In the Literature
Jul 2024
Peer-Reviewed

Overall rates of opioid use are low in adolescents; however, recent increases in mortality from overdose in adolescents have outpaced increases in the general population. This article highlights the importance of expanding evidence-based treatment for adolescent opioid use, especially medication, while also addressing key ethical considerations of harm reduction practices and how application of such practices with adolescents may differ from adults. Concepts related to adolescent populations are discussed, including autonomy, confidentiality, and brain development. Application of harm reduction practices should be age appropriate, express respect for patients’ autonomy, include social support, and be accompanied by broader aims to minimize adolescent initiation, escalation, and overall harm caused by opioid use.
The opioid crisis has had a profound influence on individuals, families, and communities throughout the United States. Increasing rates of overdose deaths—fueled largely by fentanyl and by the simultaneous use of other substances, including stimulants—are alarming.1,2 Yet overdose deaths represent only a fraction of the all-cause mortality and devastation caused by opioid use disorder (OUD).3,4,5 Harm reduction represents a promising approach to limiting the morbidity and mortality associated with OUD, a disorder recognized as a disease and condition in need of treatment.6,7 Harm Reduction International defines harm reduction as “policies, programmes and practices that aim primarily to reduce the adverse health, social and economic consequences” of substance use,8 and, as others have noted, it focuses on “the prevention of harm, rather than on the prevention of drug use itself.”9 The Substance Abuse and Mental Health Services Administration (SAMHSA) includes “prevention, risk reduction, and health promotion” as key aspects of harm reduction and further specifies that, within a harm reduction framework, “abstinence is neither required nor discouraged.”10
Questions remain on how harm reduction efforts for people who use drugs (PWUD) should be applied to adolescents (here defined as those under the age of 18). Abstinence has long been the preferred approach, with public health efforts promoting “just say no” to practices other than prevention. There is a complete prohibition of sales of alcohol, tobacco, and cannabis (where legalized) to individuals under the age of 21 in the United States.11,12,13 Despite these and other efforts to promote abstinence and prevention, many youth access and use substances, with the annual 12th-grade prevalence of alcohol use at 51.9%, vaping at 32.1%, and illicit substance use at 32.6% (8% when cannabis is excluded) in 2022 in the United States.14
By contrast, rates of opioid use are low in US adolescents, with 1.9%, 0.9%, and 0.7% of 12th, 10th, and 8th graders, respectively, reporting oxycodone misuse and 0.3%, 0.2%, and 0.3% of 12th, 10th, and 8th graders, respectively, reporting heroin use in 2022.14 However, national trends in adolescent overdose fatalities have shown a rapid increase in recent years (see Figure), with a disproportionate increase in overdose fatalities between 2020 and 2021 among adolescents aged 14 to 18 relative to the general US population (20% vs 11.5%).1 Seventy-seven percent of the overdose fatalities in US adolescents in 2021 involved fentanyl,1 which is higher than the estimated 66% of all overdose deaths for synthetic opioids (primarily fentanyl) for all ages.15 Of concern, many of these overdose fatalities are due to unintentional exposure to fentanyl by adolescents intending to misuse other substances.1
Figure. Total Number of Drug-Related Overdose Deaths of US Youths by Age, 2000 to 2021
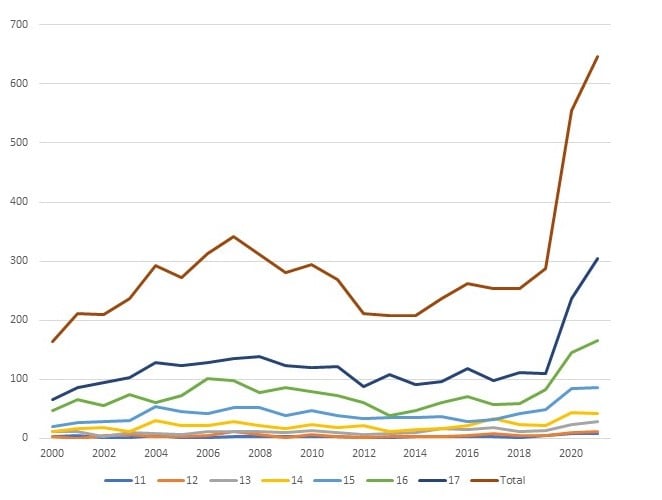
Data source: Centers for Disease Control and Prevention WONDER (Wide-Ranging Online Data for Epidemiologic Research) database.
