History of Medicine
Jul 2023
Peer-Reviewed
Body mass index (BMI) was introduced in the 19th century as a measure of weight relative to height. Before the late 20th century, overweight and obesity were not considered a population-wide health risk, but the advent of new weight loss drugs in the 1990s accelerated the medicalization of BMI. A BMI category labeled obesity was adopted in 1997 by a World Health Organization consultation and subsequently by the US government. Language in the National Coverage Determinations Manual stating that “obesity itself cannot be considered an illness” was removed in 2004, allowing reimbursement for weight loss treatments. In 2013, the American Medical Association declared obesity to be a disease. Yet the focus on BMI categories and on weight loss has yielded few health benefits and contributes to weight-related discrimination and other potential harms.
Dramatic statements about the health risks of obesity are common today. The opening lines of a recent article read: “Obesity is the most prevalent chronic disease worldwide, affecting approximately 650 million adults. Excess adiposity and its numerous complications, including cardiovascular disease and type 2 diabetes, impose a considerable economic burden and constitute major contributors to global morbidity and mortality.”1 Such assertions are a recent development. According to the Institute of Medicine, “Prior to the late 20th century, overweight and obesity were not considered a population wide health risk.”2 Body weight was often considered as more of a cosmetic and social issue than an important medical concern.3 A 1969 study found that patients and physicians did not view body weight and weight loss as salient medical problems and considered deviations from weight standards to be almost meaningless.4 Prior to 2004, the National Coverage Determinations Manual stated bluntly that “obesity itself cannot be considered an illness,”5 and treatment for obesity was not covered by Medicare.5 The costs of weight loss as a treatment for obesity were not allowed as a medical deduction for tax purposes until 2002.6 Until the 2010s, in most doctor visits, BMI was not calculated.7
In the early 1990s, obesity was not well defined in terms of either BMI or percentage body fat. A comprehensive World Health Organization (WHO) report in 1995 authored by an expert panel deliberately avoided using BMI to define obesity.8 The report explicitly defined grades of “overweight” using BMI cut points of 25, 30, and 40 but described these cut points as largely arbitrary. The panel noted: “There is no agreement about cut-off points for the percentage of body fat that constitutes obesity” and concluded that “there are no clearly established cut-off points for fat mass or fat percentage that can be translated into cut-offs for BMI.”8 Obesity became more medicalized as new weight loss drugs, such as orlistat and dexfenfluramine, began to be developed9 and the limited medical concern for obesity to be seen by the pharmaceutical industry as a barrier to wider acceptance of the use of weight loss medications.10 This article argues that the ensuing focus on BMI categories and on weight loss have created a narrative that is advantageous to the billion-dollar weight loss industry but has yielded little in the way of long-term health benefits and can exacerbate weight-related discrimination and stigmatization.
In 1995, the International Obesity Task Force (IOTF) was created, led by Philip James, who was at the time the director of the Rowett Research Institute in Aberdeen, United Kingdom (later merged with the University of Aberdeen and called the Rowett Institute). This self-appointed task force was set up as a charity and funded almost entirely by contributions from the pharmaceutical industry.11,12 In 2013, a reporter asked James where the funding for the IOTF came from, and James replied: “‘Oh, that’s very important. The people who funded the IOTF were drugs companies.’ And how much was he paid? ‘They used to give me cheques for about 200,000 [British pounds] a time. And I think I had a million or more.’”12
At its inception, the IOTF had as its explicit purpose to convince the WHO to hold a special consultation solely devoted to obesity.13 The WHO was initially reluctant. 13 Such a consultation was not part of the WHO planning process and hadn’t been agreed to by its executive board.13 The IOTF provided a substantial grant to the WHO to fund the consultation, which took place in 1997, and IOTF staff authored the draft report for the consultation, which was adopted with almost no changes.13
Because of a production backlog, the final report was delayed and not published officially until 2000.14 The WHO took the unusual step of disseminating an interim publication of the original agreed-upon version of the consultation report in 1998, paid for by the IOTF.15 According to James: “On discovering that the full WHO report on obesity would take a long time to edit and translate into the six WHO languages, we, in the IOTF, decided to publish the original agreed-upon version of the consultation ourselves and send it immediately to all 200+ ministers of health.”16 The interim publication was for limited distribution only and not issued to the general public,15 but nonetheless had a broad impact.
