Medicine and Society
Jul 2022
Peer-Reviewed
This article considers ethical questions raised during development of an online art exhibit for and with people with dementia and their care partners. This article also describes a participant engagement process emphasizing patient autonomy as a means of dismantling stigma, promoting personhood, and stimulating community engagement. This co-creative project suggests the potential for patients’ art to spark attitude change and promote reciprocal, regenerative care practices.
By 2030, Alzheimer’s Disease International estimates that 74.7 million people will be living with dementia worldwide.1 The illness is a major and increasing cause of disability associated with impairment and deterioration of memory and other mental abilities, communication and behavior disruptions, and decreased capacity for everyday activities.1 With no known cure and limited efficacy of pharmacological treatments in ameliorating cognitive decline,2,3 dementia significantly influences individuals’, families’, and communities’ health and well-being. There is mounting interest in forms of psychosocial care, including arts-based interventions, which aim to facilitate “living well” with the dementia.4,5 Moreover, there is now recognition that perspectives of people living with dementia should be included in effective care intervention development.6
Historically, this population has been omitted from conversations about care and from research owing to assumptions that they are unreliable narrators of their own stories.7 Despite ethical and methodological challenges, the benefits of involving people with dementia in research far outweigh such challenges.8,9,10,11 Participatory research, particularly qualitative and arts-based approaches, has demonstrated the efficacy of first-person perspectives in promoting agency and autonomy through aligning research methods with persons’ capabilities and experiences,10,11 which can help temper participants’ feelings of shame, anxiety, and fear of being open about their condition. For the wider public, hearing the voices of those with lived experience of dementia can call into question false assumptions about what the diagnosis means and diminish stigma related to a fear of the unknown.
The commitment to more inclusive research practice is enhanced by a relational ethic of care that foregrounds real-life relationships between self and others. As such, the source of ethical commitments is located in everyday interactions, in affirming the particular over the universal and attending to the immediacy of the situation.12 This orientation demands that researchers be reflective about their motivations and engage with participants’ stories in authentic ways, honoring the complexity and ambiguities of human life. In the context of research with (vs research on) people with dementia and their informal carers, relational care ethics is especially important in making space for narrative agency,13 social citizenship,14 and a strengths-based, person-centered approach to research ethics.15 Relational understandings of persons’ agency, their human right to fully participate in society, and their capabilities, values, and preferences obligate researchers to adopt practices that support these elements of human flourishing throughout the research process.
In this article, we draw upon relational care ethics to illuminate the ethical commitments inherent in 3 issues that arose during the development of a virtual art exhibition co-created with people with dementia and their carers. The exhibit was the final phase of a 3-phase qualitative, arts-based research project focusing on the meaning of living well with dementia at the end of life. We conclude with our thoughts on how the exhibition co-creation process embodied “taking and making care.”
The research proceeded in 3 phases. Phase 1 included 35 in-depth interviews with people with dementia and their carers. Of these, a total of 24 people (see Table) participated in phase 2, which included 4 in-person and 4 online artmaking workshops focused on what participants wanted others to know about living well with dementia. The autonomy of each participant in creating the art depended upon their individual capacity, although we were careful not to make presumptions about capacity. Indeed, both people with dementia and their carers held varying levels of comfort in creating art, and it was up to them to let us know if and when they wanted assistance. Follow-up interviews encouraged participants to jointly and individually reflect on the creative experience, what inspired or surprised them, what was most challenging, and what provided hope.
| Characteristic | Persons Living With Dementia (n = 12) |
Carers (n = 12) |
|---|---|---|
| Female, No. (%) | 4 (33) | 10 (83) |
| Age, range (mean), y | 70-89 (75.4) | 41-76 (67.7) |
| Caucasian, No. (%) | 9 (75) | 10 (83) |
| High school education, No. (%) | 7 (58) | 10 (83) |
| Living alone, No. (%) | 2 (17) | 1a (8) |
|
a Carer’s relative with dementia moved into a tertiary care center at the time of the workshop.
|
||
In phase 3 (developing the online exhibition), 58 artworks were selected by participants from the works they created in the artmaking workshops. It is this process of co-creation we focus on here. Originally intended as an in-person installation, the exhibit shifted to a virtual format in response to the COVID-19 pandemic.16 The exhibit was co-created over a 6-month period by study participants and the research team. It features painting, collage, poetry, sculpture, photography, and a short documentary, each piece accompanied by a brief artist’s statement articulating salient aspects of the work.
