Case and Commentary
Aug 2022
Peer-Reviewed
Some clinical algorithms use race as an epidemiological shorthand to “correct” for health determinants that are clinically influential but also variable because they are historical, social, cultural, or economic in origin. Such “correction factors” are both clinically and ethically relevant when their use reinforces racial essentialism and exacerbates racial health inequity. This commentary on a case in which the original vaginal birth after cesarean calculator is used argues that this and similar race-based algorithms should be considered sources of iatrogenic harm by undermining decision sharing in patient-clinician relationships and Black birthing peoples’ rights to self-determination.
Dr OB is a resident physician in a high-volume obstetrics unit at a county hospital serving predominantly Black and urban Indigenous community members. Like other resident physicians, Dr OB often uses a mobile phone application to calculate, via algorithm, vaginal birth risk for birthing people who have delivered a prior child via cesarean section (C-section).1 This vaginal birth after cesarean (VBAC) calculator has 2 race-based correction factors.1 Scores yielded by the calculator are used to inform clinical management decisions—specifically, about which delivery options to offer patients in the unit—and to motivate standard of care. For individuals who have delivered by C-section before, the score is clinically and ethically important, since vaginal delivery complication risk for a person who has had a C-section is lower than C-section delivery complication risk for a person who has had a C-section. Strangely, though, Dr OB notices that most patients in the unit who have had a C-section are not offered an option to attempt labor and vaginal delivery.
Dr OB enters a patient’s race as White instead of Black a few times and notices score changes substantial enough to influence whether a patient who has had a C-section will be offered an option to try labor and vaginal delivery. Dr OB wonders about the validity of the VBAC calculator’s “correction” factors in light of such starkly different results based on how a clinician perceives and enters a patient’s race.
Given C-sections’ higher risk of morbidity and mortality and of longer stay in the intensive care unit,2 Dr OB worries that patients of color in the unit are more frequently exposed to higher-risk deliveries than White patients. Structural determinants of health, such as systemic racism, which are independent risk factors in maternal mortality and morbidity3 when other factors such as socioeconomic status4 are controlled for, are widely documented as exacerbating racial health inequity. In light of long-standing high rates of maternal mortality in the United States5 compared to other high-income countries, and in light of Black patients suffering stark inequity in childbirth-related mortality within the United States,6 Dr OB wonders what to do.
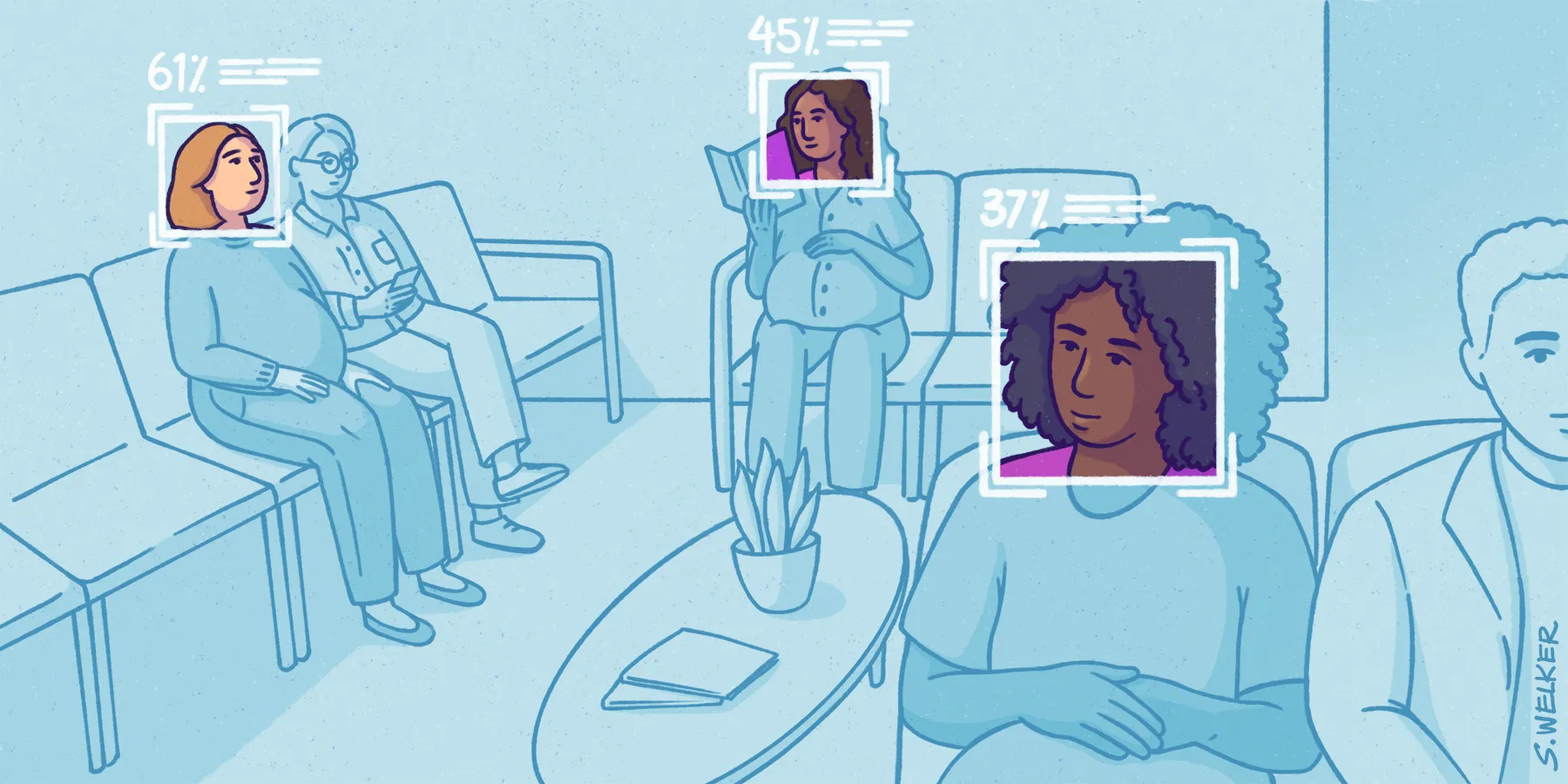
