Medicine and Society
Jun 2020

This article examines the challenges of raising a child with epilepsy and the role of portraiture in helping clinicians consider the impact of epilepsy not only on the patient but also on family caregivers. Portraiture facilitates the development of a visual narrative of how a child is seen by others, both figuratively and physically.
Thirty percent of children with epilepsy have seizures that are challenging to control and often require multiple medications.1 In the majority of these cases, the seizures cannot be stopped, which negatively affects both children’s development and families’ lives.2,3 Throughout my career as a pediatric neurologist, I have been moved and humbled by the many families I have met who care for children with a diagnosis of epilepsy. The portraiture study detailed here provided me with a way to honor what these families have faced, to allow others to “see” children with epilepsy in a different way, and to increase awareness of what these families live with.
This project was a collaboration between me and Mark Gilbert, a portrait artist and qualitative researcher. Children and their families were recruited from my pediatric neurology practice. I invited patients of a range of ages and their families to participate in order to document families’ reflections on the challenges they face as a child gets older and transitions to adult care. The patients and their families attended multiple drawing sessions with Gilbert. During these sessions, informal dialogue was recorded and transcribed. The families shared what their lives have been like and the challenges they had faced. Gilbert also kept a diary of his own thoughts, observations, and perspectives. Following completion of the portraits, a semistructured interview with each family provided further understanding of the family’s experiences living with epilepsy. The narrative data and portraits were analyzed using a phenomenological qualitative methodology.4,5 This approach provides an understanding of subjective experience6,7 and, in this specific instance, of what life is like for families living with a child diagnosed with intractable epilepsy.
What follows is the story of a single child and family from the study, yet his story represents that of all families living with the disorder. Although the specific challenges each family faces may vary, the unpredictability and stress of epilepsy impacts all families in similar ways. The length of time this family has lived with epilepsy and the multiple challenges family members have faced provide a powerful example of the burden of epilepsy.
Figure. Brad, by Mark Gilbert, 2018
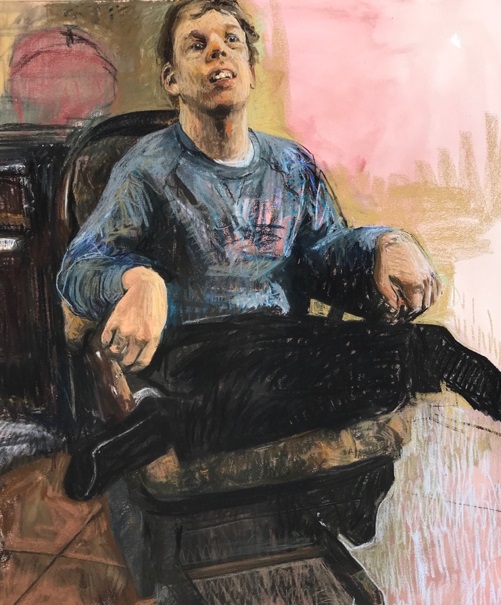
Courtesy of Mark Gilbert.
Pastel on paper, 50.25" x 39.5".
I met Brad when he was a teenager. In a rather convoluted set of circumstances following a car accident, I met the family soon after moving to New Brunswick in Canada to work as a pediatric neurologist. It was a low point for Brad and his family. He was having many tonic-clonic seizures and looked pale and unwell. His parents were feeling there was little hope for improvement in controlling his seizures. Since that time, I have provided neurological care to Brad even though he is now outside the pediatric age group. Through my many interactions with Brad and his family, I have seen his parents’ high and lows, their feelings of helplessness at times, their frustrations with the health care system, and rewarding moments.
Brad is now 26 years old. He is a gentle young man who lights up the room when he smiles. He is nonverbal and yet can communicate with his parents, siblings, and friends in so many ways—by a gentle touch, the use of signs, and sometimes vocalizations. He understands more than he can express and is very demonstrative with his family and friends, giving them hugs and kisses. They have a very strong bond with him.