From the beginning, it was important to center participant voices in the conversation about living well and to find ways to engage the wider community with the work in a positive way. In addition to soliciting individual participant feedback on the exhibit before its official launch, we held 3 group discussions with participants to collectively consider the exhibition’s overall aesthetic, navigability, and accessibility and coordinated an online survey. We also asked participants how well these elements communicated key outcomes related to living well and caring well at the end of life. Our engagement process focused on 3 issues whose ethical connotations emerged through relational understandings of these issues.
Co-creating the art exhibit required careful attention to decision-making processes to actively support participants’ agency and personhood and to promote community engagement while still maintaining our commitment to respectful representation. While these 3 issues are interrelated, we discuss each in turn.
Promoting power and agency. Dementia researchers have a long history of exerting power by limiting options and information and not ensuring that circumstances uphold the moral agency of participants.17,18 In contrast, relational understandings of autonomy encourage examination of inherent power dynamics and the tacit ways that the agency of people with dementia and their carers’ is supported or undermined.
In order to represent participants’ artwork and stories in an honest and respectful way and to prompt dialogue about what it means to live well with dementia, the layout of the art exhibition had to be simple, self-explanatory, and accessible. It was vital to meaningfully engage participants in decision making about the exhibition’s design yet not to overwhelm them with continual requests for feedback or design questions that lacked context. Thus, we created a prototype based on website design principles developed for and by people with dementia19,20 to give participants an idea of how the exhibit could look. We then provided opportunities for participants to share their opinions both individually and collectively. This iterative process allowed people to weigh in on the aesthetic aspects and navigability of the exhibit, as well as on how they were represented as individuals and as a group. The most common feedback was to increase the number of visual reminders about which webpage was open and to include clear instructions for where to click to move elsewhere on the site, access more information, or return to the homepage. In seeing their feedback incorporated in the exhibit design, several participants remarked that they “felt heard” (participants 2 and 4) and that their ideas “actually meant something” (participant 3). We took care to consult participants with dementia and their carers as equal agents by making space for them to voice concerns, opinions, and ideas to the extent they felt comfortable without putting anyone on the spot. Our understanding of participants’ needs and concerns was central to ensuring that participants felt at ease showcasing their work. This was one of the major takeaways: living well with dementia means having a seat at the table.
Another relational aspect of power and autonomy is that people with dementia and their carers must have the ability to determine if and when they will reveal their own (or their partner’s) diagnosis. Bearing in mind that labels can reify power imbalances, polarize relationships, and contribute to unfounded conclusions about the capacity of those with lived experience, we collectively decided to refrain from explicitly identifying each artist as either a person with dementia or a carer and instead made space for participants to self-identify if they chose. As shown in Figure 1, participant preferences regarding identification were sometimes explicit in the artwork and artist’s statement.
Figure 1. The Caregiver’s Mask, by Marilyn
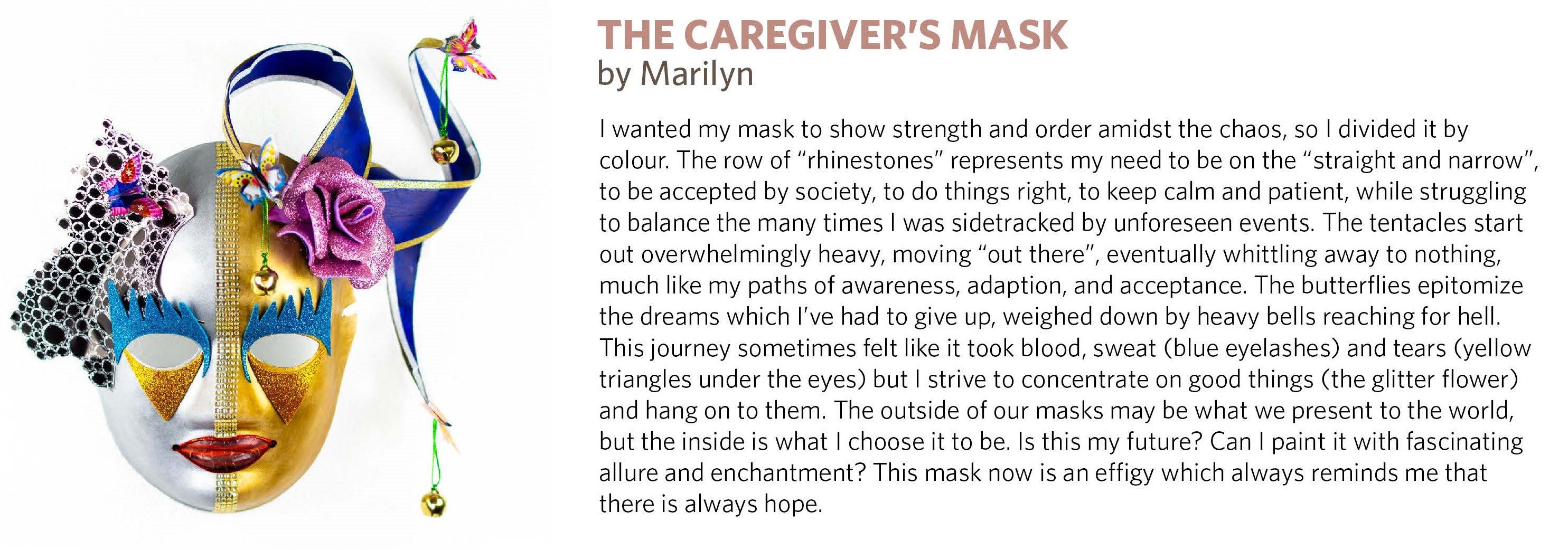
Courtesy of the participant.