The trial of labor after C-section (TOLAC) decision should be a clinically nuanced and patient-centered process that balances the increased mortality and morbidity risk associated with VBAC with the major surgical risk of repeat C-section. As Dr OB notes, racial inputs to the original VBAC calculator significantly alter risk assessment and can be used to systematically route Black and Latine patients towards repeat C-sections at higher rates than White patients. (We use the term “Latine” as a gender-neutral form that was developed within Latine/Hispanic communities to describe people of Latin American and/or Spanish descent.7,8) For example, for patients with matched profiles (eg, 28 years of age, body mass index of 26, and “prior indication for cesarean”), a White patient would have a 61.6% chance of successful VBAC, whereas a Black patient would have a 45.1% chance of successful VBAC and a Latine patient, 44.9%.1 Of note, the original VBAC calculator lacks definitions of (and distinctions between) racial and ethnic identity. Physicians are further unable to select “yes” for both African American and Hispanic, creating conundrums for biracial, multiracial, and Afro-Latine individuals.1
Choosing between a C-section or vaginal delivery can be deeply personal, and both options come with benefits and risks. Adverse C-section outcomes include protracted hospital stay, increased financial costs, and poorer patient outcomes.1,2,9,10 Moreover, TOLAC increases risk of uterine rupture (though absolute risk remains low) and morbidity from repeat C-section after a failed TOLAC11; long-term concerns after vaginal birth include urinary incontinence, uterine prolapse, and pelvic pain.9
The race-based VBAC calculator, however, does not address racialized inequities in childbirth-related morbidity and mortality. It instead embeds multiple invalidated assumptions and omits critical nuance, and its use risks removing patients’ exercise of their autonomy in an informed decision on method of delivery. Race is either falsely assumed to be an immutable biological characteristic or implemented as an overly imprecise proxy for the lived consequences of structural racism. Ultimately, this unscientific rationale places patients of color at disproportionate surgical risk, which is discriminatory and causes iatrogenic harm. Accordingly, the VBAC calculator was recently revised12 to remove race (though the new calculator’s implementation is still ongoing). The use and reform of the race-based VBAC tool demonstrates the necessity of critical inquiry in shifting to a race-conscious paradigm emphasizing racism-based structural determinants of health.13,14,15,16
Racial categorization is a historical, imperial, and erroneous enterprise. While human difference has long been scrutinized, hierarchical racial organization of humans originated from colonial efforts to subjugate people of color.17 Medical professionals published pseudoscientific racial rankings, baldly motivated by economic gain, White supremacy, and racist colonial agendas.17,18,19 Bolstered by the authority of Western biomedicine, dehumanizing conclusions about racial inferiority were widely adopted in medical scholarship and served as foundations for racial adjustments. Race was thereby operationalized as an immutable, physiological trait despite lack of evidence of a genetic basis.18,20,21
Furthermore, medical education presumes that the typical patient is White (and often able-bodied, slim, and cis-male).18,22,23,24,25 This logic frames people of color as abnormal human variants, whose manifestations of health and illness require “corrections.” Using tools with race-based corrections can lead to delayed care, unequal treatment, and personal and systemic biases.15 Fundamentally, it is unscientific and unethical to correct for race in any clinical algorithm.