An expert panel was convened in 1995 by the National Heart, Lung, and Blood Institute (NHLBI) and tasked with developing clinical practice guidelines for treatment of overweight and obesity.17 The chair and 3 other members of the NHLBI panel were members of the IOTF. The interim publication from the 1997 WHO consultation was available to the NHLBI panel and enabled the NHLBI panel members to cite it in their clinical guidelines, which were published in 1998.17 The NHLBI committee adopted almost the same BMI categories as the 1997 WHO consultation report, and these BMI categories are the ones most often used today.
As shown in Table 1, the nomenclature for BMI categories in the 1997 WHO consultation14 and in the 1998 NHLBI guidelines17 differed from the terminology in the WHO’s earlier 1995 report.8
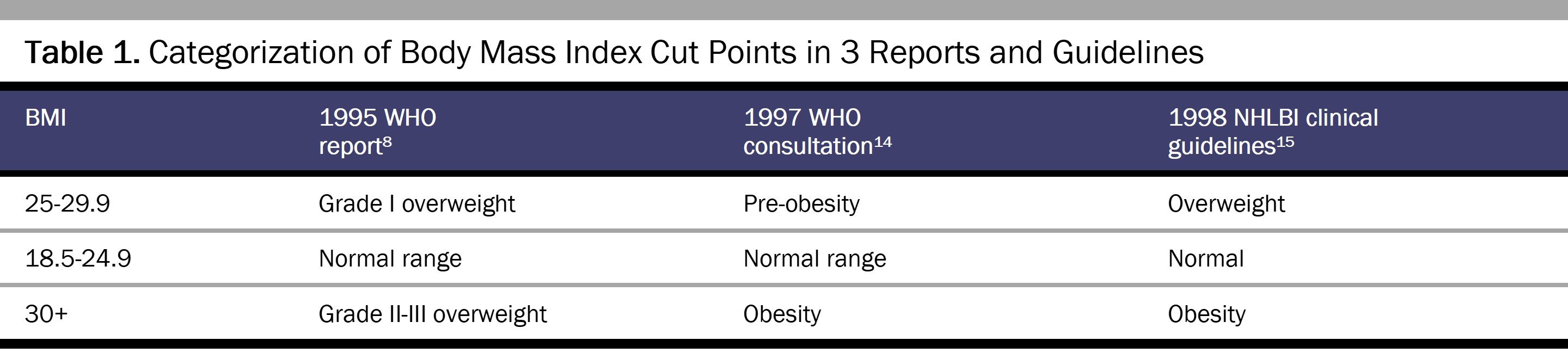
The 1997 WHO consultation used the same arbitrary BMI cut points as the 1995 report, but without discussion changed the terminology for a BMI of 30 or above from “overweight” to “obesity” (see Table 1). Despite this obvious difference, the 1997 WHO consultation report claimed that its classification was “in agreement” with the 1995 WHO report and asserted that a BMI of 30 or more was already widely accepted as denoting obesity.15 The NHLBI panel then adopted the same terminology for a BMI of 30 or more. The New York Times noted the new term obesity for a BMI of 30 or above and described the resulting categories as creating “a booming new market for diet pills for the obese, practically served to the companies on a silver platter by the Government.”18
