State of the Art and Science
Oct 2024

Sleep is essential for a healthy, productive life, but access to sufficient and quality sleep is not universal. Sleep equity is influenced by both pathological and nonpathological sources. This article considers nonpathological determinants of adequate sleep, defines 3 features of sleep insecurity, and suggests how to promote sleep literacy to remove some barriers to adequate sleep, promote sleep equity, and improve individual and community health and well-being.
Air, food, and water are essential for human survival, and access to each is considered a fundamental human right. No less essential for survival is sleep, and insufficient or poor-quality sleep—like insufficient or poor-quality air, food, or water—is associated with severe health consequences.1,2,3,4,5,6 Therefore, sleep, too, has been considered a fundamental human right.7,8 However, public health efforts to ensure sufficient quality of air, food, and water and thereby avoid serious health problems have traditionally dwarfed attention to adequate sleep. Moreover, adequate sleep is not universally accessible, as many people endure circumstances beyond their control that create substantive sleep inequities and disparities.9 As a result, adverse health and social consequences ensue, often without the realization of those affected.10 Public health policies and legislation have scarcely kept pace with the rapidly expanding but still young science of sleep and biological rhythms. The passage of California’s law regarding later school start times for high school students is a notable exception.11
The first half of this manuscript will describe the concepts of sleep insecurity and sleep deserts, terms that help to illuminate inadequate sleep as a social justice issue. Although many sleep determinants may seem familiar, they are seldom discussed in the context of inequity, taken to mean absence of justice or fairness. The second half of this manuscript will propose key public health policies that could improve sleep equity and secure better health, quality of life, and well-being in a tangible manner and for sizeable segments of the population.
The right to adequate sleep—sufficient in amount and quality—is often put at risk by multiple barriers that can be transient or persistent.12 The concept of sleep insecurity refers to the “limited or uncertain availability of adequate sleep,” whether short-term or long-term.13 A related concept, sleep deserts, refers to environments that “are not conducive to adequate sleep health.”14 Whereas sleep insecurity may be transitory, sleep deserts inflict chronic, poor sleep on their residents. Whether barriers to adequate sleep health are mild and transient or rampant and persistent, they often have an uneven distribution and intensity across communities, environments, and societal circumstances.
Sleep deserts. Sleep deserts exist in socioeconomically disadvantaged neighborhoods—for example, where busy transportation routes too frequently cause noise and air pollution that prevent good-quality sleep.15 Beyond neighborhoods, sleep deserts can extend into a college dormitory where students on completely different sleep schedules engage in late-night activities that prohibit sound sleep.16 Communities plagued by war, crime, or other threats of violence do not offer safety during an unconscious state of sleep and can also create sleep deserts.17,18 Global warming has raised fears that some regions are becoming too hot to support human life, with the result that high nighttime temperatures—without air conditioning, which remains out of reach for many—threaten sleep quality that depends on reasonably cool surroundings.19
Sleep insecurity. In contrast to persistent exposure to sleep deserts, many situational realities beyond the sleep environment can contribute to sleep insecurity. At a school where pressures to succeed cause excessive anxiety, students can experience sleep insecurity. Work environments—in medicine, the military, and factories, for example—can require such excessive working hours that sleep insecurity can emerge.20,21 Intermittent shift work repeated weekly creates sleep insecurity, as no human circadian rhythm can adapt effectively to many wake-sleep schedule changes every few days.22 Even if workplace requirements do not technically preclude adequate sleep or alignment with the circadian rhythm, work-related stress and anxiety can still foster sleep insecurity. All these situations, beyond the impact of physical environments, have similar potential to create inequities in sleep health.