Our collaborative work with participants was an enriching learning process that had a profound effect on the exhibition design, which further highlights the importance of co-construction—that is, centering the exhibit on the vision and priorities of people with lived experience. Maintaining an ethical commitment to attend closely to relationships in the myriad ways these can be expressed (eg, between care recipients and care givers, participants and their artwork, research team and participants, and caring and being cared for) reinforced our awareness of the overlapping nature of and intimate connections between these relationships. Moreover, the active engagement of participants illustrated how people might live well or even thrive with dementia. This emphasis on agency and voice and its importance as a social determinant of health is, however, neglected when the value of creative expression is reduced to a specific set of measurable health outcomes.21 Beyond promoting autonomy, creativity plays a larger role in promoting the personhood of both persons with dementia and their carers.
Personhood. Smith et al assert that “an individuals’ expressive capacity, or voice, is both an interactive link to others and a type of identity authentication. Without it, individuals lose their ability to participate in their environment and assert their autonomy.”22 That art making is an especially powerful vehicle for promoting self-expression and social participation in people with dementia is well documented.23,24,25 In developing the exhibition, as a team, we reflected on how best to honor the voices of persons with dementia and their carers through co-creation of the exhibition design and careful curation of the artworks. Participants were also directly engaged in editing artist statements for 2 reasons. First, researchers’ words and images could unintentionally portray persons with dementia in stereotyped or stigmatizing ways.26 Second, presuming persons’ incapacity to participate in decision making can quickly lead to deterioration of their standing and dignity.14,27
Working from a place of relational ethics enabled us to critically reflect on our own roles in “caring for” participants while promoting their personhood through actions such as not making assumptions about their preferences, supporting creative risk taking (eg, encouraging participants to use a new art form), being in the moment, and adapting the process to facilitate participation. However, what was at the forefront of our minds was striking a balance between hearing directly from people with dementia about their perspectives and hearing about their experiences through the voice of a carer. We accommodated this tension by coming at questions from several angles and engaging in an iterative process that ensured we listened to multiple perspectives and provided everyone with a chance to speak as authentically possible.
To support the ability of participants to exercise some control over the interpretation of their artworks, all were invited to write, or contribute to, a reflective statement about their creative work. However, many were hesitant to write the statement themselves, deferring to the research team for assistance. To foster a space of trust and to honor the priorities and values of each participant, it was essential to amplify participants’ voices rather than speak for them. Thus, in writing these statements, we employed multiple checks and balances. We wrote in the first person and used the participants’ own words available verbatim to us through interview transcripts and audio files. Listening to their voices and intonations and how they expressed themselves painted a picture of their personalities, values, and priorities. The words in each artist statement were arranged to reflect these unique voices and ideas.
Personhood was also reflected in the artwork itself. Each piece had a character and distinctive voice expressed through colors and shapes. Some were vibrant pieces in bright yellow and red (see Figure 2), and others were more quiet and subtle, using wood veneer in shades of brown (see Figure 3). Each piece and medium captured something unique about how the artist felt at that specific moment—and how they wanted to express it.
