Viewpoint
Jul 2012

The increase in diagnostic and therapeutic options over the last half century has created more medical decision making situations. Yet the process of medical decision making remains nebulous. Many decisions (e.g., ordering routine blood tests) are made unilaterally by physicians, while others (e.g., elective surgical procedures, medication adherence) involve more patient choice. In many cases, decisions may not be straightforward, and the choices of patients do not always align with the advice of physicians. Practice standards that guide decision making have shifted greatly in recent decades from a paternalistic model to one based on respect for patient autonomy and, more recently, to shared decision making (SDM) [1-3].
These models, however, focus more on who makes the decision than on how the decision is made. Therefore, our aim is to identify elemental characteristics necessary for decision making, establish how they affect the information exchange between physician and patient, and provide an ethical framework for the SDM process.
Shared decision making is an active dialogue between physician and patient with the goal of arriving at mutual understanding and agreement on a treatment plan [1, 3]. With the shift in decision making roles, SDM has been interpreted in various ways that describe rigid authority roles (for either patient or physician) that do not accord well with the process of decision making [4]. A recently published shared decision making continuum proposes a shifting balance between physician expertise (paternalism) and respect for patient autonomy [5]. This framework depicts varying degrees of patient and physician authority with regard to the decision-making process, rendering SDM increasingly adaptable to clinical practice.
Studies of shared decision making link increased patient involvement to improved treatment adherence, disease coping, and quality of life, whereas lack of patient involvement correlates with lower adherence to treatment, patient satisfaction, and health outcomes [6, 7]. The advantages of SDM are clear: maximizing the likelihood that both patient and physician will be respected, satisfied, and invested in the outcome.
These advantages may only prove successful under ideal circumstances [8, 9], however, and be less effective with patients who are in denial or lack health literacy and do not understand disease processes and treatment implications. Physicians may view requests from these patients as impractical, unjust, or even harmful from a professional point of view and may feel they are being asked to give inappropriate or futile care [10]. Finally, SDM is predicated on the presumption that an agreement will be reached between patient and physician, failing to account for the inevitable occurrence of unresolved disagreements [9]. Under such circumstances, SDM breaks down.
In contemporary medical ethics, when a shared decision cannot be reached, respect for patient autonomy is often considered the most important principle to follow, while paternalism has been relegated to a nearly historical perverse concept [11, 12]. Yet, the practice of physician-driven decision making is far more common than many physicians recognize or may care to admit. There are many situations, neither emergent nor life-threatening, in which physicians diagnose or treat patients without their knowledge or consent [8]. The subtleties of medical decision making are complex, and standards delineating a balance between patient autonomy and medical paternalism remain undefined. Efforts to generate decision-making parameters are often undermined by the unique nature of patient-specific values and preferences. This variability leaves physicians to interpret situation-dependent conditions without clear guidelines. To best describe the practice of situational decision making by physicians, we propose the concept selective paternalism.
Broadly defined, paternalism is an action performed with the intent of promoting another’s good but occurring against the other’s will or without the other’s consent [13]. In medicine, it refers to acts of authority by the physician in directing care and distribution of resources to patients. Medicine is a practice, not a mere formulary of facts; the expertise of the physician developed through years of education, apprenticeship, and experience cannot be fully imparted to the patient, hence, knowledge-based value judgments are essential to good medical care, and the physician must not be a passive participant [12, 14, 15]. This means that paternalism is inherent in the physician role and, thus, in the decision-making process.
Paternalism—choosing a course of action in the patient’s best interest but without the patient’s consent—serves as an integral value in ethical decision making, both as a balance to other values and as an ethical obligation to neither withhold guidance nor abdicate professional responsibility to patients [12, 16, 17].
Selective paternalism—the use of paternalism when, for any number of reasons, shared decision making breaks down—is commonplace in clinical practice in different degrees and various scenarios [3, 7, 8, 18], and must be recognized, discussed, and embraced as necessary for optimal patient care.
Paternalism does not serve as an endpoint or solution but as one of many integral values in the decision-making process. Just as the primary value of a moral rule is to alert us to the presence of a moral problem, thereby opening the door to potential resolution or alternatives to the dilemma, so selective paternalism should effectively promote awareness, productive dialogue, and prevention of error in decision-making situations [16].
Although respect for patient autonomy is imperative and there are benefits to pursuing shared decision making, there are scenarios in which SDM is impractical or even impossible. Medical decisions are often emotion-laden and induce distress, confusion, and conflict among patients and families, which can impair their desire and ability to participate in decision making [6].
Consider an example in which a 60-year-old man removes his nasogastric tube, telemetry leads, pulse oximeter, and supplemental oxygen at 2:00 AM immediately following abdominal surgery. The intern is called and sees the patient at the bedside. The patient requests that the Foley catheter and intravenous line be taken out; he is uncomfortable and does not want to be in the hospital any longer. Nurses have attempted to calm the patient for several hours, but he has become more agitated because his requests are not being followed. When examined by the intern, the patient is alert, oriented, and judged to have decision-making capacity. He (1) understands the treatment goals, (2) appreciates the significance of his decisions, (3) displays reasoning for his decisions, and (4) appropriately expresses choices that fall within his system of values [19]. The nurses request chemical or mechanical restraints for the patient.
Or suppose that a 20-year-old woman suffers devastating central neurological injuries from a motor vehicle accident and is left ventilator-dependent with poor chances of recovery. Her care team advises that tracheostomy and percutaneous gastrostomy be performed or that life support be withdrawn. Her mother, the lone surrogate decision maker, is unable and ultimately unwilling to decide on a plan of care; she does not consent to aggressive intervention or withdrawal of care. Multiple family meetings are unproductive at identifying a plan of care.
