Case and Commentary
Jun 2020
This article describes one collaborative arts-based research project. Portrait artist Mark Gilbert and coinvestigators consider lessons for art and healing from one patient, Anthony, whose experience of head and neck cancer diagnosis, surgery, and recovery suggests how silence is ethically, artistically, and clinically significant.
At the request of Virginia Aita and the fourth author (WL), the first author (MG) was invited to coconduct an arts-based research study using portraiture to investigate care and caregiving. In this mixed-methods study, MG drew and painted patients and their caregivers. The project culminated in an exhibit, Here I Am and Nowhere Else: Portraits of Care (POC) and was displayed at the Bemis Center for Contemporary Arts in 2008-2009.1 This exhibit featured visual art as a means of cultivating deeper understanding of ethical and aesthetic values expressed in the experiences of patients, family caregivers, clinicians, and others—janitors, biomedical researchers, public health professionals, and policymakers, for example—working in health care. POC considered portraiture to be an untapped resource in health care that could be used to “imagine the humane dimensions, cultural frameworks and processes that shape human experiences of health and illness.”2 The relationship that MG shared with one POC participant, Anthony, is especially illustrative of this purpose. Although this essay about Anthony is conveyed in MG’s voice, this work has been a collaboration among the 4 authors.
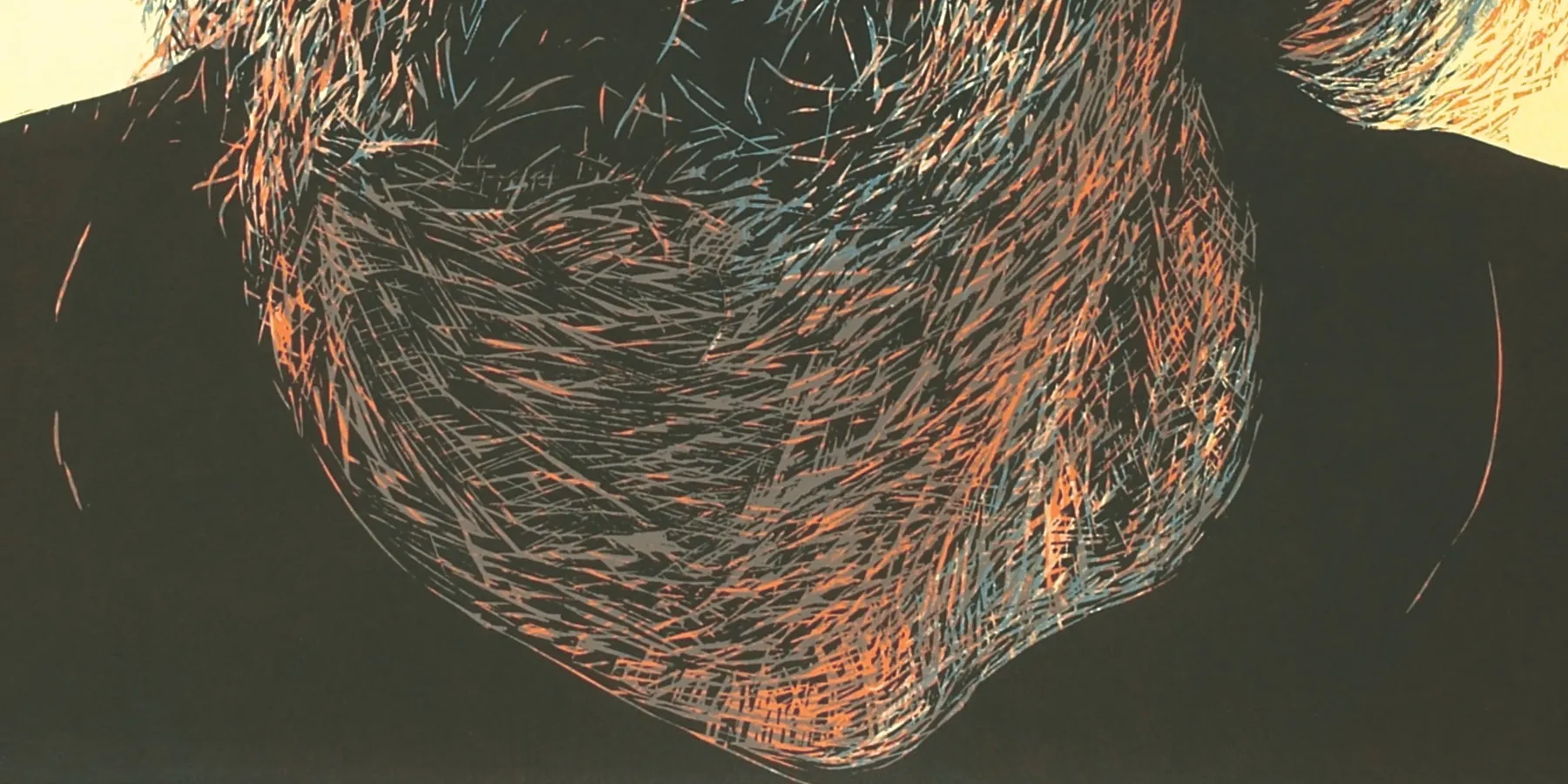
I first met Anthony in the company of WL just prior to his tumor resection surgery. Anthony had graying hair tied back in a ponytail. His thin beard covered, but could not hide, a protruding cancer that enveloped most of his mandible, lower jaw, and tongue. When Anthony first noticed the tumor, he avoided treatment and traveled around the Midwest by himself. MG wondered why Anthony delayed seeking treatment and if his finally doing so was at the behest of his sister Gloria, who accompanied him that day to the clinic. Anthony was soft spoken, and his voice