The change in terminology from overweight to obese was medically and socially significant. When the American Medical Association decided in 2013 to classify obesity as a disease,19 it made no distinction between obesity defined as excess fat harmful to health and obesity defined as a BMI of 30 or above. There is no clearly accepted level of body fat, however, that would represent a diagnosis of obesity.20 Scientific organizations routinely explain that the degree of body fat that is (or may be) harmful varies by age, sex, fat distribution, and multiple other factors.21,22 In the absence of any clear definition of obesity in terms of body fat, a BMI of 30 or above is used as a cut point, but no justification has been provided for that number. The definition of “normal” weight as a BMI of 18.5 to 24.9 is also problematic and has no obvious justification.23 In almost all Organisation for Economic Co-operation and Development countries, over half the population is, on this definition, above normal weight24 and thus in some way abnormal, pathological, or deviant.25 Such classifications invite stereotypes.26
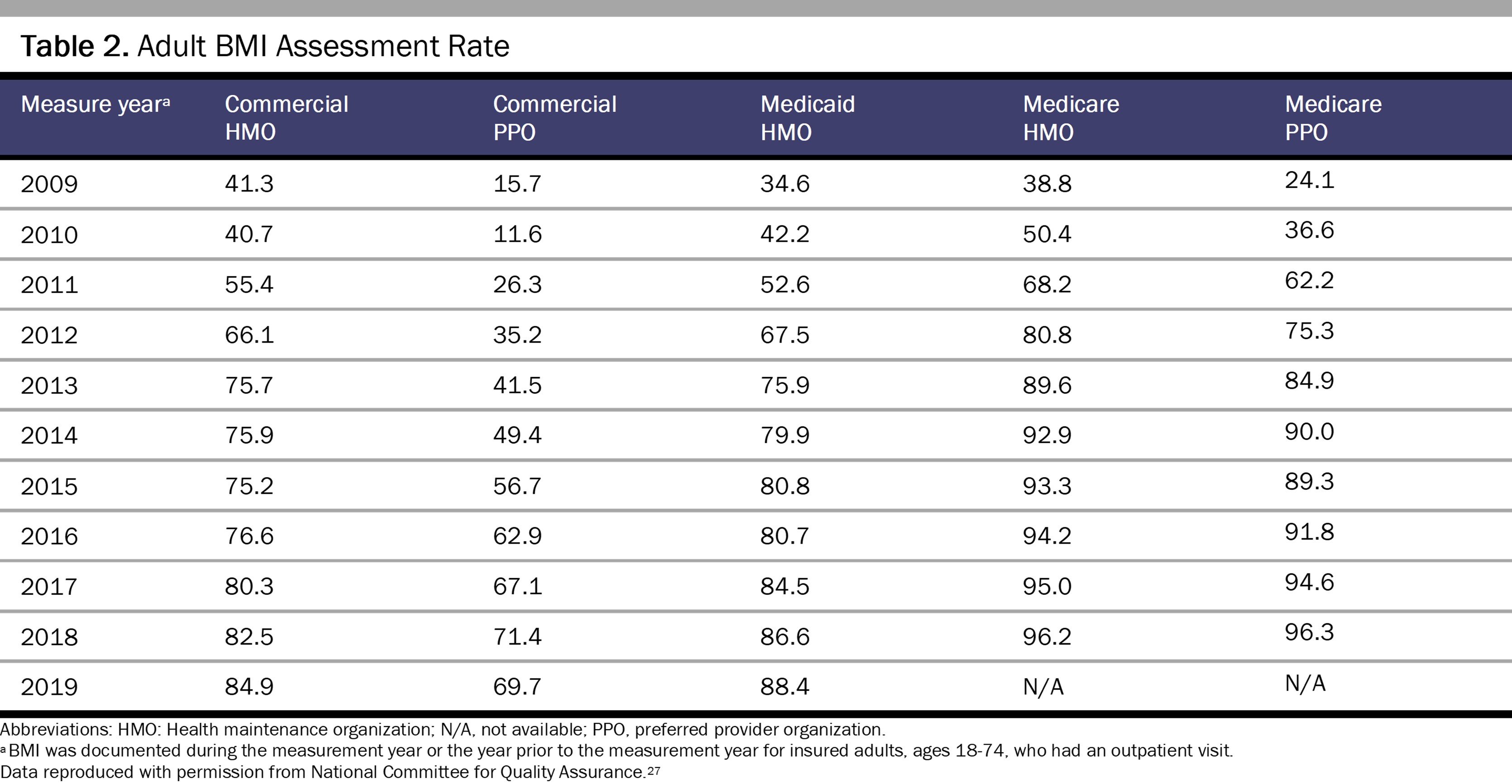
As shown in Table 2, there has been a steady increase in BMI assessment in clinical settings, with it being included in over 96% of Medicare visits in 2018.27 As will be discussed, there is little evidence that this procedure has yielded benefits for patients or improved long-term health outcomes of morbidity or mortality.