His seizures began at 1 year of age. The initial few accompanied a febrile illness, but they then continued without illnesses, and Brad developed multiple seizure types. His mother described the sense of fear, urgency, and desperation when the seizures first started. Although the epilepsy became a part of the family’s life, the parents’ immediate fear concerned the loss of who Brad might have become and their desire for a cure for his epilepsy. No etiology was ever found to explain his presentation. Over the years he has been on many different medications, the ketogenic diet, intravenous immunoglobulin, steroids, and he has had a vagal nerve stimulator inserted.8 Despite all these efforts, he has never remained seizure free for an extended length of time. As is common with many patients, he experienced periods of seizure freedom after starting a new medication, but the seizures always recurred.9
The seizures negatively impacted Brad’s functioning and the family’s functioning over time. The family was unable to take vacations and chose to create a positive space at their home on the river. In this way, Brad could—at any time—engage in family activities, such as riding on the personal watercraft with his dad, for example. The parents worked hard to have what they perceived as a normal family life but recognize it was not typical for the majority of people. It was challenging to do things as a family because of the seizures, and when Brad was young there was limited social support that would allow his parents to do things with the other 2 children. Brad’s older and younger siblings recognized that Brad needed more support and have been changed by their experiences with him. His mother stated that his siblings “have great empathy for others” and are “kind and caring. It’s beyond their years … more from an experience point of view.”
Getting to know someone and being present with someone with epilepsy or cognitive delay can challenge and change our viewpoints.
The family had to deal with the stress of the epilepsy itself and the associated impact on Brad’s cognitive and physical abilities. When Brad was younger, he loved to swim, ride horseback, and go skating. He would smile from ear to ear during these experiences. He is no longer able to do these things due to safety concerns. Now that he is in young adulthood, his parents fear for his future. They worry he will end up in an institutional or home setting with less care and support. Specifically, they are concerned he will lose his current quality of life. He goes out walking, goes to the mall, and goes to see hockey games, for example. He loves to sit in the garden and watch the birds or walk barefoot in the garden and at the beach. His parents have sought out daytime activities, but these often provide less stimulation than activities at home, making them feel uncertain about the future, particularly if they die before Brad.
When Brad was young, his parents were told by one physician that he would not be able contribute to society and they should just let him be. His mother believes everyone brings something to society that does not have to be on an intellectual level. She shared an example of being at the grocery store. A woman was being mean to the cashiers, then Brad had a seizure. This woman completely changed, becoming gentle and supportive and doing whatever she could to assist Brad. His mother reflected: “Your contribution in life can be in various ways… I think how he [Brad] touches or changes people or makes them think differently about their life is … more powerful than [what] most of us bring to society.”
In society, we struggle with acceptance and tolerance of people who are different from ourselves, often due to fear of the unknown.10 Getting to know someone and being present with someone with epilepsy or cognitive delay can challenge and change our viewpoints. Brad’s mother shared a perspective from someone she knew who got to know Brad: “I’m not afraid anymore. I’m not afraid of somebody who doesn’t look like me or act like me or [if] cognitively they’re impaired. I’m not afraid of how somebody looks.” Children at school, family friends, and others who have gotten to know Brad are touched by his gentleness and his joy in the moment, noting that “sitting at a table, you can’t help but be drawn into his aura of pureness and goodness.”
Previous research has demonstrated that the creation of images humanizes and gives voice to the people and communities pictured. In Gilbert’s previous arts-based research, patients with cancer whose portraits he painted described feeling empowered—of not feeling alone—when they saw the other portraits and found it therapeutic to share their stories and feel heard.11 There is, however, a vulnerability and risk in having a portrait painted. During this study, Brad’s mother was concerned that a portrait would not capture the “whole picture” and would be limited to a period in his life. She feared that people would only see one side of Brad, depending on the final image(s) used in the show. She hoped people would be able to see all of who he is and not just the physical impact of the seizures. The project tapped into all the different experiences and emotions she had had over the years. His mother shared with me: “When I … let myself go to that place [the challenge of the initial diagnosis]. it’s still raw.… After 26 years, you would think it wouldn’t be. But I think everyone wants the best for their child.”