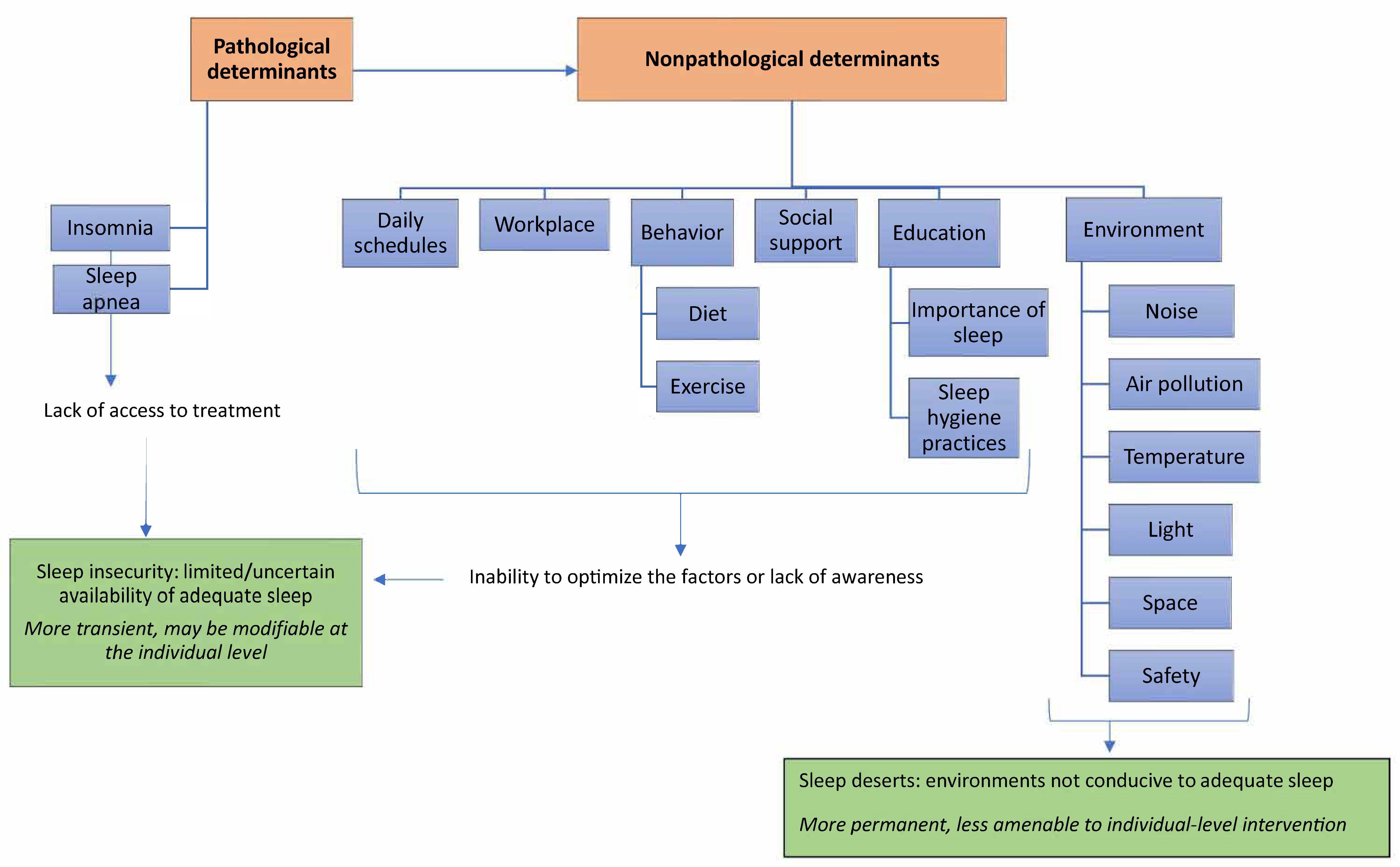
Human behaviors can also give rise to sleep insecurity. Alcohol consumption at night, caffeine consumption later in the day, adoption of a highly variable sleep schedule, or heavy meals near bedtime23 are all detrimental to good sleep quality. A summary of the determinants of sleep insecurity and sleep deserts is illustrated in the Figure.
