Medicine and Society
Aug 2022
Peer-Reviewed

Clinicians cannot always directly or effectively engage patients experiencing mental health crises. This article considers the common practice of relying upon law enforcement personnel to facilitate mental health checks and considers its implications for Black patients. An antiracist approach to decriminalizing acute exacerbations of mental illness requires clinicians’ engagement in educating, training, and policymaking. This article recommends strategies for effective real-time communication before, during, and after a 911 call involving a person experiencing a mental health crisis.
An estimated 1 of 5 Americans lives with mental illness, and the number of adults reporting unmet mental health needs has increased during the COVID-19 pandemic.1,2,3 Clinicians sometimes call emergency services to recruit police to facilitate mental wellness checks on individuals expressing suicidal ideation or intent to harm themselves or others. However, reliance on law enforcement to handle such emergencies can escalate already sensitive situations. Police officers are more likely to arrest individuals with mental illness for minor offenses or use lethal force than individuals without mental illness.4,5
Criminalization of mental health is situated within the broader context of racialized policing practices in America. Black Americans are disproportionately represented among victims of lethal and nonlethal police violence compared to White Americans.6 The fatal shooting of Travis Jordan, a 36-year-old Black man killed by police in 2019 after his girlfriend called 911 out of fear that he would complete suicide, expresses harrowing irony: the dangers of a wellness check. In the 911 transcripts, Jordan’s girlfriend tells the dispatch officer that Jordan called her “all the time saying he wants to die” and that she did not “know how to deal with it.”7 Approximately 15 minutes later, he was shot and killed. The officers did not face criminal charges.8
While the media publicizes only a fraction of such encounters, we must acknowledge inequitable trauma suffered by Black persons from unexpected and frequently armed police responses. The impact of police brutality extends beyond those directly involved, as the mental well-being of Black adults is further eroded when they are exposed to police killings of Black Americans.9,10 These consequences are relevant for all people of color and disadvantaged communities.11 Police violence is uniquely traumatic in being conceptually distinguishable from other forms of violence and independently associated with adverse mental health outcomes.12 In a vicious cycle, exposure to police violence is an independent risk factor for subsequent mental illness, and those suffering from untreated mental illness are 16 times more likely to be killed during police confrontations than other civilians.11,13
An antiracist approach to decriminalizing acute exacerbations of mental illness requires clinicians’ engagement in educating, training, and policymaking. This article recommends strategies for effective real-time communication before, during, and after a 911 call involving a person experiencing a mental health crisis.
Lack of available community mental health services usually means persons experiencing crises lack access to emergent psychiatric services. Clinicians are often unable to directly intervene and thus could justify involving law enforcement to engage a patient in distress. But we are professionally and ethically obligated to ask whether and when calling 911 causes harm to historically marginalized patients. Antiracism requires us to identify historically racist policies and practices and stop perpetuating them. Drawing from abolitionist approaches to health justice and equity, we can reimagine what intersections between health and public safety should look like.14
Training and policy. Specifically, antiracism requires us to question clinical practices that utilize force, such as seclusion or physical or chemical means of restraint.15 Clinicians’ perceptions of threat or harm can be distorted and muddled by affective biases (eg, the belief that Black persons are inherently dangerous), which can prompt inequitable uses of force against Black patients.16,17 Indeed, Black patients are more likely than others to be physically restrained in emergency departments.18,19 Historically, inequitable uses of force have fueled racist narratives used to suggest Black persons’ “propensity” for criminality and violence.15 This relationship between carceral and clinical logic can cause harm when clinicians call upon police to extend the reach of clinical control. Interventions targeting sources of clinicians’ affective bias should motivate understanding of their origins to effectively combat racism within and beyond clinical settings during wellness checks.20,21,22
Protocol. Clinicians need explicit training in how to orchestrate and conduct suicide risk assessments and in de-escalating situations in which patients are at risk of harm.23 They must become comfortable in de-escalation to decrease reliance upon law enforcement. Clinical care guidelines might encourage clinicians to call 911 to secure a patient’s or their own safety and well-being, but even well-intentioned policies exacerbate systemic racial inequity. Prior to involving law enforcement, attempts to reach a patient’s emergency contacts are obligatory. If these efforts are insufficient, a crisis hotline, if available, should also be utilized prior to calling 911, so that a mobile mental health crisis team or mental health professional can initially respond and contact police only if needed.24 Clinicians and organizations must interrogate whether their policies undermine equity and can be improved to promote structural change25—specifically, by asking who benefits and who is harmed by a policy, who was involved in its development, and how can it be better formulated to express antiracism.26
Communication. If de-escalation attempts have been exhausted and the benefits of contacting law enforcement appear to outweigh potential harms, particularly in situations in which the threat of harm to the patient or others is imminent, communication between a caller and dispatcher is critical. A dispatcher’s subjective interpretation of a situation’s urgency and severity can affect how frontline responders are informed.27 Antiracist dispatch practice28 includes bidirectional, structured communication. We recommend clinicians provide the following information to a dispatcher (see Figure).