Importantly, biological essentialism frames racial genetic variation as the source of health inequities, despite ample evidence demonstrating that structural racism is a major contributor to health injustice.3,13,20,21,26,27 Nonetheless, extensive resources are allocated to investigate how genetics contributes to racial differences in disease rates and mortality, while funding for investigations that seek to examine and address the social realities that beget unequal health remains sparse.28,29,30 This funding disparity leads to low-quality scholarship that prevents and muddies broader comprehension while overlooking opportunities to unravel the complex threads of structural power that bar patients of color from healthier lives.
A structurally just algorithm would prioritize upstream causes of social inequity that can be readily defined, measured, and addressed.
Interdisciplinary scholarship has identified key intersecting drivers of inequities ranging from life-long toxic exposures, epigenetic and hospital-level risk factors, and the impact of structural racism.3,31 For instance, the authors of the original VBAC calculator analyzed but did not include insurance status,1,32 which is associated with successful VBAC for privately insured patients.33 Because structural racism causes access to private insurance to fall along racial lines,34 utilizing race but not insurance in VBAC possibly exacerbates bias. Using race as a stand-in for such interlocking factors is an overly crude tool in research on root causes of childbirth disparities and morbidity and mortality, let alone in nuanced clinical decision making to address such suffering.
As discussed above, the unscientific use of race causes patient harm by systematically increasing risk for Black and Latine patients. It also reinforces racist notions by casting birthing people of color as fundamentally different from White birthing people, echoing racist medical legacies that ascribed differing pelvic anatomy and reproductive “fitness” to Black and Latine patients.1 Using race thus perpetuates medical othering without elucidating actionable factors of VBAC disparities.
Neglect of patient autonomy and consent is another source of harm. Fundamentally, physicians must inform patients of the risks, benefits, and reasonable alternatives (including no intervention) to make their own decision.35 Although the American College of Obstetricians and Gynecologists recommends implementing shared decision making for VBAC,11 the determination and application of race is often done without patient knowledge, let alone patient input or consent. This neglect of patient autonomy reenacts historical legacies of medical disenfranchisement in communities of color, highlights physician paternalism, and infringes upon basic patient rights. Rather than assigning race or engaging in “colorblind” medicine that disregards race and racism, clinicians should prioritize respect for autonomy and shared decision making to enable race-conscious medicine that emphasizes racism.14 This approach should facilitate transparent discussion of patient values and preferences about TOLAC in the context of the effects of structural racism on their bodies, environments, and hospital care.
It is also necessary to consider the harm of the unscientific use of race to clinicians and the greater society. Teaching clinicians to believe in the fundamental biological inferiority of non-White bodies creates inappropriate, harmful, and unscientific clinical practice. Such a belief renders invisible the toll of structural racism, hinders shared decision making and health equity, and exacerbates injustices that plague already-oppressed populations. Clinicians and trainees of color often bear “chronic minority stress” and can be additionally harmed by internalizing false bioessentialist claims.36
Structural justice requires that health care organizations “acknowledge and work to reduce the inequities in society.”37 A structurally just algorithm would prioritize upstream causes of social inequity that can be readily defined, measured, and addressed (eg, insurance status). Critically examining race-based instruments disrupts structural racism’s power. Although race-based adjustments seem to address racial disparities, they perpetuate damaging bioessentialist perspectives of race, are fundamentally nonspecific because they do not define or capture clinically meaningful variables, and intrinsically reinforce White supremacy to our patients’ detriment. When race-based tools perpetuate health inequities and cause potential iatrogenic harm, we must then practice race-conscious medicine that emphasizes structural justice by analyzing disparities’ root causes and materially addressing them.