These data indicate a need for a thoughtful and comprehensive approach to adolescent opioid use beyond just prevention or abstinence. While we will limit our discussion to harm reduction as it applies specifically to opioid use and OUD within this population, we recognize that opioid use represents a small percentage of overall substance use in this age group and that some of the principles discussed are applicable to other substances, as discussed in recent papers.16,17
Multipronged approach needed. Adolescence is a period of high neuroplasticity and rapid neurodevelopment through synaptogenesis, dendritic and synaptic pruning, progressive and differential myelination, and neurotransmitter-specific changes that are influenced by the complex interplay of genetics, epigenetics, and environmental factors.18,19 These changes contribute to developmentally appropriate (and necessary) strengths, as well as vulnerabilities, including risk-taking, novelty seeking, higher salience of emotions and sensations, impulsivity, and greater peer influence.18,20 These changes also make adolescents particularly vulnerable to experimentation and the associated euphoria of substance use while having decreased ability to consider negative outcomes. The developing adolescent brain is also uniquely susceptible to the building and reinforcing of unhealthy neural circuitry.18,21 Earlier substance use is correlated, among many other negative outcomes, with a higher likelihood and severity of later substance use disorders.22 Due to these particular vulnerabilities, ethically, as health care professionals, we should acknowledge that the best developmental outcomes occur with abstinence from all substances, that limited use is better than regular use, and that treatment is preferable to harm reduction alone. Thus, one ethical imperative in addressing adolescent substance use is an even greater emphasis on prevention of and reduction in use than on reduction in harm.
Harm reduction. Given the relatively small number of adolescents who have used opioids,14 there is little data on the efficacy of harm reduction strategies specific to this age group. The potential benefits of many of the most common harm reduction approaches are universal, and evidence supporting their use can be generalized to youth (eg, regardless of age, naloxone is effective for opioid overdose reversal, and sterile syringes have decreased risk of infection). In tandem with these efforts, youth should be encouraged to participate in evidence-based treatment (ie, medication for opioid use disorder [MOUD], including buprenorphine and naltrexone), although treatment should not be a requirement for accessing harm reduction services. Additionally, widespread implementation of harm reduction interventions for adolescents has significant potential to diminish disparities in access to MOUD based on minoritized group, socioeconomic, and demographic statuses. Street-involved youth represent a particularly vulnerable group that benefits from expanded harm reduction efforts.23,24,25,26
While employing harm reduction practices for the protection and benefit of members of the highest-risk population—adolescents who use opioids—it is imperative to avoid harming or increasing risk for others. Specifically, while providing harm reduction to adolescents in need, it is important to consider if such efforts might encourage or escalate use in both those seeking services and their peers. Harm reduction practices might be perceived by youth as condoning use and consequently lead to greater experimentation or continued use. Specific supplies, such as sterile syringes, might lead youth to perceive substance use as less risky and thereby increase it. These theoretical risks are worthy of rigorous study; however, just as in adults, so in adolescents, inaction is leading to actual harm through the spread of infections and death.
Some may worry that one mechanism by which harm reduction can lead to escalation of adolescent substance use is via the diminished perception of risk. Several large data sets and individual studies have demonstrated an inversely proportional relationship between perceived risk and experimentation with or regular use of substances among adolescents.17,27 However, there are limited data on the direct impact of harm reduction practices on adolescent perception of risk. One study showed that a higher proportion of youth (ages 14 to 16) reported seeing PWUD at a needle exchange program as a deterrent rather than an incitement to use (46% vs 11.1%, with 42.4% saying it had no effect).28 In an older study among youth (ages 13 to 23) who inject drugs, most reported that they did not believe that needle exchange programs led to earlier intravenous (IV) use, increased frequency of IV use, or decreased treatment-seeking behaviors.29 Of note, it is not known how harm reduction practices tailored to adolescents would affect their perception of risk or actual use of substances. Ongoing research is needed to evaluate the impact of the availability of harm reduction services on youth substance use, especially when these harm reduction strategies are accompanied by robust treatment options and evidence-based prevention strategies.