was somewhat muffled, as the tumor restricted movement of his tongue and jaw. His surgery that day would leave him unable to communicate verbally and therefore would illuminate the ethical and aesthetic roles of silence in MG’s subsequent interactions with him.
Figure 1. Anthony (Before Surgery), 2008
Courtesy of Mark Gilbert.
Woodcut, 44" x 32".
Surgical removal of Anthony’s larynx, tongue, and lower jaw left him unable to talk. A citizen of the Winnebago tribe of Eastern Nebraska, Anthony had misgivings about sitting for his portrait, and these misgivings were founded in his traditional belief that being drawn or photographed “toys with someone’s spirits.” MG was initially concerned that the verbal one-sidedness of the interactions would be awkward, but Anthony wrote short notes during his portrait sessions to communicate. MG learned that Anthony was also an artist who worked in traditional leather and beadwork. Many of MG’s and Anthony’s exchanges focused on their respective artistic practices. Anthony visited MG’s studio weekly for 6 months.
Silently, together, MG and Anthony cocreated in multiple media and formats. Portraits of Anthony were drawn on canvas and paper and carved into wood for a relief print. MG used photography to record Anthony’s time as an anesthetized patient. Anthony’s resected tumor is shown below in a color monotype.
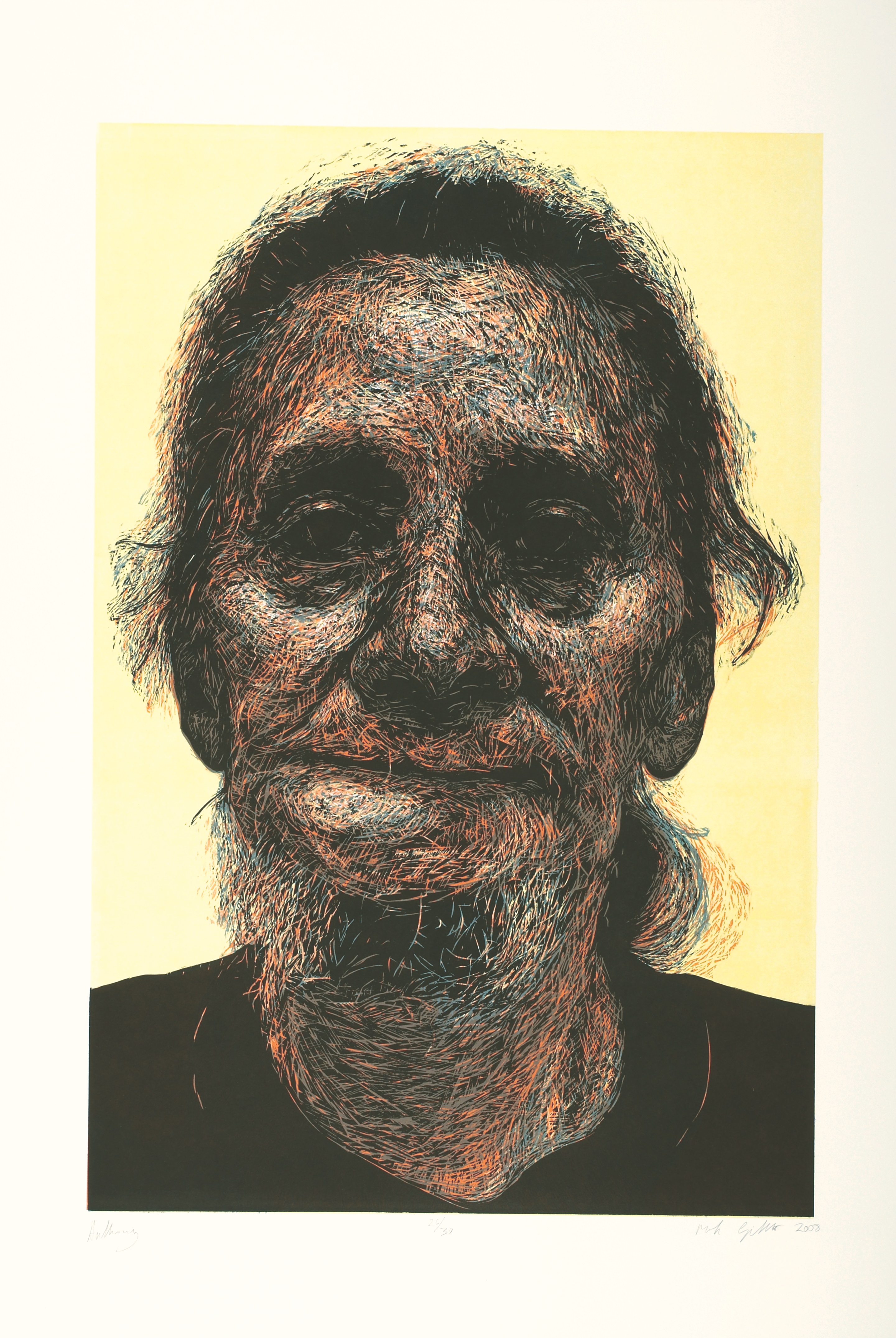
Figure 2. Tumor (Anthony), 2006
Courtesy of Mark Gilbert.
Monoprint, 40" x 26".
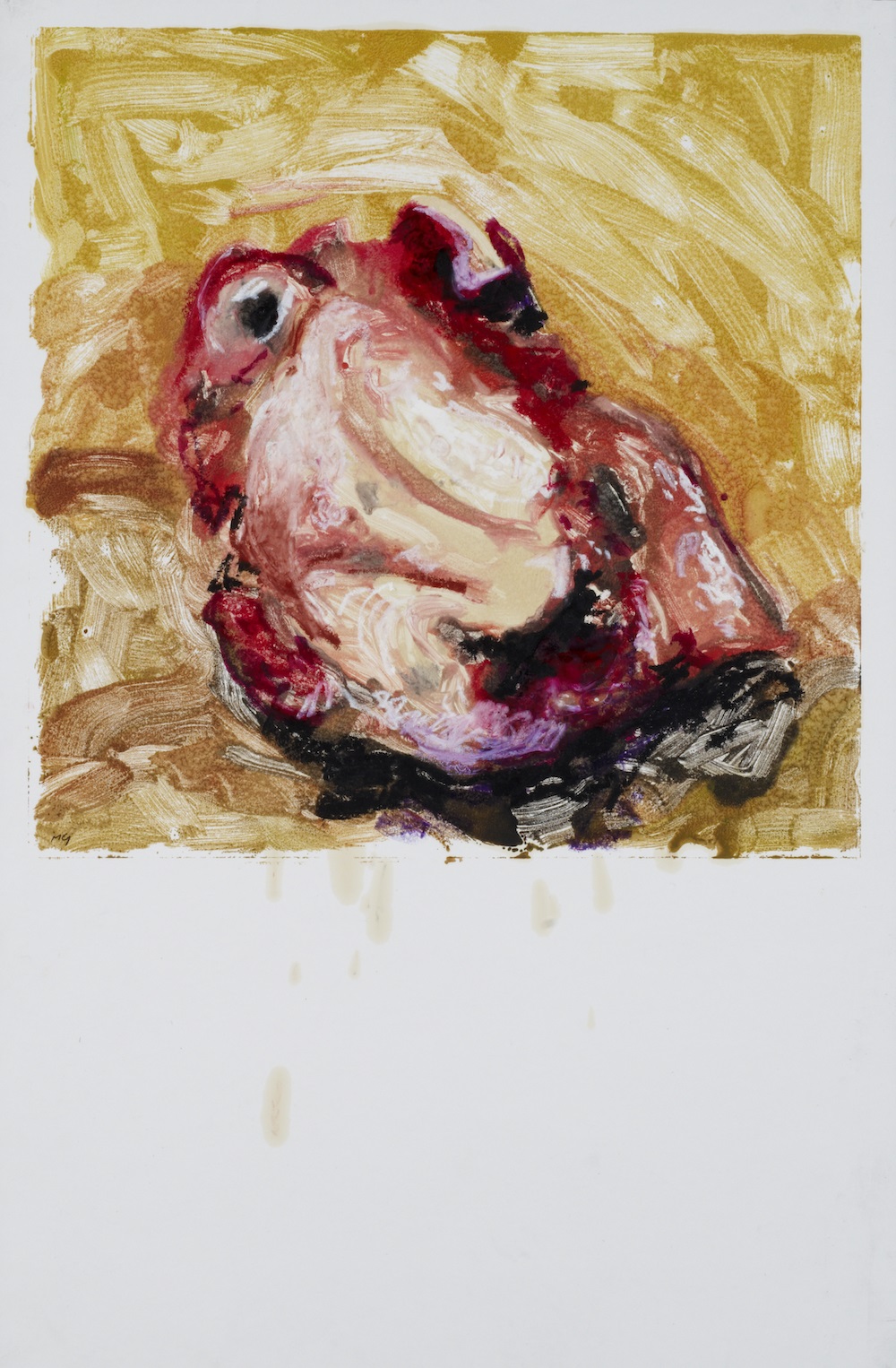
A photogravure of Anthony’s tongue and lower jaw, suspended in WL’s hands, was also made.
Figure 3. Removed Cancer (Anthony), 2008
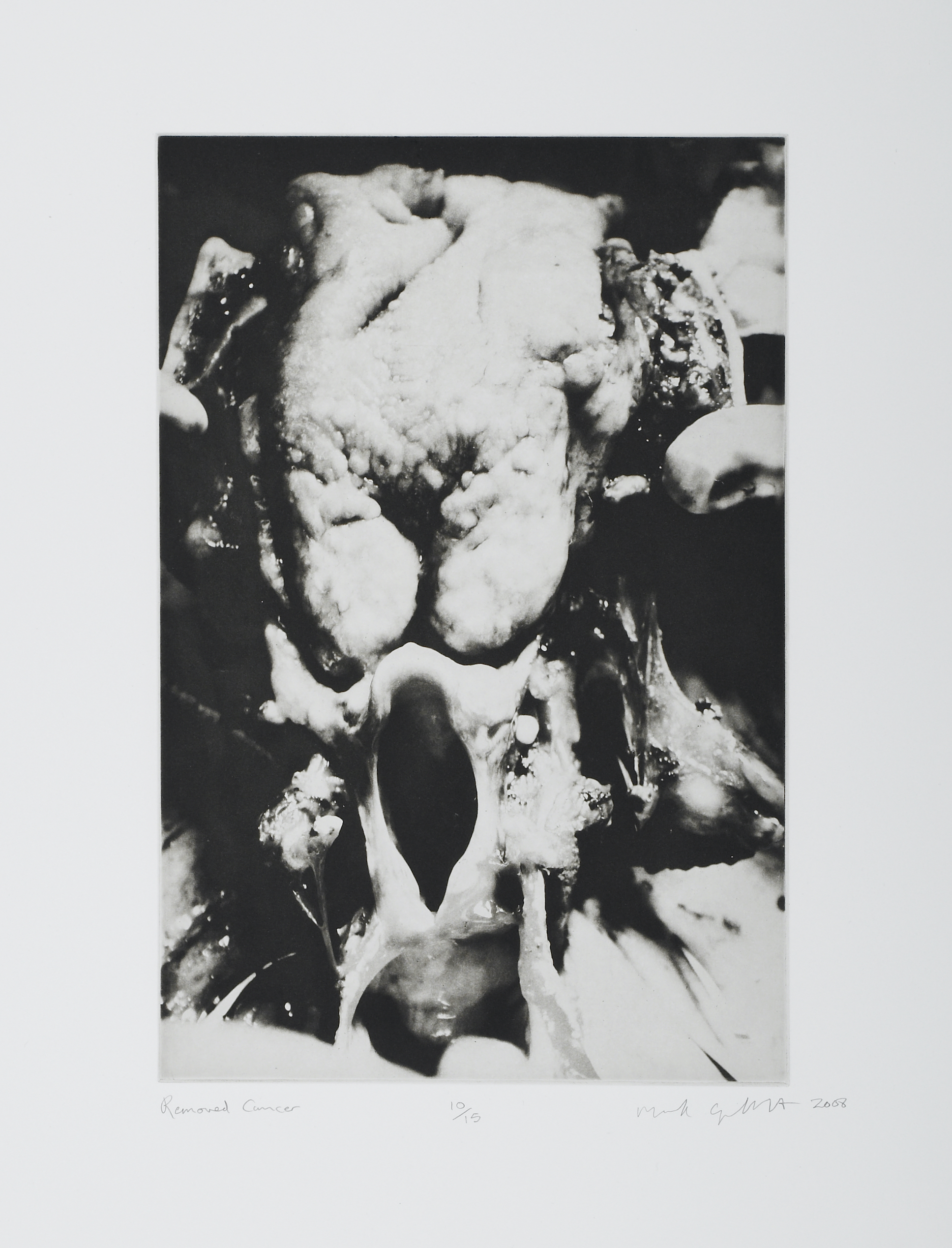
Courtesy of Mark Gilbert.
Copper photogravure, 20" x 15".
As WL and others worked to remove Anthony’s jaw, tongue, and larynx, MG quietly sketched in pencil and photographed the specimen. Once removed, Anthony’s jaw, voice box, and tongue were held by MG in his hand. MG still vividly remembers their weight.
In depicting the tumor, MG hoped to respectfully depict the mass and volume of what was removed from Anthony’s body. Aesthetically, the cancer glistened and seemed bejeweled under the glare of the operating theater lights; ethically and clinically, however, the tumor specimen can be appreciated as being threatening and insidious. Elsewhere the third author (MMD) and her coauthor, 2 Indigenous scholars, explain how, “as part of the self-telling body that is the field of MH and NM [Medical Humanities and Narrative Medicine], we tell our stories … because, like the parts of a body or the individual strands in a sweetgrass braid, our stories are connected to yours, irrevocably connected.”3 In holding the tumor or even beholding the images made of the tumor, we might more fully recognize how the tumor, whether inside or outside Anthony’s body, is an integral part of his story, a critical thread in his narrative. MG spent more time with Anthony than any other participant in POC. In the silence of the studio, Anthony and MG listened and responded to each other’s curiosity and presence, drawing on portraiture to navigate different orientations to Anthony’s life with the tumor and his life after its resection.
