0 International.
The SDM process differs from a more simplified model of surgical decision-making that involves discussing a diagnosis and proposed surgical treatment, along with risks and expected outcomes, and reliance on patients to make decisions based on that provided information. While on the surface this process aligns with the principle of respect for patient autonomy, it may not allow for truly informed decisions that account for both expected outcomes and patient goals. The three-talk model, which strives to create an equal playing field with all stakeholders, nevertheless may not completely equalize the power dynamic between patient and surgeon, and this fact should always be kept in mind while engaging in these discussions.9
To explore the relationship between decision-making and regret, we need to identify aspects of decision-making that could contribute to regret and how SDM could potentially address them.
Inadequate options talk. After a poor outcome, surgeons may regret not having fully discussed all options available to a patient and their likely associated outcomes, including nonoperative options. During a brief surgical visit, it has been shown that much time and effort is spent describing disease processes and technical aspects of procedures.10 This prioritization leaves less time to discuss the likely outcomes of nonsurgical alternatives and patient goals. In the setting of a poor outcome, it’s reasonable to believe that surgeons may regret not having spent more time discussing alternatives out of a desire to explain technical aspects of procedures and specific risks. A foundational aspect of SDM is option talk, which ensures that patients understand that there are options and that they have a choice between these options. While “best supportive care” is not an option many patients might end up choosing, the SDM model ensures that this option, as well as its consequences, are included in a decision-making discussion, in addition to other surgical and nonsurgical options. Direct discussion of this option could potentially contribute to mitigating surgeon regret in the setting of a poor postoperative outcome.
Inflated patient or family expectations. Surgeons can also experience regret in situations in which patient or family expectations are incongruent with those of the surgeon, and a complication or poor outcome occurs. In high-stakes situations, for example, a surgeon might believe that they have adequately communicated the high-risk nature of an intervention, but patients and families are caught off guard when a complication or poor outcome occurs. While using risk calculators and describing complications of surgery may create the impression that the downsides of surgery have been communicated, these tools may not fully impart to patients and families the realities of a poor outcome. The SDM model necessitates creating space for narrative descriptions of life after the different options discussed, which can better allow patients to understand likely outcomes. This approach contrasts with other communication methods that might rely on numbers and percentages to convey surgical risk. Some approaches that have been described to assist in creating such narrative descriptions are Best Case/Worst Case11 and presenting patients with the comprehensive “downsides” of surgery rather than just the risks.12 The Best Case/Worse Case communication tool involves describing for both surgical and nonsurgical options the range of outcomes that may occur (in real-life, narrative terms) and creating a visual tool for the patient that locates the “most likely” outcome on a spectrum for each option. The visual tool is given to the patient and family while they deliberate and can be referred to later. This communication tool, as modeled in a whiteboard video,13 expands on the three-talk model previously discussed. Following an SDM model of communication that includes tools such as Best Case/Worst Case likely will lead to patient and family expectations that are more congruent with the option chosen, which intuitively might mitigate regret that follows a poor outcome.
Patient’s or family’s desire for futile aggressive treatment. Finally, surgeons may experience regret after a poor outcome if, during the decision-making process, the patient or family had expressed a strong desire for aggressive treatment or that they wanted “everything done,” even in the setting of a poor prognosis. Specifically, surgeons might experience not only regret but moral distress14 if they feel they have been pressured to provide treatment they knew would not end well or if they did not adequately—or in enough detail—outline the downsides of treatment. In these situations, applying the SDM framework can facilitate decision-making in a number of ways. First, the SDM framework naturally provides opportunity to avoid the description of options as “everything or nothing,” with “everything” possibly corresponding to a major operation and “nothing” to best supportive care. Presenting all options (including best supportive care) as detailed narratives allows patients to fully appreciate the benefits and downsides of those choices. Most patients, unsurprisingly, will not opt for medical care described as “nothing.” Besides creating space for thorough discussion of options, the team talk component of SDM creates a natural alliance between the patient and surgeon so that discussions of options can occur in the context of goal alignment. Discussion of multiple options and whether they align with patient goals can minimize the extent to which surgeons might feel they are being pushed towards a specific choice. If the patient’s goals are aligned with the chosen option, even in the setting of a poor outcome, regret (and even moral distress) may be dampened by having followed this process.
Ultimately, it is likely not possible to eliminate surgeon regret following the poor outcome of a patient, even in absence of error. The time and emotion that surgeons dedicate to patients makes it reasonable to feel regret in these situations. It is reasonable to imagine, however, that aligning surgical decisions with patients’ goals and values can minimize the regret experienced when things go poorly. This approach in particular would minimize regret about the decision-making process, which can be considerable in high-stakes situations. SDM provides an established model to maximize the alignment of decisions with patients’ goals and values. While further study is needed to determine what communication models best protect surgeons from decisional regret, there is ample evidence that the SDM model provides an ideal framework.
Lunger L, Meissner VH, Kopp BCG, et al. Prevalence and determinants of decision regret in long-term prostate cancer survivors following radical prostatectomy. BMC Urol. 2023;23(1):139.
Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891.
Campbell T. Best Case/Worst Case (BC/WC) SURGEON communication tool—whiteboard video. Patient Preferences Project. Accessed October 22, 2024. https://www.youtube.com/watch?v=FnS3K44sbu0