The use of harm reduction strategies with adolescents is significantly different than with adults concerning the principle of autonomy. Autonomy has been defined as “the obligation to respect the actions of persons and valuing informed voluntary consent, confidentiality and privacy.”30 Inherent in this definition is the expectation that an individual has the capacity—ethically, developmentally, and legally—for informed consent. In our current health care and legal systems, capacity to make one’s own decisions is an age-based construct barring any gross deficits or court-ruled limitations. Neuroscience and developmental theory teach that capacity for decision-making evolves through childhood and into adulthood. While some “as young as 14 can understand medical information” to the point of making an informed decision,31 each individual’s developmental trajectory is subject to biological and environmental influences, thus confounding the idea that a single age confers decision-making readiness. Should we then restrict autonomy to choose treatment or harm reduction for someone of a certain age who has already exercised that autonomy to choose substance use?
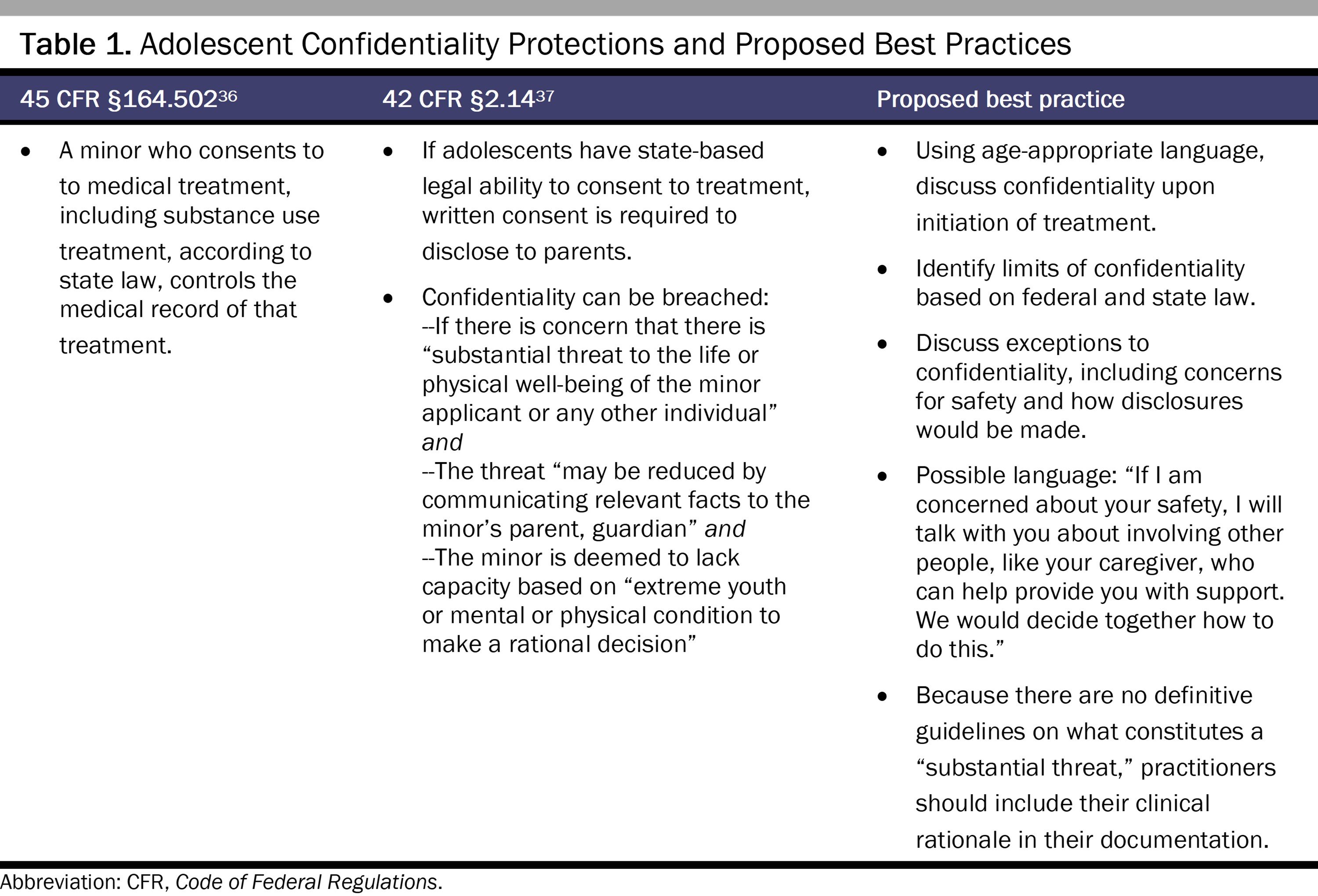
It is beyond the scope of this article to provide a complete overview of the complexities of adolescent consent and confidentiality laws, which vary widely by state. Most states allow for adolescent consent for some specified medical, mental health, or substance use treatment,32 even while 48 states recognize 18 as the age of majority.32 These statutes are meant to encourage youth to access needed care, increase engagement, allow the confidence and trust necessary for full disclosure, and create a more meaningful therapeutic relationship.33,34 State laws permitting minors to consent to substance use treatment vary based on age (12 to 16 or unspecified), the allowable location of treatment (inpatient or outpatient), and the types of treatment provided (medical or nonmedical).35 Some states require parents to consent to inpatient or outpatient substance use treatment for their children.35 State medical societies, other organizations (eg, the Center for Adolescent Health and the Law), and published articles can provide additional information on state-specific policies.32,35 Practitioners should be aware of state-specific laws governing substance use treatment and harm reduction strategies for adolescents. They should also be aware of confidentiality laws and best practices related to adolescent substance use treatment (see Table 1).