US Preventive Services Task Force (USPSTF) recommendations regarding obesity in adults started in 1996 with a recommendation that clinicians periodically measure all patients’ weight and height.28 The USPSTF recommendations then progressed through several iterations to the recommendation in 2018 that clinicians provide access to intensive, multicomponent behavioral interventions for all adults with a BMI of 30 or above.29,30 The USPSTF thus took a weight-centered approach, not a health-centered approach, in its recommendations.31 A thread running through all the USPSTF recommendations is the lack of evidence that weight loss will improve morbidity and mortality. The 1996 version stated: “Evidence is limited that screening for obesity and implementing weight-reducing or weight maintenance strategies are effective in decreasing long-term morbidity and mortality.”28 According to the 2012 version, “Inadequate evidence was found about the effectiveness of these interventions on long-term health outcomes (for example, mortality, cardiovascular disease, and hospitalizations).”32 The 2018 version29,30 referenced 2 major studies33,34 showing that participants with prediabetes had a lower risk of developing diabetes after weight loss interventions but stated there was no evidence of other benefits. Long-term follow-ups of the 2 cited studies showed no impact of the interventions on cardiovascular morbidity or mortality.35,36,37 Women’s Preventive Services Initiative 2022 recommendations for counseling interventions to prevent weight gain among midlife women also noted the absence of direct evidence that these interventions improve mortality or morbidity.38,39
A 1997 workshop convened by the National Institutes of Health called for a randomized controlled trial of an intensive lifestyle intervention for intentional weight loss—including behavior modification, diet, and exercise—to provide needed guidance on the risks and benefits of weight loss that could inform rational clinical and public health policy.40 That trial, known as Look AHEAD, found that an intensive lifestyle intervention focusing on weight loss did produce weight loss and reduce waist circumference but did not reduce the rate of cardiovascular events in adults with type 2 diabetes and overweight or obesity.41 The trial was discontinued after a maximum of 13.5 years of follow-up on the basis of a futility analysis.41 A follow-up study found that the lifestyle intervention also did not significantly reduce mortality risk.42 Two other trials, one involving patients with arthritis and one involving patients with hypertension, found similar results.43,44
As these studies demonstrate, recommendations for universal screening and lifestyle interventions generate an intense focus on BMI categories and weight loss without adequate evidence of long-term improvement in morbidity or mortality. Moreover, they ignore several potential sources of harm. A 1998 New England Journal of Medicine editorial cautioned: “Until we have better data about the risks of being overweight and the benefits and risks of trying to lose weight, we should remember that the cure for obesity may be worse than the condition.”45 The focus on BMI also ignores the possible adverse health effects caused by weight bias in health care leading to health care avoidance.46 More generally, the emphasis on weight loss contributes to discrimination and the harms of weight stigma.47,48 Potential harms may also arise from weight loss medications or from adverse events following bariatric surgery. Several weight loss medications approved by the US Food and Drug Administration have been subsequently withdrawn for causing unexpected harmful side effects.49,50,51,52 A weight-inclusive approach has been called for to minimize the harms of weight loss promotion.53 In the United Kingdom, members of Parliament recently called on the government to stop using BMI as a measure of health.54
International standardization of BMI categories, largely motivated by the introduction of weight loss drugs and funded by the pharmaceutical industry, has resulted in the creation and overuse of arbitrary BMI categories that don’t identify the same level of health risks across individuals or populations. These categories have been used to arrive at misleading population estimates of overweight and obesity that are in effect prevalence estimates of a clinically diagnosed disease based solely on height and weight. People are thus classified as having a disease without ever having been diagnosed by a clinician or been seen by a medical professional.
BMI is not a good measure of fat mass, and fat mass itself may not be a good indicator of health.55 Some studies have found that low muscle mass is more of a health risk than high fat mass.56,57,58 Bosy-Westphal and Müller suggest that obesity should not even be considered a question of body fat per se but should be addressed in terms of body composition and that the use of both BMI and body fat percentage in assessing obesity-related health risk should be avoided.59 They call for a new approach focused on fat-free mass instead and point out that, at older ages, a higher BMI may indicate more adequate fat-free mass. Another new paradigm has been suggested according to which overweight and moderate obesity are beneficial for patients with a broad spectrum of chronic diseases.60 Physical activity and fitness may be more important for health than adiposity is.61,62,63 It is time to look beyond the arbitrary and questionable BMI categories and evaluate other approaches to promote health and well-being.
Glickman D, Parker L, Sim LJ, Del Valle Cook H, Miller EH, eds; Institute of Medicine. Accelerating Progress in Obesity Prevention: Solving the Weight of the Nation. National Academies Press; 2012.
Flegal KM. How body size became a disease: a history of the body mass index and its rise to clinical importance. In: Gard M, Powell D, Tenorio J, eds. Routledge Handbook of Critical Obesity Studies. Routledge; 2022:23-39.
Centers for Medicare and Medicaid Services. Treatment of obesity. US Department of Health and Human Services. October 1, 2004. Accessed February 28, 2023. https://www.hhs.gov/guidance/document/treatment-obesity-1
Graham J. Height, weight—BMI? Doctors urged to treat body mass index as a vital sign. Washington Post. May 12, 2012. Accessed October 10, 2022. https://www.washingtonpost.com/national/health-science/height-weight--bmi-doctors-urged-to-treat-body-mass-index-as-a-vital-sign/2012/05/12/gIQAbFbJLU_story.html
Physical status: the use and interpretation of anthropometry. Report of a WHO expert committee. World Health Organ Tech Rep Ser. 1995;854:1-452.