Figure 2: Sailboat, by Myrna
Courtesy of the participant.
Figure 3 Untitled, by Jack

Courtesy of the participant.
Stimulating community engagement. With the shift from an in-person to an online exhibition, new avenues for community engagement emerged, enabling the project to reach a larger, more international audience. While exciting, this development also increased the importance of thinking carefully about intended and unintended audience impacts and their ethical implications.28 Who might visit the exhibit and under what conditions? Was it likely someone with dementia or their carer would see aspects of themselves in the artwork and stories? Could the issues examined in the exhibit be triggering or seen as stigmatizing? What kinds of background information or design features would help ensure that viewers could both appreciate how the work was generated and have a safe and stimulating space in which to respond?
We developed 3 activities to encourage visitors to interact with the participants and one another. Once engaged, they could upload and share their own artwork, ask questions of the artists or comment on the art, or participate in writing a collaborative story. The goal was to provide a platform to connect people with similar experiences.
Since its launch in October 2020, the exhibition has attracted more than 2800 visitors from 38 different countries. This much-wider-than-anticipated reach allowed us to tap into a broader community perspective. To help us understand the exhibition’s impact, a viewer survey was available directly from the website. As illustrated in Figure 4, a word cloud depicting the most commonly identified words used to describe the exhibit, responses to the exhibition from individual viewers were overwhelmingly positive.
Figure 4. Word Cloud, by Susan Cox
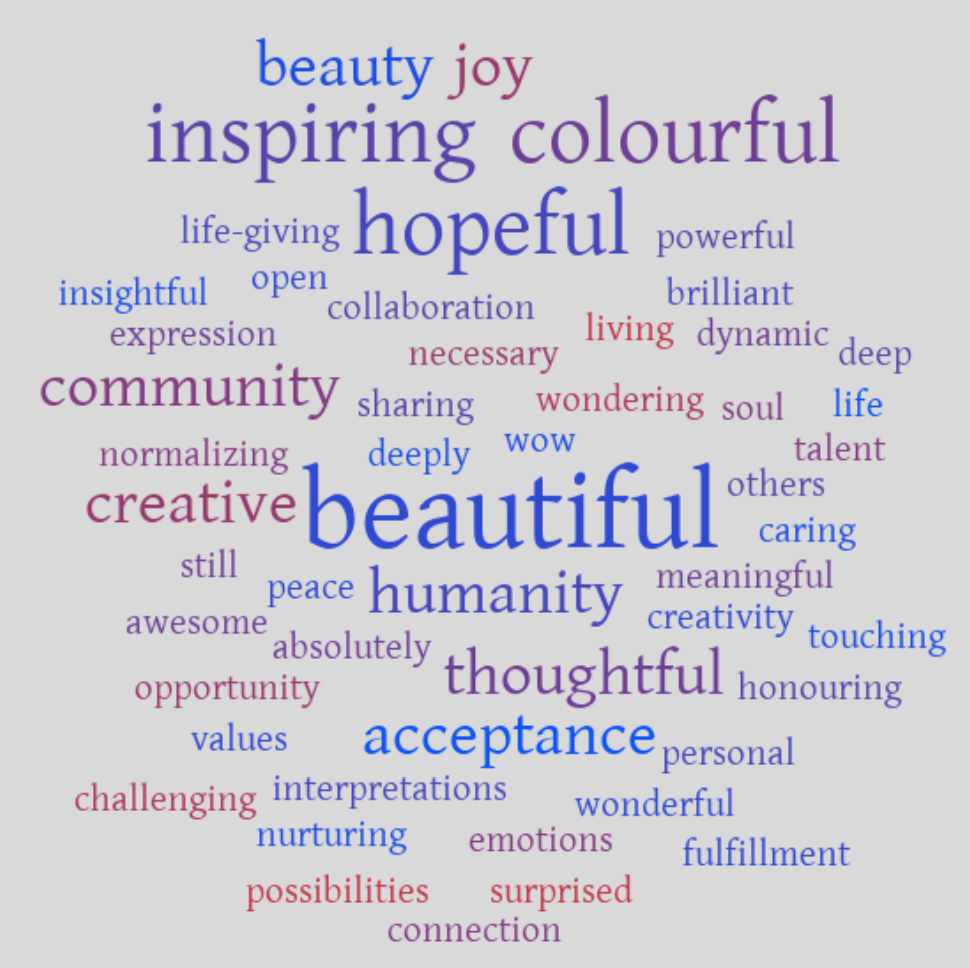
Courtesy of the author.