With legal and clinical efforts often focused on the autonomy and confidentiality of adolescents, parents, guardians, and other caregivers (hereafter referred to as parents) can be left with a sense of powerlessness in helping promote abstinence and safety for their teens. Although parents have a legal and moral responsibility to provide for the health and well-being of their children, they often are unable to prevent or control their children’s substance use. Nevertheless, adolescents’ perception of parental monitoring is associated with lower rates of substance use,38 and family-based treatment has a strong evidence base.39,40 Efforts should be made by clinicians to work with adolescents to engage supports, including parents. Once parents are part of treatment, tension may arise regarding types of treatment, location of treatment, and primary treatment goals. Depending on the state, parental consent may be needed to provide harm reduction measures or treatment for OUD. Clinicians need to be aware that because adolescents may primarily seek harm reduction and parents may only be interested in abstinence, additional work may be needed to help patients and families align their goals.
While not specifically harm reduction, MOUD represents one of the best treatment tools to reduce risks of substance use in adolescents with OUD.16,41,42 There is substantial evidence of the effectiveness of MOUD in adults and growing evidence of its effectiveness in adolescents; buprenorphine is approved by the US Food and Drug Administration (FDA) for those 16 years and older, and naltrexone is FDA approved for adults 18 years and older.43 It is essential to expand access to MOUD for adolescents with moderate or severe OUD by increasing the comfort and willingness of clinicians to prescribe to adolescents of any race or ethnicity.44 Despite increasing rates of opioid overdose deaths among adolescents (see Figure), recent data have shown that buprenorphine prescribing to youth decreased from 2015 to 2020.45 Clinicians interested in prescribing MOUD can access resources on education and on peer supervision and mentorship at the Providers Clinical Support System, a program funded by SAMHSA.46
Naloxone is a lifesaving medication to which adolescents who use substances, including opioids, and those who care about them should have easy access. Given adolescents’ high risk for unintentional and intentional exposure to fentanyl,1 all clinicians who work with adolescents who use substances should prescribe, provide, or educate on how to obtain naloxone.47 In March 2023, the FDA approved over-the-counter naloxone nasal spray,48 which has increased access throughout the country for patients and families. Accordingly, patients, families, and friends should be educated on symptoms of overdose and administration of naloxone, as is done in Massachusetts.49 Recently, the American Medical Association adopted a resolution to back making naloxone available to teachers, staff, and students and to remove barriers for youth to carry naloxone.50 Education on the important role naloxone plays in decreasing the risk of fatal overdose not only saves lives but also provides an opportunity to emphasize the risk associated with using substances alone and provides additional resources to mitigate that risk, such as never-use-alone hotlines.