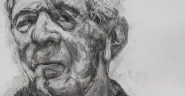
Figure 4. Anthony, 2007
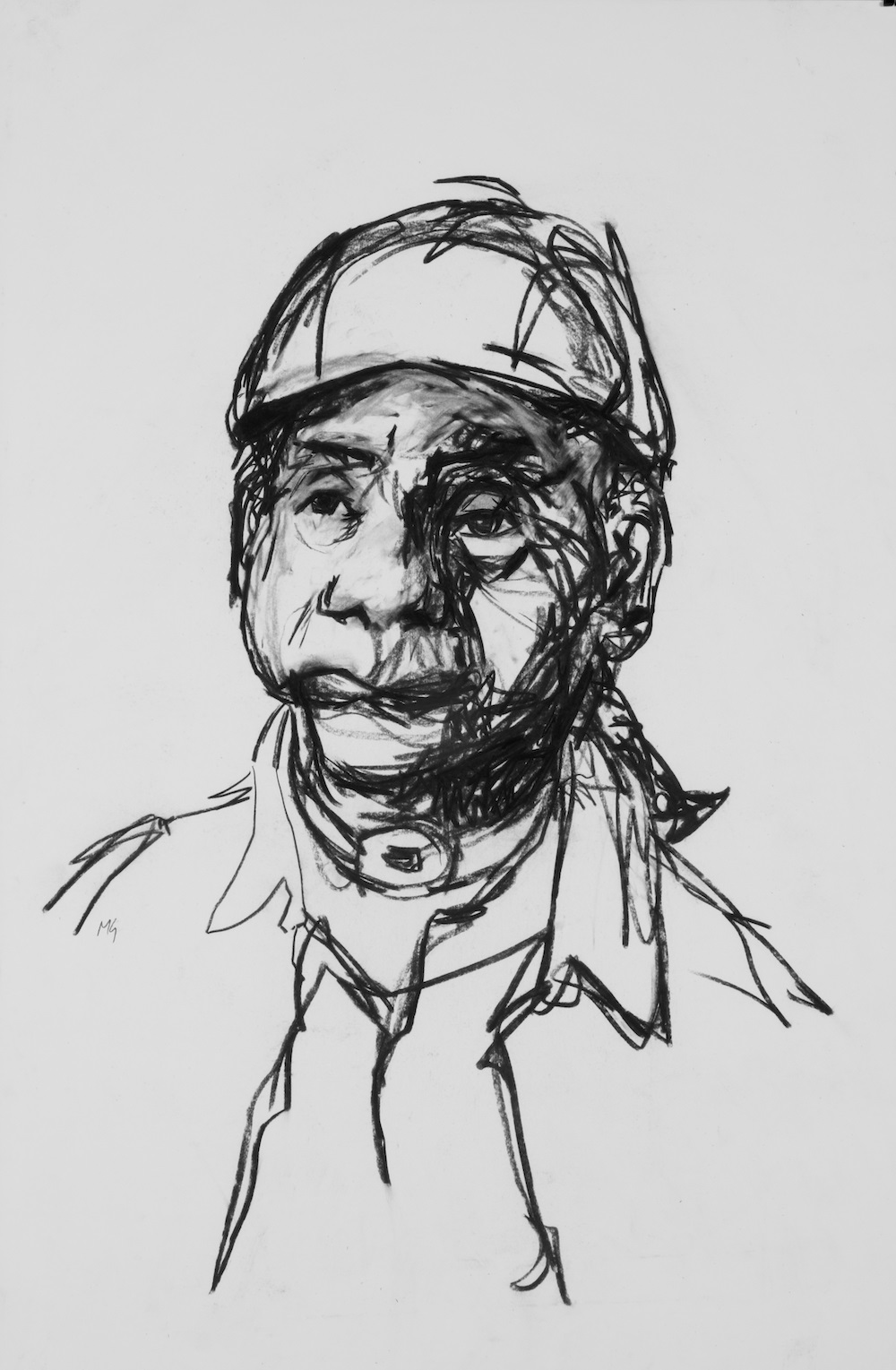
Courtesy of Mark Gilbert.
Charcoal on paper, 44" x 32".
Anthony let MG witness his responses to the demands of his recovery, his poise while adapting to his new postsurgery world and appearance, and his journey of learning to be composed despite being rendered nonverbal. Upon completion of his portraits, Anthony wrote of the role that his work with MG played in his recovery and of his adjustment to postresection life, describing the portraits as “testimony of the struggle that would follow to make life livable again with all of these changes.”
In many portrait sessions, as the studio goes silent, the sounds of the first marks on the paper and those of the sitter settling into position accentuate both artist’s and subject’s embarking on an activity that generates an almost instant intimacy. Silence, deep looking, and curiosity emanate from both sides of the easel, sometimes creating an initial awkwardness. As the discomfort of those first moments dissipates, however, artist and sitter can interact and share to create a portrait that both testifies to their relationship and narrates the sitter’s experiences.
Anthony lost his tongue and larynx, but he did not lose his voice. The silence that took its place became a profound form of expression.
As an artist, MG is acutely aware of the courage required to sit for one’s portrait. In general, the silence in portraiture is often broken, punctuated with conversation. Although MG never regarded the silence as an empty void, Anthony helped him realize how much he’d initially assumed that verbal exchanges were the primary influence on the development of artist-sitter understanding, trust, and reciprocity during portrait sessions. That is, it is usually through talking that sitters and artists exchange stories; voice their passions, fears, and anxieties; and describe their responses to day-to-day happenings. These conversations, MG once thought, were the richest way to build relationships and create portraits.