Figure. Information for Police Wellness Check
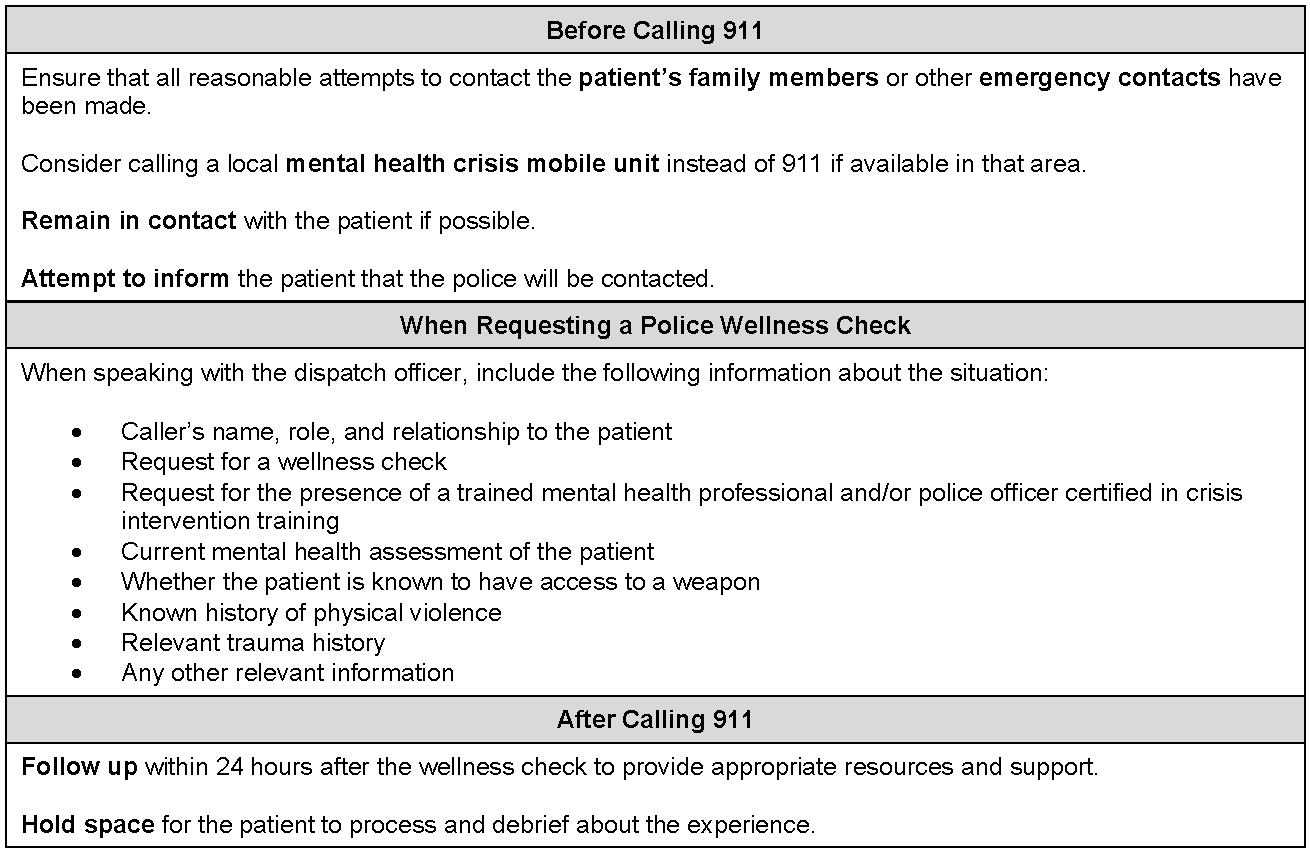
A clinician-caller should then inform the patient to expect an encounter with emergency responders, including police. It is essential to follow up to provide resources and hold space for the patient to process and debrief about a potentially traumatic experience.29
Inequitable and potentially deadly impact of police mental health checks is but one example of how clinicians’ actions exacerbate oppression. Responsibility to cultivate antiracist crisis responses and to decriminalize mental illness belongs to students, clinicians, and organizations, who must formalize training,28 partner with local mental health advocacy organizations, lobby for mental health service and resource expansion, and promote research that motivates equity through antiracist action.30,31 Research should also evaluate outcomes of implementing the recommendations offered in this article and seek to more robustly document and centralize data about wellness check practices.
When the 988-call number replaces the National Suicide Prevention Hotline number by July 2022,32 mental health crisis counselors are likely to be as easy to reach as a 911 dispatcher. Furthermore, if passed, the Mental Health Justice Act, introduced in the US House of Representatives in 2021, would award grants to states to hire more mental health professionals to serve in first responder units.33 These efforts are encouraging attempts to limit police exposure to patients of color in need of mental health care. Clinicians’ roles in promoting unarmed, decriminalized, and antiracist mental health crisis responses are key.