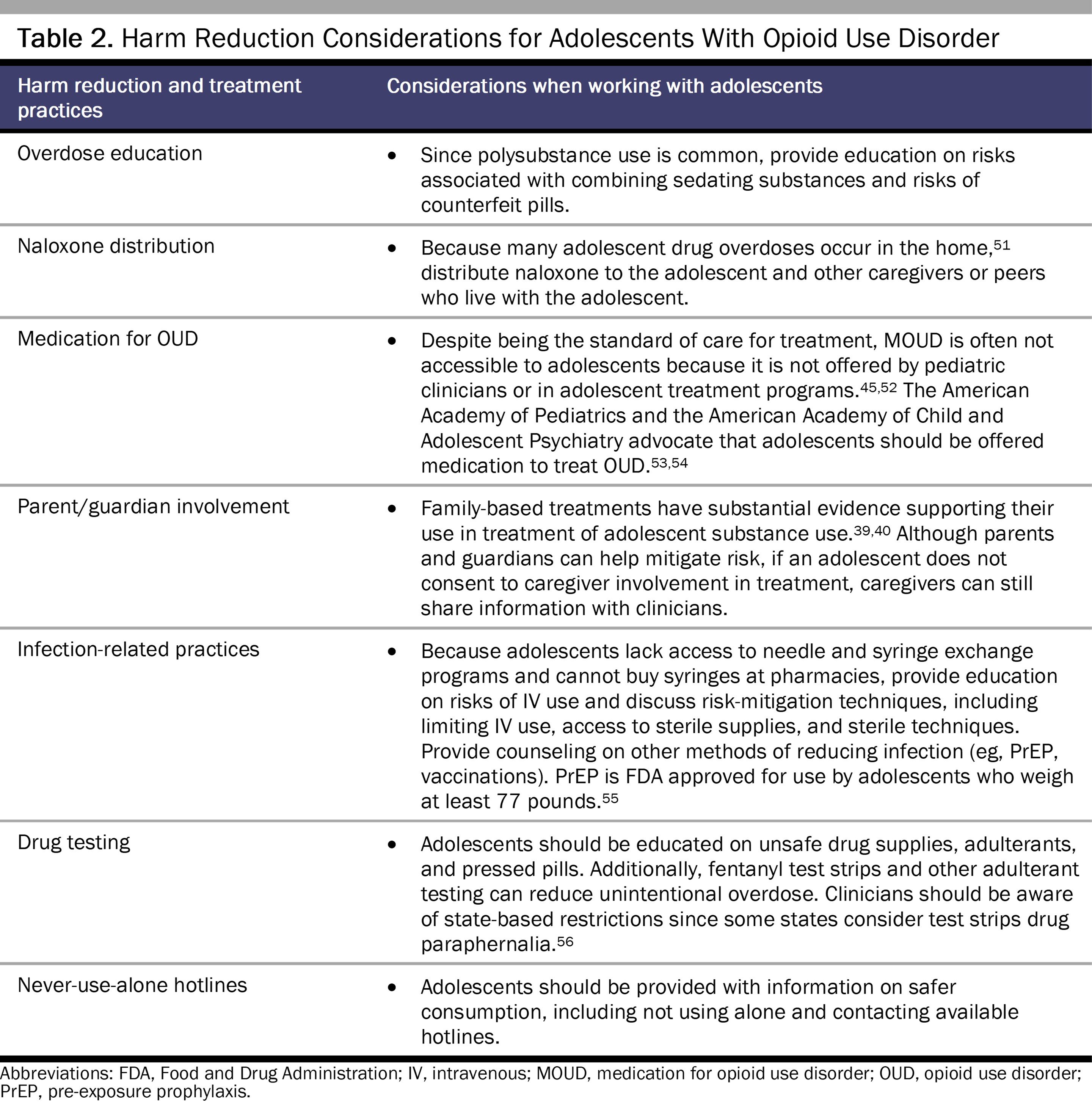
Youth should also be educated on the risks associated with specific use patterns and be provided with guidance and tools to mitigate that risk. Discussion of safety should cover risks associated with current use patterns and potential escalation of use (eg, IV use), as well as methods (and their availability) to mitigate risk. Clinicians should be clear that the safest approach is abstinence, while also providing additional information that aligns with patients’ goals and priorities and facilitating open communication. In providing this education, it is important for clinicians to be aware of local laws that may limit access to specific harm reduction strategies or require parental consent and thereby limit confidentiality. In addition to providing education and information on obtaining supplies, within the local legal limits, clinicians should consider providing clinically indicated harm reduction materials to adolescents (eg, fentanyl test strips, xylazine test strips, naloxone nasal spray, safe injection supplies).