Figure. Determinants of Sleep Insecurity and Sleep Deserts
Prevalence of sleep disorders. Large proportions of the population suffer from undiagnosed sleep disorders and often have symptoms for decades.24 Insomnia symptoms affect about 30% to 40% of the population at any one time, and specific insomnia disorders have a prevalence of 5% to 10% in adults.25 Obstructive sleep apnea affects more than half of individuals with diabetes, and symptoms of restless legs syndrome affect up to 15% of adults.26,27 Few individuals emerge from childhood without having had sleep problems. Yet, in many cases, no medical assistance is sought, and only ineffective medical assistance is provided. Despite the pervasiveness of sleep problems, sleep medicine occupies only a few hours in a typical 4-year medical school curriculum; most medical textbooks devote scant numbers of pages to sleep disorders; and the ratio of board-certified sleep medicine physicians to people even in the United States, where they are more common than in many other countries, is 1:43 000.28,29,30,31
Inequities in sleep insecurity and sleep deserts are multifaceted and cannot be easily addressed by any single set of public health policies. However, many inequities do share at least 1 of 2 key underpinnings. The first is limited personal financial resources, which can be insufficient for an individual to live in a quiet neighborhood, ensure a secure sleep environment, avoid the necessity for shift work, access a healthy diet, or see a physician familiar with sleep disorders. The imperative to ameliorate poverty and socioeconomic challenges has long motivated compelling arguments to do so by many experts other than sleep health specialists, and yet the solution is not likely to be found easily or soon.
The second fundamental underpinning of inequities in sleep health, however, is lack of critical, relevant education about sleep health. Importantly, the solution—sleep health literacy—may be achievable much more readily than resolution of socioeconomic disparities. Sleep health literacy is a first, key step to improving sleep for people who suffer from sleep insecurity and who live in sleep deserts. Importantly, education efforts must focus not only on individuals and health care professionals but also on school administrators and policy makers who can alleviate some of the barriers to adequate sleep.
Individual-level measures. At the individual level, education for children, their parents, and other adults about the importance of a simple concept—sufficient sleep, of good quality, on a regular basis—is astoundingly nearly completely absent from the curricula and agenda of schools, public health efforts, health literacy programs, relief agencies, health insurance companies, and government-run health programs in the United States and globally. Whereas nutrition and exercise programs are nearly universal experiences in schools, starting at early ages, teaching about the importance of healthy sleep is often excluded. Of note, the increasing focus on sleep health content in mass media and social media in recent years is welcome but does not represent an organized educational effort of the magnitude necessary to make a positive impact on sleep insecurity and sleep deserts. Moreover, media content should emphasize the need for 7 to 9 hours in bed nightly for most adults and considerably more for children and teens.32 Little time is spent on the importance of quiet, dark, comfortably cool, and physically and mentally secure sleep environments. In fact, many young people assume that sleep time is infinitely compressible, like a sponge, and that it can accommodate any exigencies that demand more time spent awake. Many individuals are not aware that lost sleep usually cannot be made up entirely or that chronic sleep deprivation can have serious, even life-shortening, consequences.33 Many do not appreciate the enormous risk to productivity, social interactions, quality of life, and well-being of sleep disturbances.
Awareness of sleep health and the basics of sleep medicine is also necessary for all clinicians who routinely provide wellness and sick visits,28 as sleep disturbances are often unreported and undiagnosed but carry significant implications for overall health.33 During routine visits, screening for poor sleep hygiene could help identify patients who may be at risk for poor sleep health.
