Case and Commentary
May 2020
Shared decision making honors patient autonomy, particularly for preference-sensitive care decisions. Shared decision making can be challenging, however, when patients have impaired decision-making capacity. Here, after presenting an illustrative case example, this paper proposes a capacity-adjusted “sliding scale” approach to shared decision making.
Dr Q is an academic hepatologist meeting a new patient, Mr R, for newly diagnosed cirrhosis. The patient has clear signs of liver dysfunction and has already been admitted to the hospital previously for a gastrointestinal bleed related to esophageal varices. He also has chronic obstructive pulmonary disease, obesity, and poorly controlled type 2 diabetes mellitus.
Dr Q and her student, Ms G, interview and examine Mr R together. They learn that Mr R did not complete high school and lives on what he calls “the wrong side of the tracks.” He lives alone and drinks 4 beers daily. He thinks his brother might have had “liver problems,” too.
As the conversation unfolds, it becomes clear that Mr R does not know why he’s in clinic today. “My doc said it was something about my liver, but…” He shrugs.
Ms G and Dr Q teach Mr R about cirrhosis. They emphasize the importance of alcohol abstinence and start to explain that further workup is necessary—including, potentially, a liver biopsy. Their goal is to enter into shared decision making with Mr R about liver biopsy.
Mr R holds up his hand midway through their explanation and says, “I’m not a detail guy, Doc. I trust you. You tell me what to do, and I’ll do it.”
They talk more, and, ultimately, Dr Q asks, “Do you have any questions for me?” Mr R pauses for a second, starts to ask a question, and then tapers off.1 Finally, he says, “Whatever you say, Doc. I’m in your hands.”
In the hallway, after Mr R has left to reschedule a follow-up visit, Ms G asks, “Did he really understand what we were talking about?” “Great question!” says Dr Q. “I have no idea. How can we be patient centered if the patient can’t or won’t tell us what he wants?”1
Shared decision making, in contrast to the parentalism of yesteryear, achieves the foundational bioethical value of respect for patient autonomy.2 Shared decision making is also good medicine: it improves patient understanding of medical options, deepens patient trust, and alleviates decisional conflict.3,4,5 These proven benefits of shared decision making accrue even though—or perhaps because—shared decision making is strongly influenced by complex factors such as cultural context, personal experiences, and social relationships, including relationships with clinicians.6
Shared decision making also fulfills the ethical duty to allocate resources wisely. First and foremost, shared decision making ensures that we invest health care resources in agreed-upon rather than presumed patient needs. By leading to care decisions by patients that tend to be more conservative than the care physicians assume patients would want, shared decision making likely reduces total health care expenditures,7,8 although we predict the magnitude of savings will vary from decision to decision.
Decision-making capacity is not binary. It can be whole, partial, or absent, and vary from decision to decision as well as from time to time.
Like most patients, physicians generally support shared decision making as long as patient decisions do not preclude the provision of high-quality care.9,10,11 However, many patient and clinician factors decrease the likelihood that shared decision making will occur.12 Prominent among these factors is impaired patient decision-making capacity. This impairment, and how to navigate it, is the focus of this article.
Shared decision making requires that the patient have some degree of decision-making capacity. Decision-making capacity entails patients’ ability to understand their decision, appreciate the consequences of each alternative, and communicate their wishes and rationale.13 The high prevalence of reduced decision-making capacity in some settings can thus make shared decision making a challenge. For example, although fewer than 3% of elderly patients in the general population lack decision-making capacity, a 2011 study found that decision-making capacity was impaired in 26% of hospitalized adults, 44% of nursing home residents, and 54% of patients with Alzheimer’s dementia.14
A common misconception is that patients who have impaired decision-making capacity cannot be expected to engage in shared decision making. Yet decision-making capacity is far from a binary phenomenon: it can be whole, partial, or absent; and decision-making capacity varies from decision to decision as well as from time to time.15 A mildly cognitively impaired patient might be capable of deciding that she wants surgery after failed medical therapy for knee osteoarthritis but be unable to weigh complex decisions regarding the various surgical options available. Alternatively, a fragile elderly patient receiving opioid treatments for pain might be perfectly capable of shared decision making in the morning but be cognitively impaired later in the day after his pain medications have taken effect.
Given situational and temporal variation in patient decision-making capacity and misconceptions of impaired decision-making capacity, clinicians may be tempted to deny patients the opportunity to engage in shared decision making. Nevertheless, clinicians should assess capacity in a decision-specific manner while tailoring their approach to shared decision-making to patient decision-making capacity. We call this tailored approach capacity-adjusted sliding-scale shared decision making (see Figure).
Figure. Capacity-Adjusted Sliding-Scale Shared Decision Making
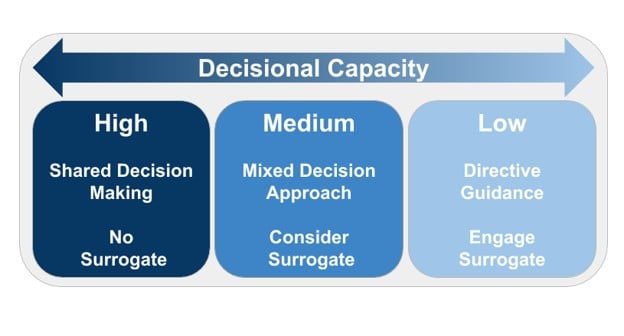
Capacity-adjusted sliding-scale shared decision making combines the assessment of patient decision-making capacity and the tailoring of shared decision making to patient capacity. This intermingling of processes is organic; the elicitation of patient preferences often yields information about patient decision-making capacity, while capacity assessments frequently yield information about patient preferences.