While African American and Latine patients have decreased rates of successful VBAC in comparison to White counterparts, this disparity is not because of their genetic code but because of historical and contemporary inequities, as the toll of COVID-19 attests.38,39,40,41 In this respect, race certainly still matters. As social inequities regarding insurance, access to care, educational level, and financial support also affect rates of successful VBAC, these factors could be explored during prenatal care or family planning to more precisely redress inequities.1 Shifting to race-conscious medicine that emphasizes racism (which requires working with advocates, system-level administrators, and community organizations; addressing the structural justice and societal-level circumstances; and critically examining childbirth-related morbidity and mortality) represents a better and more concrete step towards redressing structural racism. Because no individual clinician can compel these reforms, collaboration is crucial.
In the meantime, clinicians should eschew racialized corrections in individual practice and instead name racism—not race—as a marker in health inequities. Continuing education on race, racism, and race-based medicine is necessary. We invite clinicians to thoughtfully reflect on What happens if I remove this race adjustment? What factors of social injustice are contributing to this assessment? What additional factors may be relevant? Such queries remind us that unilaterally assigning race based on phenotype or participating in colorblind medicine (ie, ignoring race) are baseless behaviors. Rather, firmly repositioning patients as the foremost experts on their illnesses, histories, and lives bolsters shared decision making and patient autonomy. These shifts can improve patient discussions and encourage clinical practice tools to incorporate markers of structural violence while helping clinicians make thoughtful and informed clinical decisions.14,42
Creating alternatives to racial categories will require significant effort. Professional organizations must reform race-based guidelines, and researchers across allied health fields must innovate and implement measures of structural harms. Institutions must also address the time and financial pressures in clinics, which reward heuristics and limit clinicians’ ability to have nuanced, structurally informed encounters. These constraints most affect underserved patients, whose social realities and resulting comorbidities often require time-intensive efforts to address in order for clinicians to confer high-quality care.
Although there are significant obstacles to race-conscious medicine that emphasizes racism, we remain hopeful about progress. We have witnessed recent professional consensus eliminating race-based corrections in VBAC and kidney function tests,11,43,44 and we are inspired by new research demonstrating racism as a cause of downstream factors that contribute to preterm birth.45 These advances have been achieved through collaboration and tireless advocacy and should be a blueprint for the reform of other tools.
In sum, we recommend that clinicians engage in transdisciplinary collaboration to do the following26:
We suggest implementing these recommendations in transdisciplinary collaboration within and beyond academic health care settings.
Yan Liu S, Fiorentini C, Bailey Z, Huynh M, McVeigh K, Kaplan D. Structural racism and severe maternal morbidity in New York State. Clin Med Insights Womens Health. 2019;12:1179562X1985477.
Bishop-Royse J, Lange-Maia B, Murray L, Shah RC, DeMaio F. Structural racism, socio-economic marginalization, and infant mortality. Public Health. 2021;190:55-61.
Duclercq E, Zephyrin L. Maternal mortality in the United States: a primer. Commonwealth Fund. December 16, 2020. Accessed March 14, 2022. https://www.commonwealthfund.org/publications/issue-brief-report/2020/dec/maternal-mortality-united-states-primer
Odegard Pereira E. For most Latinos, Latinx does not mark the spot. New York Times. June 15, 2021. Accessed April 25, 2022. https://www.nytimes.com/2021/06/15/learning/for-most-latinos-latinx-does-not-mark-the-spot.html
Noe-Bustamante L, Mora L, Hugo Lopez M. About one-in-four US Hispanics have heard of Latinx, but just 3% use it. Pew Research Center. August 11, 2020. Accessed April 25, 2022. https://www.pewresearch.org/hispanic/2020/08/11/about-one-in-four-u-s-hispanics-have-heard-of-latinx-but-just-3-use-it/
Keag OE, Norman JE, Stock SJ. Long-term risks and benefits associated with cesarean delivery for mother, baby, and subsequent pregnancies: systematic review and meta-analysis. PLOS Med. 2018;15(1):e1002494.