Quest for blockbuster anti-obesity drug vexes firms. Daily Record. August 28, 2000. Accessed October 10, 2022. https://thedailyrecord.com/2000/08/28/quest-for-blockbuster-antiobesity-drug-vexes-scientists/
Moynihan R. Obesity task force linked to WHO takes “millions” from drug firms. BMJ. 2006;332(7555):1412.
Peretti J. Fat profits: how the food industry cashed in on obesity. The Guardian. August 7, 2013. Accessed October 10, 2022. https://www.theguardian.com/lifeandstyle/2013/aug/07/fat-profits-food-industry-obesity
Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i-xii, 1-253.
World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation on Obesity, Geneva, 3-5 June 1997. World Health Organization; 1998. Accessed February 10, 2023. https://apps.who.int/iris/bitstream/handle/10665/63854/WHO_NUT_NCD_98.1_%28p1-158%29.pdf?sequence=1&isAllowed=y
James WPT. A dissenter’s journey. Annu Rev Nutr. 2021;41:1-18.
Expert Panel on the Identification, Evaluation, and Treatment of Overweight in Adults. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: executive summary. Am J Clin Nutr. 1998;68(4):899-917.
Stolberg SG. Ideas and trends: the fat get fatter; overweight was bad enough. New York Times. May 2, 1999. Accessed October 10, 2022. https://www.nytimes.com/1999/05/02/weekinreview/ideas-trends-the-fat-get-fatter-overweight-was-bad-enough.html
Healy M, Gorman A. AMA declares obesity a disease. Los Angeles Times. June 18, 2013. Accessed May 19, 2023. https://www.latimes.com/science/la-xpm-2013-jun-18-la-sci-obesity-disease-20130619-story.html#:~:text=The%20American%20Medical%20Assn.,a%20medical%20condition%20requiring%20treatment
Sommer I, Teufer B, Szelag M, et al. The performance of anthropometric tools to determine obesity: a systematic review and meta-analysis. Sci Rep. 2020;10(1):12699.
Overweight or obese population (indicator). OECD (Organisation for Economic Cooperation and Development) iLibrary. Accessed March 24, 2023. https://www.oecd-ilibrary.org/social-issues-migration-health/overweight-or-obese-population/indicator/english_86583552-en
Cryle P, Stephens E. Normality, A Critical Genealogy. University of Chicago Press; 2017.
Hacking I. Kinds of people: moving targets. Proc Br Acad. 2007;151:285-318.
Adult BMI assessment (ABA). NCQA (National Committee for Quality Assurance). Accessed February 28, 2023. https://www.ncqa.org/hedis/measures/adult-bmi-assessment
Final recommendation statement. Obesity: screening, 1996. US Preventive Services Task Force. January 1, 1996. Accessed September 2, 2022. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/obesity-screening-1996#citation8
Uusitupa M, Peltonen M, Lindström J, et al. Ten-year mortality and cardiovascular morbidity in the Finnish Diabetes Prevention Study—secondary analysis of the randomized trial. PLoS One. 2009;4(5):e5656.
Wing RR, Bolin P, Brancoti FL, et al; Look AHEAD Research Group. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369(2):145-154.
Alberga AS, Edache IY, Forhan M, Russell-Mayhew S. Weight bias and health care utilization: a scoping review. Prim Health Care Res Dev. 2019;20:e116.
Puhl RM. Weight stigma, policy initiatives, and harnessing social media to elevate activism. Body Image. 2022;40:131-137.
Fenfluramine and dexfenfluramine withdrawn from market. Am J Health Syst Pharm. 1997;54(20):2269-2270.
Czernichow S, Batty GD. Withdrawal of sibutramine for weight loss: where does this leave clinicians? Obes Facts. 2010;3(3):155-156.
Mahase E. Weight loss pill praised as “holy grail” is withdrawn from US market over cancer link. BMJ. 2020;368:m705.
Mahase E. Stop using body mass index as measure of health, say MPs. BMJ. 2021;373:n941.
Bosy-Westphal A, Muller MJ. Diagnosis of obesity based on body composition-associated health risks—time for a change in paradigm. Obes Rev. 2021;22(suppl 2):e13190.