There are 5 steps in the capacity-adjusted sliding-scale shared decision-making approach:
The Figure depicts 3 levels of shared decision making that depend on degree of impairment, but, of course, there are innumerable degrees of impairment in patient decision-making capacity.
The engagement of surrogate decision makers can also be tailored to patient decision-making capacity. We invite clinicians to engage surrogates at all decision points, of course, but as highlighted in the Figure, surrogate decision maker engagement becomes progressively more indispensable as patient decision-making capacity wanes. When patients can make simple decisions (for instance, whether they want surgery for a given malady) but cannot engage nuanced decisions (ie, they cannot choose between competing surgical options), then a surrogate decision maker can provide more nuanced input that builds on the patient’s preferences. For patients who lack decision-making capacity entirely, a surrogate decision maker decides on their behalf. There are infinite gradations of patient decision-making capacity and thus infinite ways surrogate decision makers can tailor their support of patients’ goals of care.
Although surrogate decision makers are the best option when patients are unable to make decisions independently, they are not perfect. One systematic review found that surrogate decision makers represent patient preferences accurately only 68% of the time.17 Hopefully, the increasing utilization of living wills and decision support tools will improve surrogate decision maker accuracy.
Beyond supporting optimal accuracy of surrogate decision making, clinicians must take into account surrogates’ preferences regarding how they represent patient wishes. Archetypal surrogate roles in decision making have been defined, including preference advocates (who focus on patient values) and clinical facilitators (who focus on clinical information).18 These archetypes correspond loosely to the needs of patients with more or less decision-making capacity and thus to sliding-scale shared decision making. When there is mild impairment of patient decision-making capacity, surrogate decision makers often act as a preference advocate, whereas surrogates become more of a clinical facilitator as patient decision-making capacity wanes.
Directive clinician (or surrogate) decision support for patients with impaired decision-making capacity is parental.2 A common misconception is that parental decision support conflicts with the patient-centered nature of shared decision making. In fact, shared decision making can be understood and enacted through many patient-physician models, including parentalism, and is best understood as allowing clinicians flexibility to tailor their approach to patient capacity and preferences.19 Some patients might feel their preferences have been ignored or sidelined by a clinician taking a parental approach, while others might feel they’ve had inadequate guidance if a clinician is insufficiently directive. If the clinician takes the approach preferred by the patient and most appropriate to the patient’s decision-making capacity, then arguably patient autonomy is more respected than if the clinician were to hew dogmatically to a patient-driven approach contrary to the patient’s wishes or capacity.20 The unavoidably subjective determination of patient decision-making capacity and preferred decision-making style is, of course, susceptible to clinician bias,21 but fear of this bias should not dissuade clinicians from attempting to the best of their ability to tailor their shared decision-making approach to patient needs and preferences.
During sliding-scale shared decision making, clinicians might encounter patients who are reluctant to engage in shared decision making.22 Some patients might be unfamiliar with shared decision making, feel they have insufficient expertise to give an opinion, or be unaccustomed to having their preferences elicited by clinicians. With further education and coaching, they might well engage productively. Other patients will articulate a more steadfast preference for a directive clinician style. Much as aligning the approach to shared decision making to patient decision-making capacity honors patient autonomy, so too does tailoring the decision-making process to patient decision-making preferences.
Returning to the case, it is unclear whether Mr R lacks decision-making capacity or if he simply prefers a more directive clinician style. We would devote a conversation to the formal assessment of his decision-making capacity at the same time that we attempt to elicit his decision-making preferences. This approach would ensure that next steps in the liver biopsy decision both align care to Mr R’s preferences and respect his autonomy.
Broadening shared decision making to include patients with impaired decisional capacity would expand the uses—and potentially the benefits—of shared decision making. Coupled with other logistical means of aligning the method of decision making to patient preferences, such as decision aids and patient-reported outcome measures,23 capacity-adjusted sliding-scale shared decision making is well aligned to the preeminent goal of providing the highest quality care in a fashion that fits patient preferences and ameliorates the high cost of health care delivery today.24
Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4:CD001431.
Walsh T, Barr PJ, Thompson R, Ozanne E, O’Neill C, Elwyn G. Undetermined impact of patient decision support interventions on healthcare costs and savings: systematic review. BMJ. 2014;348:g188.
Murray E, Pollack L, White M, Lo B. Clinical decision-making: physicians’ preferences and experiences. BMC Fam Pract. 2007;8:10.
Sessums LL, Zembrzuska H, Jackson JL. Does this patient have medical decision-making capacity? JAMA. 2011;306(4):420-427.
Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891.
Lilley EJ, Morris MA, Luxford JMH, et al. Taking over somebody’s life: experiences of surrogate decision-makers in the surgical intensive care unit. J Am Coll Surg. 2016;223(4)(suppl 1):S48.
Kopelman LM. On distinguishing justifiable from unjustifiable paternalism. Virtual Mentor. 2004;6(2).
Légaré F, Adekpedjou R, Stacey D, et al. Interventions for increasing the use of shared decision making by healthcare professionals. Cochrane Database Syst Rev. 2018;7:CD006732.
Elwyn G, Frosch DL, Kobrin S. Implementing shared decision-making: consider all the consequences. Implement Sci. 2016;11:114.