Physicians should respond to such situations with a more paternalistic approach, bearing the professional responsibility to act in the patient’s best interest and justly appropriate medical resources [20]. Ideally, patient autonomy is respected, not invoked as an excuse for abdication of professional responsibility or justification of unjust, futile use of resources [21, 22].
There are critical implications to the loss of physician-driven decision making in medicine. In many fields (e.g., law, education, economics), it is generally accepted that decisions are best made by experts. Within their respective fields, experts are charged with understanding the nuances required for best practice of the profession. Physicians are obligated to ensure quality and value in health care through education, expertise, and ethical practice patterns. Despite the common political opinion, medicine is not a simple consumer-producer market, and physicians cannot be forced into a fully patient-autonomous system. Furthermore, a default overemphasis on autonomy hinders the upholding of other central values in medical ethics: respect for autonomy must be balanced with nonmaleficence, beneficence, justice, and the paternalistic obligation to uphold standards of care [14]. Utilizing paternalism selectively in decision making is not only necessary but obligatory [16, 17].
Defining specific limits of physician or patient authority that would be applicable to all situations is an impossible task, but, since selective paternalism is commonplace and essential in clinical practice, a model of the process is both pragmatic and necessary. We have created a framework that identifies necessary elements of ethical decision making, based on that of Mulley and Sepucha, most recently revised in 2009 [6].
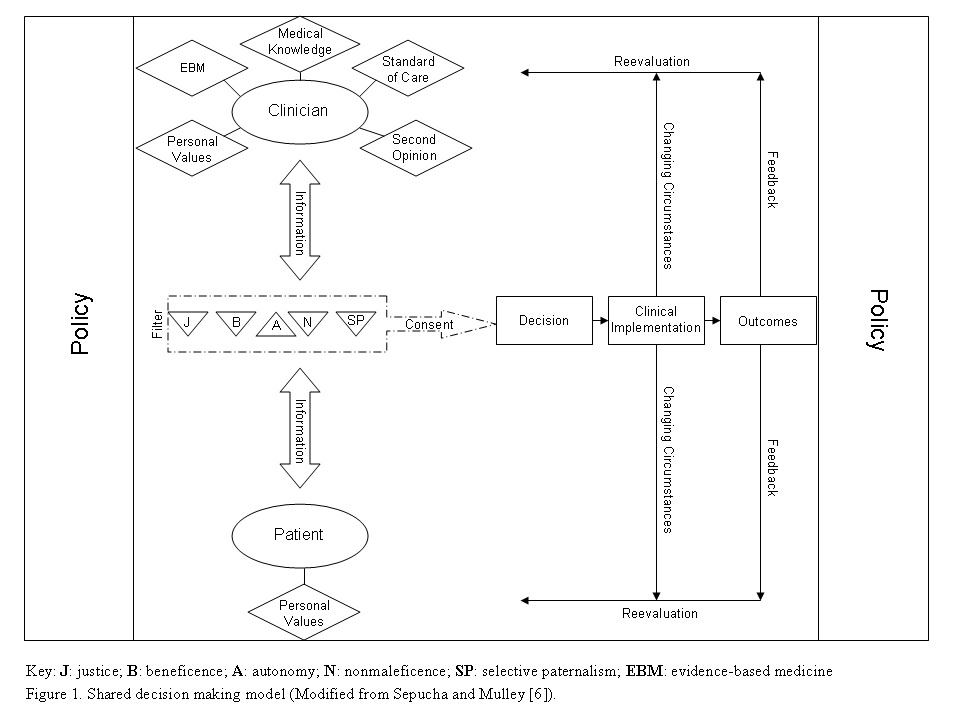
Figure 1. Shared decision making model.
Cllick image for larger view.
The original model underemphasized how one arrives at a decision, and, while it identifies the necessary participants, separates them from the decision. Our SDM framework focuses on how the decision process occurs by identifying elements that each participant represents and how those elements should be applied using a set of mandatory ethical value “filters” in order to reach consent [18]. This, in turn, can lead to the formation of a shared decision.
Policy creates the system in which clinicians and patients interact. Each participant, physician and patient, necessarily has an active role in shared decision making, introducing a variety of elements into the system, information that is used to determine consent and decision. Information flow between physician and patient with direct implications for decision making should be guided by applying values that promote ethical decision making and prevent imbalance among the values that could lead to abuse. A successful flow of information produces informed consent, from which a decision is made and subsequently enacted in clinical practice, with outcomes to follow that, in turn, render feedback to the participants.
The values represented as “filters” should be applied in every decision-making scenario. Failure to apply these values in decision making leads to a failure of communication, arresting shared decision making, and decisions made without these values can have dire consequences.
As physicians, most of us pride ourselves on respecting patient autonomy and the involvement of patients in the decision-making process, but we overlook the frequent occurrences of selective paternalism and often fail to use it appropriately or consistently. Instead, as physicians we should be both cautious and conscientious about our paternalistic decision making. We should acknowledge how we make decisions, thoughtfully reconsider those that may allow for an SDM process, and, at all times, take responsibility for ensuring the highest standards of ethical practice are enacted and embrace those decisions that are in patients’ best interest.
Milunsky A, Annas GJ. Genetics and the Law—II. New York: Plenum Press; 1980.
President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. Buffalo, NY: W.S. Hein; 1998.
Sartorius RE. Paternalism. Minneapolis: University of Minnesota Press; 1983.
Gert B, Culver CM, Clouser KD. Bioethics: A Systematic Approach. 2nd ed. New York: Oxford University Press; 2006.