Societal-level measures. Beyond individual-level education, widespread implementation of government- and institution-supported lifelong education about the importance of healthy sleep and feasible steps to achieve it would reduce sleep inequities even in sleep deserts. The aim of this sleep health literacy campaign should be to change a culture that devalues sleep and, moreover, celebrates the implied dedication, motivation, or strength of those who defy natural sleep needs through use of caffeine, force of will, or other means. These programs should be available in all communities across all socioeconomic levels. However, their implementation in underserved communities that endure inequities in wealth, safety, education, and health may have the highest impact and may merit prioritization. The earliest beginnings of such programs already exist. Sweet Dreamzzz® for Early Childhood, now part of the Pajama Program,34 is a nonprofit organization established in the early 2000s in Detroit by a nurse, Kathleen Donnelly, who found children sleeping in the hallways outside their classroom in an inner-city elementary school. In the years since its establishment, the organization has delivered a half-day of sleep education to more than 70 000 children and their families and distributed sleep essentials.35 A preschool curriculum for teachers with daily reinforcing teacher-administered lessons for 2 weeks after the day of intervention was found to have lasting impact in one study of Head Start programs in Michigan,36 but not in other Head Start programs in New York State.37 This effort, though, developed and administered mainly by volunteers with only limited philanthropic, foundation, or National Institutes of Health funding, is an example of what could and should grow into a nationwide mandate at all public schools.
Despite strong advocacy and persuasive data, school start times in middle and high schools across much of the United States are still before 8:30 am. Parents, teachers, and school administrators often oppose changes likely to benefit the sleep of many students, as well as their academic and athletic performance, with negligible impact on after-school activities.38 In 2019, California became the first state to pass a law requiring all high schools and middle schools to start after 8:30 am and 8 am, respectively, which provides a model for other states to follow.11 Education campaigns that reach stakeholders should be part of public health efforts to improve the overall health, well-being, and academic performance of sleep-deprived teens and provide them with sleep security.
At the institutional level, inclusion of sleep health information in medical school curricula and continuing medical education activities to highlight symptoms, risk factors, and consequences of poor sleep has the potential to help ameliorate sleep insecurity and sleep deserts. Cost-effectiveness research and dissemination of its results could also help to convince health plan administrators that sleep health literacy, screening programs, health promotion programs, and sleep medicine services are win-win opportunities. Indeed, cost-effectiveness research has shown that diagnosis and treatment of obstructive sleep apnea likely saves insurers considerable downstream health care expenditures.39,40 Similarly, the enormous economic burden of insomnia, the most common sleep disorder among adults, would be significantly reduced with treatment, according to several studies.41 Financial benefits to society, insurers, and individuals thus would be likely if sleep disturbances and disorders were reduced.
At the corporate level, education of employers about individual chronotypes and losses in productivity of sleep-deprived staff could lead to policies that improve sleep health for employees and, at the same time, enhance on-job effectiveness, well-being, and profits.
Effective education programs would be a first step toward major policy changes that could take years to be envisioned, formulated, and realized before sleep deserts are largely eliminated. Conceivable examples, however, include solutions that would address some of the more obvious disruptors of sleep from a public health perspective. For example, sleep health education for policy makers could lead to incentives for sleep security-enhancing features in new low-income housing, including safety features, noise abatement, and temperature control, which should be part of housing codes to the same extent that safe water and sewage are required. Sleep health-savvy policy makers could also conceivably reduce noise in neighborhoods along train tracks by enforcement of the maximum volume level for locomotive horns (96 decibels),42 by modified train schedules between 12 am and 5 am, and by incentives for residents of sleep deserts to implement effective soundproofing.
As public health advocates, we believe that education—sleep health literacy—should be a key initial priority in any long-term public health strategy to address sleep insecurity, sleep deserts, and inequity in sleep health.43 For local, state, and national government structures, education of staff at all levels with responsibility for schooling and public health would ensure well-informed choices and policy making. At the corporate and institutional level, education of employers could promote higher productivity, improved mood, and profits. At the individual level, people who suffer from sleep inequities rarely realize that this is a fundamental problem. A baseline level of sleep health literacy would enable people to be better self-advocates, to realize that healthy sleep is a key part of healthy wakefulness, and to make best use of any available resources to counter a substantial list of threats to their personal sleep security.
Wang S, Li Z, Wang X, et al. Associations between sleep duration and cardiovascular diseases: a meta-review and meta-analysis of observational and Mendelian randomization studies. Front Cardiovasc Med. 2022;9:930000.