Table 2 summarizes harm reduction practices relevant to adolescents with OUD.
Clinicians and organizations should approach adolescents with respect for their autonomy and with a clear understanding of the benefits and potential harms associated with treatment and harm reduction. Optimal clinical care should be nonjudgmental and seek to include and expand natural supports. A successful encounter may have less to do with sobriety and more to do with engagement and patient-centered care. Additionally, clinicians are uniquely positioned to discuss confidentiality with adolescents and to find ways to encourage engagement of families in harm reduction and treatment. Family-based approaches represent some of the strongest evidence-based treatments for adolescents.
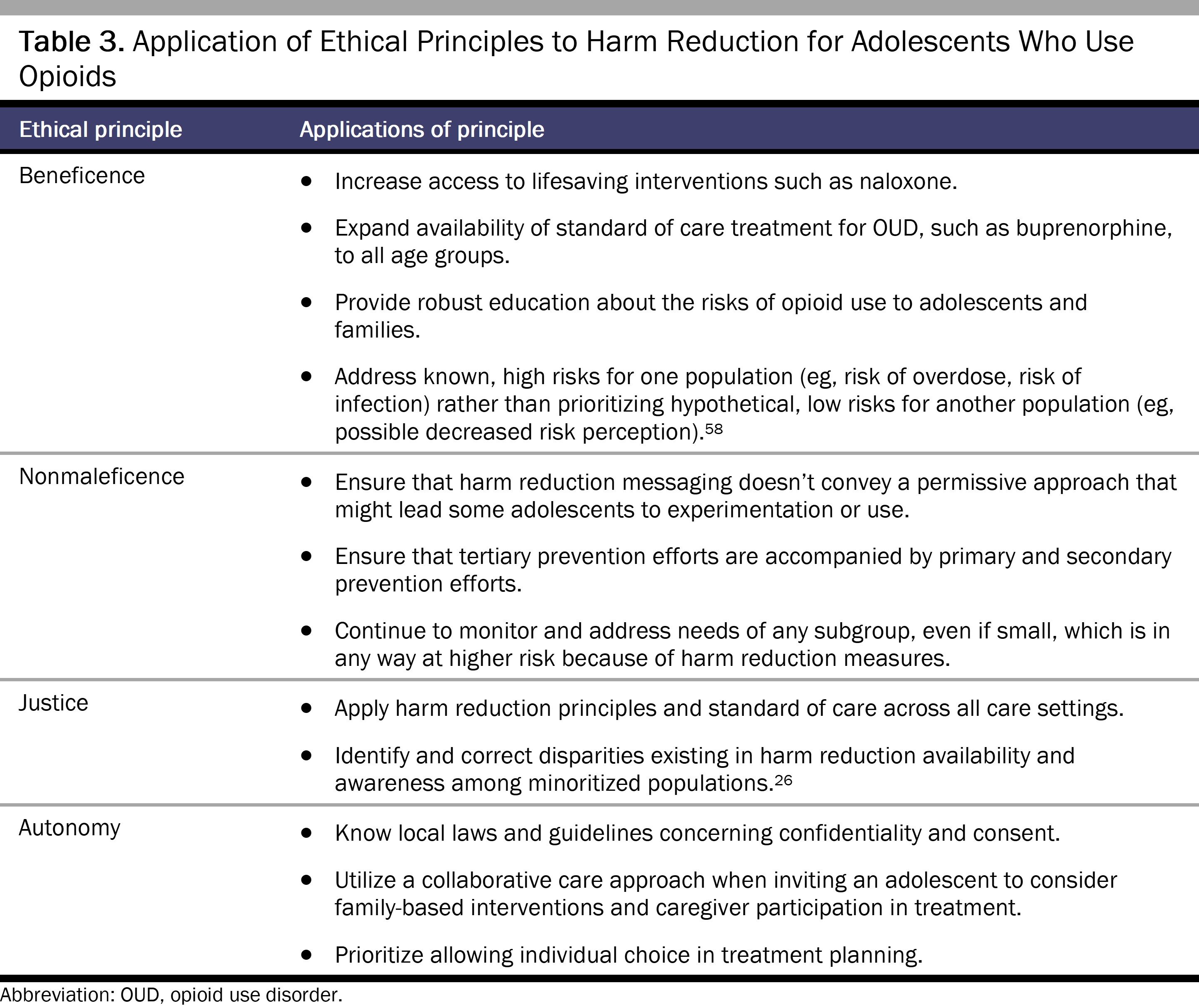
Harm reduction represents, in part, a pivot from blame and punishment to the principles of autonomy, beneficence, nonmaleficence, and justice in addressing substance use (see Table 3).57 Adolescents who use opioids or have OUD can equally benefit from harm reduction approaches. From an ethical standpoint, a teen should have equal, if not expanded, opportunities to choose treatment over use and harm reduction over no treatment. However, legal limits may impair adolescents’ autonomy and ability to access this care.
While clinicians and organizations seek to expand harm reduction to minimize risk in the most vulnerable adolescent population, it is vital that reducing harm not be the only message that adolescents receive. It should be clear that brain development is best supported by abstinence from all substances. Furthermore, limited use is better than regular use; certain patterns and methods of use are less dangerous than others. While regular use is strongly discouraged for adolescents, harm reduction can help prevent significant negative outcomes, including death and severe infections. Expanding resources only to prevent the worst outcomes without equal or expanded efforts to promote and provide primary and secondary prevention (eg, early screening, detection, and intervention) may inadvertently convey the wrong message to adolescents and, at a minimum, may fail to prevent experimentation and escalation of use.