Silence and intimacy. It was not until MG worked with Anthony that he recognized silence as a deeply communicative act. Anthony lost his tongue and larynx, but he did not lose his voice. The silence that took its place became a profound form of expression. Anthony sensitized MG to the importance of silence and its salient role in portrait making. In Anthony’s case, quiet was there to be discerned, just as noise might be. In silence, Anthony and MG gave earnest attention to nonverbal communication cues and were mutually committed to keeping, safeguarding, and stewarding silence. Neither sought to fill quiet with noise; Anthony’s visual narrative of living with cancer and recovery was allowed to grow in—indeed, was enabled and enhanced by—the silence and in the space we inhabited together.
Silence and presence. In portraiture, both artist and sitter tend to be absorbed in the here and now. Silence is considered essential to developing full awareness of a present moment.3 Silence can be thought of as preparing a field for observing, for noticing. For artists and sitters alike, silence is to soundscape as space is to landscape, a state of receptivity, openness, and acceptance. Silence nurtures curiosity, stimulates interest, and frames the field in which thoughts, feelings, and sensations can be observed, interpreted, and visually recorded. Sitters often tell MG how they use the quiet of their sessions to reflect, meditate, or even pray. MG, too, uses the quiet to look, consider, and appreciate.
Silence and equality. Portrait making involves concentration, sustained focus, and astute attention to specific physical, mental, and sensory experiences. A productive portraiture process can be understood as occupying time and space for purposes of telling and listening that inform the painting of an aesthetic and narrative whole. Although positioned differently, both artist and sitter are intentional, actively learning from one another, building trust, and recognizing each other’s strengths, weaknesses, values, interests, and thoughts. As Back and colleagues explain, “While there are silences that feel awkward, indifferent, or even hostile, there are also silences that feel comforting, affirming, and safe.”5 Occupying silence in comfort means sharing power—the power of disruptive potential, perhaps. One way to think of the ethical value of silence is in how artist and subject express respect for each other’s equal potential to disrupt silence or stillness at any moment: painting and sitting demand that artist and subject embody that equality in their respective roles.
Silence and narrative. Learning to interpret what silence-stillness offers is also part of good portraiture practice. A portraitist’s challenge is to be open not only to what is seen and heard but also to what is present and what is absent. Similarly, noticing and responding to space and negative space is vital to creating a narrative whole. As Buetow explains, “If we ignore the negative space, we risk seeing only the positive space we expect to see, rather than what is there.”6 What is excluded is as important as what is included: blank space and silences shape the portrait as much as marks and layers of paint. For the portraitist, navigating the tension between documenting and creating, receiving and shaping, reflecting and imposing, and mirroring and improvising is a strategy for achieving visual narrative coherence and accuracy that flows organically from data offered by the subject and from the portraitist’s interpretive witnessing.7 Artist and sitter cocreate visual narrative by inviting each other to fully engage with the potential of uncluttered space-time and silence-stillness to think and reflect and to see, feel, recognize, and generously acknowledge each other. Generosity is one thing creation and healing ask of us all. Anthony teaches us this.
These elements of creating visual narrative in portraiture can also be useful in clinical practice. Anthony’s portrait with the tumor, the painting of his resected tumor, and his portrait without the tumor form a series, enabled by his having shared silence with MG. Noises in clinical environments where health care is delivered tend to be distracting and to interfere with the attentiveness required for the artist’s careful theme development and compositional decision making.8 But silence has its risks in both clinic-based and studio-based narrative inquiry. For a patient, silence can provoke anxiety, especially if someone disrupts a quiet space unilaterally. A mutually occupied silence, however, can nurture symmetrical connection, foster shared experience, and make collaboration and care palpable. Thus, in clinical settings as in studio settings, artists and subjects occupy silence together to enable cultivation of what Hart calls an “inner technology of knowing”9 that can engage stories and portraits of healing.
Bemis Center for Contemporary Arts. Mark Gilbert: Here I Am and Nowhere Else: Portraits of Care, Gallery 1. https://www.bemiscenter.org/art/past_section/mark_gilbert.html. Accessed May 11, 2020.
Desmarais MM, Robbins RE. From the ground up: indigenizing medical humanities and narrative medicine. Survive Thrive. 2019;4(1):6.