Han B. Key substance use and mental health indicators in the United States: results from the 2019 National Survey on Drug Use and Health. HHS publication PEP20-07-01-001, NSDUH series H-55. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Accessed October 4, 2021. https://www.samhsa.gov/data/sites/default/files/reports/rpt29393/2019NSDUHFFRPDFWHTML/2019NSDUHFFR090120.htm
Tate J, Jenkins J, Rich S. Fatal force. Washington Post. Updated April 20, 2022. Accessed October 4, 2021. https://www.washingtonpost.com/graphics/investigations/police-shootings-database/
911 transcript: victim of Folwell police shooting previously told girlfriend he wanted to die. FOX 9 Minneapolis-St Paul. November 12, 2018. Accessed October 4, 2021. https://www.fox9.com/news/911-transcript-victim-of-folwell-police-shooting-previously-told-girlfriend-he-wanted-to-die
McGuire M. Minneapolis police officers not charged in shooting death of Travis Jordan. CBS Minnesota. January 3, 2019. Accessed April 27, 2022. https://minnesota.cbslocal.com/2019/01/03/police-officers-not-charged-in-fatal-north-minneapolis-shooting/
DeVylder JE, Jun HJ, Fedina L, et al. Association of exposure to police violence with prevalence of mental health symptoms among urban residents in the United States. JAMA Netw Open. 2018;1(7):e184945.
Fuller D, Lamb HR, Biasotti M, Snook J. Overlooked in the undercounted: the role of mental illness in fatal law enforcement encounters. Office of Research and Public Affairs; 2015. Accessed October 4, 2021. https://www.treatmentadvocacycenter.org/storage/documents/overlooked-in-the-undercounted.pdf
Bhattacharyya S, Breslow AS, Carrasco J, Cook B. When structural inequity is ubiquitous, can force ever be compassionate? AMA J Ethics. 2021;23(4):E340-E348.
Wong AH, Whitfill T, Ohuabunwa EC, et al. Association of race/ethnicity and other demographic characteristics with use of physical restraints in the emergency department. JAMA Netw Open. 2021;4(1):e2035241.
Maina IW, Belton TD, Ginzberg S, Singh A, Johnson TJ. A decade of studying implicit racial/ethnic bias in healthcare providers using the Implicit Association Test. Soc Sci Med. 2018;199:219-229.
FitzGerald C, Martin A, Berner D, Hurst S. Interventions designed to reduce implicit prejudices and implicit stereotypes in real world contexts: a systematic review. BMC Psychol. 2019;7:29.
Bolton JM, Gunnell D, Turecki G. Suicide risk assessment and intervention in people with mental illness. BMJ. 2015;351:h4978.
Puntis S, Perfect D, Kirubarajan A, et al. A systematic review of co-responder models of police mental health “street” triage. BMC Psychiatry. 2018;18:256.
Racial Equity Tool: policy review worksheet. Puget Sound Educational Service District. Accessed April 27, 2022. https://resources.finalsite.net/images/v1533747604/psesdorg/iitlnnnhmnv3txzin6zs/PSESD_RET_PolicyReviewWorksheet.pdf
Drew P, Walker T. Citizens’ emergency calls. In: Coulthard M, Johnson A, eds. The Routledge Handbook of Forensic Linguistics. Taylor & Francis; 2010:chap 7.
Mitchell K, Graziani C. Reimagining 911 and Non-Police Crisis Response Work Group recommendations. Non-Police Crisis Response Work Group; 2021. Accessed April 27, 2022. https://www.austintexas.gov/sites/default/files/files/RPS-TF%20Reimagining%20911%20and%20Non-Police%20Crisis%20Response%20Recommendations.pdf
Price D; University of Michigan School of Social Work. Teaching law enforcement new ways to engage. Ongoing. 2021;Spring:2-5. Accessed April 27, 2022. https://ssw.umich.edu/sites/default/files/publications/ongoing-spring-2021.pdf
President’s Task Force on 21st Century Policing. Final Report of the President’s Task Force on 21st Century Policing. Office of Community Oriented Policing Services, US Department if Justice; 2015. Accessed April 27, 2022. https://cops.usdoj.gov/pdf/taskforce/taskforce_finalreport.pdf
National Suicide Hotline Designation Act of 2020, S 2661, 116th Cong (2019-2020). Accessed June 10, 2022. https://www.congress.gov/bill/116th-congress/senate-bill/2661/text
Mental Health Justice Act of 2021, HR 1368, 117th Cong (2021-2022). Accessed April 27, 2022. https://www.congress.gov/bill/117th-congress/house-bill/1368/text