Florence C, Luo F, Rice K. The economic burden of opioid use disorder and fatal opioid overdose in the United States, 2017. Drug Alcohol Depend. 2021;218:108350.
Hawk M, Coulter RWS, Egan JE, et al. Harm reduction principles for healthcare settings. Harm Reduct J. 2017;14:70.
Harm Reduction Steering Committee. Harm Reduction Framework. Substance Abuse and Mental Health Services Administration; 2023. April 1, 2024. https://www.samhsa.gov/find-help/harm-reduction/framework
Why a minimum legal drinking age of 21 works. Centers for Disease Control and Prevention. May 15, 2024. Accessed June 13, 2024. https://www.cdc.gov/alcohol/underage-drinking/minimum-legal-drinking-age.html?CDC_AAref_Val=https://www.cdc.gov/alcohol/fact-sheets/minimum-legal-drinking-age.htm
STATE System minimum legal sales age (MLSA) laws for tobacco products fact sheet. Centers for Disease Control and Prevention. Reviewed January 4, 2024. Accessed February 21, 2024. https://www.cdc.gov/statesystem/factsheets/mlsa/Minimum-Legal-Sales-Age.html
Review of state laws to regulate marijuana. Marijuana Policy Project. Accessed February 21, 2024. https://www.mpp.org/issues/legalization/review-of-state-laws-to-regulate-marijuana/
Miech RA, Johnston LD, Pat ME, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future—National Survey Results on Drug Use, 1975-2022: Secondary School Students. Institute for Social Research, University of Michigan; 2023. Accessed February 2, 2024. https://monitoringthefuture.org/wp-content/uploads/2022/12/mtf2022.pdf
Drug overdose death rates. National Institute on Drug Abuse. June 30, 2023. Accessed August 24, 2023. https://nida.nih.gov/research-topics/trends-statistics/overdose-death-rates
Arain M, Haque M, Johal L, et al. Maturation of the adolescent brain. Neuropsychiatr Dis Treat. 2013;9:449-461.