Martin JA, Hamilton BE, Osterman MJ, Driscoll AK. Births: final data for 2019. Natl Vital Stat Rep. 2021;70(2):1-50. Accessed April 25, 2022. https://www.cdc.gov/nchs/data/nvsr/nvsr70/nvsr70-02-508.pdf
Vaginal birth after cesarean delivery. ACOG Practice Bulletin No. 205. Obstet Gynecol. 2019;133(2):110-127.
Vaginal birth after cesarean calculator. Version 2.0. Maternal-Fetal Medicine Units Network. Updated May 2021. Accessed March 21, 2022. https://mfmunetwork.bsc.gwu.edu/web/mfmunetwork/vaginal-birth-after-cesarean-calculator
Chadha N, Lim B, Kane M, Rowland B. Toward the abolition of biological race in medicine. Institute for Healing and Justice in Medicine; Othering & Belonging Institute; 2020. Accessed April 25, 2022. https://static1.squarespace.com/static/5e94e4feaa92821de07e3682/t/5f0b40ab2d6235002617d565/1594572974864/Toward+the+Abolition+of+Biological+Race+in+Medicine+FINAL.pdf
Smith J, Spodak C. Black or “other”? Doctors may be relying on race to make decisions about your health. CNN. June 7, 2021. Accessed April 25, 2022. https://www.cnn.com/2021/04/25/health/race-correction-in-medicine-history-refocused/index.html
Omi M, Winant H. Racial formations. In: Racial Formation in the United States: From the 1960s to the 1990s. Routledge; 1994:3-13.
Roberts D. Fatal Invention: How Science, Politics, and Big Business Re-create Race in the Twenty-First Century. New Press; 2011.
Curran AS. The Anatomy of Blackness: Science and Slavery in an Age of Enlightenment. Johns Hopkins University Press; 2013.
Anonymous. “White” should not be the medical standard. Doximity Op-Med. July 20, 2020. Accessed March 21, 2022. https://opmed.doximity.com/articles/white-should-not-be-the-medical-standard?_csrf_attempted=yes
Parker R, Larkin T, Cockburn J. A visual analysis of gender bias in contemporary anatomy textbooks. Soc Sci Med. 2017;180:106-113.
Collins FS. Report of the Director, National Institutes of Health: Fiscal Years 2016-2018. Division of Program Coordination, Planning, and Strategic Initiatives, National Institutes of Health. Accessed April 25, 2022. https://dpcpsi.nih.gov/sites/default/files/NIH-Triennial-Report-FY-2016-2018_Final508.pdf
Grobman WA, Lai Y, Landon MB, et al; National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU). Development of a nomogram for prediction of vaginal birth after cesarean delivery. Obstet Gynecol. 2007;109(4):806-812.
Artiga S, Hill L, Orgera K. Health coverage by race and ethnicity, 2010-2019. Kaiser Family Foundation. July 16, 2021. Accessed April 25, 2022. https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-coverage-by-race-and-ethnicity/
Sedig L. What’s the role of autonomy in patient- and family-centered care when patients and family members don’t agree? AMA J Ethics. 2016;18(1):12-17.
DiChristina WD. Structural justice ethics in health care. Voices in Bioethics. 2021;7:10.52214/vib.v7i.8404.
Phillips J, Peck Malliaris A, Bakerjian D. Nursing and patient safety. PSNet. Updated April 21, 2021. Accessed April 25, 2022. https://psnet.ahrq.gov/primer/nursing-and-patient-safety
Byrd WM, Clayton LA. An American Health Dilemma: A Medical History of African Americans and the Problem of Race, Beginnings to 1900. Routledge; 2000.
Braveman P, Dominguez TP, Burke W, et al. Explaining the Black-White disparity in preterm birth: a consensus statement from a multi-disciplinary scientific work group convened by the march of dimes. Front Reprod Health. 2021;3:684207.