Nevertheless, Brad’s mother found the experience of sharing during the creation of the drawings and portraits therapeutic. To have someone listen allowed some of the hard moments from the past to be “washed away,” which she found freeing. When she saw the artwork displayed collectively and saw the portrait of Brad hung, she noted: “When I really stopped to look at it, I thought you [Gilbert] caught him, the essence of who he is, beautifully” (see Figure). Some friends accompanied her to the opening of the initial show, and they could not believe the detail of Brad’s portrait and the emotion they felt looking at it. She was moved by seeing the whole collection of portraits of my patients: “Every picture would capture an emotion within. And I think the emotion is different for everybody…. The artwork is kind of the vehicle that lets us see the emotion … and gives people a glimpse of who that individual is without knowing the details of his life.”
The project has had a profound effect on me and been a source of my reflections on care of children with chronic illnesses. Although I know these families well and understand many of their struggles, I am struck by how much more I have learned when the families were given time to share their stories. So often in medicine, we are constrained by time and focused on the medical issues at hand. Yet other issues are often more important for families, particularly if there is no cure. Families might need social, financial, or other support, and they need to know that someone is there for them.
Intractable epilepsy means there is no cure, and physicians must live with this uncertainty and lack of resolution. Walking with a family and being willing to listen is as important as the medical treatment. The portraiture study has affirmed my belief in the importance and value of being present to families, even when there is no cure. This trusting relationship can help them keep going and feel less alone and isolated.
In previous work, Gilbert identified themes that are common to the artist-sitter relationship and to the doctor-patient relationship: embracing uncertainties, developing trusting relationships, engaging in reflective practices, telling a story (expression), and being empowered.12 Portraiture provides a forum for learners and professionals to consider aspects of epilepsy care beyond medications, surgeries, or special diets. The portraits themselves provide a way of more wholly seeing patients and their families as individuals with struggles, resilience, and rewards and of understanding the impact of epilepsy on the family unit. The humanization of individuals has the potential to help health professionals find meaning at a time when burnout is a significant concern.13,14 The portraits created for this project are being used to educate the public, practitioners, and learners in health care about seizures and epilepsy and will have a role in advocating for families living with epilepsy.15
Janmohamed M, Brodie MJ, Kwan P. Pharmacoresistance—epidemiology, mechanisms, and impact on epilepsy treatment. Neuropharmacology. 2020;168:107790.
Moustakas C. Phenomenological Research Methods. Thousand Oaks, CA: Sage; 1994.
Giorgi A. The Descriptive Phenomenological Method in Psychology: A Modified Husserlian Approach. Pittsburgh, PA: Duquesne University Press; 2009.
Wertz FJ, Charmaz K, McMullen LM, Josselson R, Anderson R, McSpadden E. Five Ways of Doing Qualitative Analysis. New York, NY: Guildford Press; 2011.
Avanzini G. Is tolerarance to antiepileptic drugs clinically relevant? Epilepsia. 2006;47(8):1285-1287.
Canadian Medical Association. CMA national physician health survey: a national snapshot. https://www.cma.ca/sites/default/files/2018-11/nph-survey-e.pdf. Published October 2018. Accessed April 8, 2020.
Reith TP. Burnout in United States healthcare professionals: a narrative review. Cureus. 2018;10(12):e3681.
Tunney J. Seeing the patients: art shines light on New Brunswick children with epilepsy. CBC News. Sept. 13, 2018. https://www.cbc.ca/news/canada/new-brunswick/epilepsy-arts-saint-john-1.4821122. Accessed February 17, 2020.