Windred DP, Burns AC, Lane JM, et al. Sleep regularity is a stronger predictor of mortality risk than sleep duration: a prospective cohort study. Sleep. 2024;47(1):zsad253.
Yin J, Jin X, Shan Z, et al. Relationship of sleep duration with all-cause mortality and cardiovascular events: a systematic review and dose-response meta-analysis of prospective cohort studies. J Am Heart Assoc. 2017;6(9):e005947.
Liu RT, Steele SJ, Hamilton JL, et al. Sleep and suicide: a systematic review and meta-analysis of longitudinal studies. Clin Psychol Rev. 2020;81:101895.
Lim DC, Najafi A, Afifi L, et al; World Sleep Society Global Sleep Health Taskforce. The need to promote sleep health in public health agendas across the globe. Lancet Public Health. 2023;8(10):e820-e826.
Chattu VK, Manzar MD, Kumary S, Burman D, Spence DW, Pandi-Perumal SR. The global problem of insufficient sleep and its serious public health implications. Healthcare (Basel). 2019;7(1):1.
Dunietz GL, Braley TJ, Jansen EC. Sleep insecurity as a health disparity. J Clin Sleep Med. 2022;18(10):2521.
Sahloul MZ, Sankari AG. Sleep disorders in Syria. In: Attarian HP, Coussa-Koniski MLM, Sabri AM, eds. The Practice of Sleep Medicine Around the World: Challenges, Knowledge Gaps and Unique Needs. Bentham Science Publishers; 2023:203-228.
Buguet A, Reis J, Radomski MW. Sleep and global warming: how will we sleep when the Earth is hotter? J Neurol Sci. 2023;454:120859.
Cornejo C. How does sleep apnea affect diabetes? Healthline. June 8, 2022. Accessed May 29, 2024. https://www.healthline.com/health/diabetes/sleep-apnea-and-diabetes#:~:text=In%20the%20general%20population%2C%20an,diabetes%20experiencing%20obstructive%20sleep%20apnea
Collen JF, Wickwire EM, Capaldi V, Lettieri C. Losing sleep! Are we missing the future of sleep medicine? J Clin Sleep Med. 2020;16(4):473-474.
Almohaya A, Qrmli A, Almagal N, et al. Sleep medicine education and knowledge among medical students in selected Saudi medical schools. BMC Med Educ. 2013;13(1):133.
Watson NF, Rosen IM, Chervin RD; Board of Directors of the American Academy of Sleep Medicine. The past is prologue: the future of sleep medicine. J Clin Sleep Med. 2017;13(1):127-135.
How much sleep is enough? National Heart, Lung, and Blood Institute. Updated March 24, 2022. Accessed July 1, 2024. https://www.nhlbi.nih.gov/health/sleep/how-much-sleep
Colten HR, Altevogt BM, eds; Institute of Medicine. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. National Academies Press; 2006:chap 3.
Sweet Dreamzzz® for Early ChildhoodSM. Pajama Program. Accessed May 29, 2024. https://pajamaprogram.org/sweet-dreamzzz-for-early-childhood%E2%84%A0/
Bedtime just got better! Pajama Program. November 12, 2020. Accessed May 29, 2024. https://pajamaprogram.org/bedtime-just-got-better/
Bonuck K, Collins-Anderson A, Schechter CB, Felt BT, Chervin RD. Effects of a sleep health education program for children and parents on child sleep duration and difficulties: a stepped-wedge cluster randomized clinical trial. JAMA Netw Open. 2022;5(7):e2223692.
Dunietz GL, Matos-Moreno A, Singer DC, Davis MM, O’Brien LM, Chervin RD. Later school start times: what informs parent support or opposition? J Clin Sleep Med. 2017;13(7):889-897.
Wickwire EM, Shaya FT, Scharf SM. Health economics of insomnia treatments: the return on investment for a good night’s sleep. Sleep Med Rev. 2016;30:72-82.