Semple BD, Blomgren K, Gimlin K, Ferriero DM, Noble-Haeusslein LJ. Brain development in rodents and humans: identifying benchmarks of maturation and vulnerability to injury across species. Prog Neurobiol. 2013;106-107:1-16.
Griffin A. Adolescent neurological development and implications for health and well-being. Healthcare (Basel). 2017;5(4):62.
Jordan CJ, Andersen SL. Sensitive periods of substance abuse: early risk for the transition to dependence. Dev Cogn Neurosci. 2017;25:29-44.
Elliott AS; Adolescent Health Committee, Canadian Paediatric Society. Meeting the health care needs of street-involved youth. Paediatr Child Health. 2013;18(6):317-326.
Chatterjee A, Dunleavy S, Plakas I, Gaeta JM, Taveras E. Street-involved youth and young adult perspectives on harm reduction. J Gen Intern Med. 2020;35(suppl 1):S280.
Goldman-Hasbun J, DeBeck K, Buxton JA, Nosova E, Wood E, Kerr T. Knowledge and possession of take-home naloxone kits among street-involved youth in a Canadian setting: a cohort study. Harm Reduct J. 2017;14(1):79.
Lipari RN. Trends in adolescent substance use and perception of risk from substance use. In: Center for Behavioral Health Statistics and Quality. The CBHSQ Report. Substance Abuse and Mental Health Services Administration; 2013. Accessed August 25, 2023. http://www.ncbi.nlm.nih.gov/books/NBK385059/
Guydish J, Brown C, Edgington R, Edney H, Garcia D. What are the impacts of needle exchange on young injectors? AIDS Behav. 2000;4(2):137-146.
Sawyer K, Rosenberg AR. How should adolescent health decision-making authority be shared? AMA J Ethics. 2020;22(5):E372-E379.
Sharko M, Jameson R, Ancker JS, Krams L, Webber EC, Rosenbloom ST. State-by-state variability in adolescent privacy laws. Pediatrics. 2022;149(6):e2021053458.
Uses and Disclosures of Protected Health Information: General Rules. 45 CFR §164.502 (2023).
Minor Patients. 42 CFR §2.14 (2023).
Hadland SE, Aalsma MC, Akgül S, et al; Society for Adolescent Health and Medicine. Medication for adolescents and young adults with opioid use disorder. J Adolesc Health. 2021;68(3):632-636.
Terranella A, Guy GP Jr, Mikosz C. Buprenorphine dispensing among youth aged ≤19 years in the United States: 2015-2020. Pediatrics. 2023;151(2):e2022058755.
About. Providers Clinical Support System-Medications for Opioid Use Disorders. Accessed February 21, 2024. https://pcssnow.org/about/
Chadi N, Hadland SE. Youth access to naloxone: the next frontier? J Adolesc Health. 2019;65(5):571-572.
FDA approves first over-the-counter naloxone nasal spray. News release. US Food and Drug Administration; March 29, 2023. Accessed April 1, 2024. https://www.fda.gov/news-events/press-announcements/fda-approves-first-over-counter-naloxone-nasal-spray
Moran M. AMA backs making overdose reversal meds accessible in schools. Psychiatric News. June 23, 2023. Accessed February 2, 2024. https://psychnews.psychiatryonline.org/doi/full/10.1176/appi.pn.2023.08.8.41
Opioid use disorder treatment for youth. American Academy of Child and Adolescent Psychiatry. June 2020. Accessed September 2, 2023. https://www.aacap.org/AACAP/Policy_Statements/2020/Opioid_Use_Disorder_Treatment_Youth.aspx
Ryan SA, Gonzalez PK, Patrick SW, Quigley J, Siqueira L, Walker LR; Committee on Substance Use and Prevention. Medication-assisted treatment of adolescents with opioid use disorders. Pediatrics. 2016;138(3):e20161893.
Hosek S, Henry-Reid L. PrEP and adolescents: the role of providers in ending the AIDS epidemic. Pediatrics. 2020;145(1):e20191743.
Davis CS, Lieberman AJ, O’Kelley-Bangsberg M. Legality of drug checking equipment in the United States: a systematic legal analysis. Drug Alcohol Depend. 2022;234:109425.