Feedback on survey questions about possibilities for living well with dementia and how the viewer might subsequently respond to people with dementia attest to how the exhibition could also prompt change in viewers’ attitudes. As one respondent noted, they now see people living with dementia “not as patients but as people first.” Another respondent noted that the exhibit opens one “up to possibilities and the choice to not start with self-defeating assumptions based on what has been presented by others…. Quality of life is what you make of it as you proceed around, through, and over the potholes on the path.”
In other, unexpected ways the exhibit enhanced the quality of life for some participants. One person living with dementia and their carer were featured in a high school documentary that was later shared with their spiritual community. Both participants were initially reluctant to share the diagnosis, given their concern about ongoing acceptance within their community. However, sharing the exhibition and being featured in a documentary led to them not only feeling heard but also being valued in ways they had never imagined at the outset. Other participants were invited to speak about their role in the exhibition on a popular radio program and at other community events; these activities showcased the power of arts-based research to convey and promote best practices in community engagement.
The participant engagement processes used for both generating the artwork and procuring ongoing consent for the use of art, images, and story were strengths based and person centered. As an added measure to ethically safeguard and care well for all participants and relationships, we chose to foreground the art and artist statements that most reflected participants’ relationships to the art itself, rather than delving into personal biographies. As a manifestation of an ethic of care, centering the artist statements on the art enabled us to emphasize the stories participants most wanted to share. It also framed an important space for critical reflection on our own practices of research and participant engagement, encouraging us to sit with questions of what it means to “be cared for” and to “care for well.”
These 3 elements—power and autonomy, personhood, and community engagement—highlight the importance of situating ethics in the context of everyday interactions by attending closely to developing practices that support and sustain research as an act of both taking care and making care. This is a reciprocal co-creative process that asks nothing more and nothing less of us than to listen deeply and to respond with care.
Prince M, Wimo A, Guerchet M, Ali GC, Wu YT, Prina M. World Alzheimer Report 2015. The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. Alzheimer's Disease International; 2015. Accessed January 25, 2018. https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf
Morgan J. Living well with dementia. Lancet Neurol. 2017;16:587-588.
Clare L, Wu YT, Jones IR, et al; IDEAL Study Team. A comprehensive model of factors associated with subjective perceptions of “living well” with dementia: findings from the IDEAL study. Alzheimer Dis Assoc Disord. 2019;33(1):36-41.
Bergum V, Dossetor J. Relational Ethics: The Full Meaning of Respect. University Publishing Group; 2005.
Baldwin C. Narrative and decision-making. In: O’Connor D, Purves B, eds. Decision-Making, Personhood and Dementia: Exploring the Interface. Jessica Kingsley; 2009:25-36.
Bartlett R, O’Conner D. Broadening the Dementia Debate: Towards Social Citizenship. Policy Press; 2010.
Puurveen G, Mann J, Cox SM. Beyond tokenism and unconscious bias: a strengths-based approach to dementia research. In: Weisstub DN, Zima T, eds. Medical Research Ethics: Challenges in the 21st Century. Springer Publishing. Forthcoming.
In There Out Here: Art Making Space to Live Well With Dementia virtual exhibition. Art Making Space. Accessed February 22, 2022. https://www.artmakingspace.com/
Alzheimer Society of British Columbia; Emily Carr University. Collaborate, Gather, Share: A Workbook Towards Dementia-Friendly Research. Alzheimer Society of British Columbia. Forthcoming.
Williams R. How to design a website for someone affected by dementia. Alzheimer's Society. May 18, 2017. Accessed July 02, 2020. https://www.alzheimers.org.uk/blog/how-design-website-someone-affected-dementia
Williams R. 5 things to consider when designing websites for older people. Alzheimer's Society. November 9, 2017. Accessed July 02, 2020. https://www.alzheimers.org.uk/blog/considerations-for-designing-websites-older-people
Smith NL, Kotthoff-Burrell E, Farber L. Protecting the patient's voice on the team. In: Mezey MD, Cassel CK, Bottrell MM, Hyer K, Howe JL, Fulmer TT, eds. Ethical Patient Care: A Casebook for Geriatric Health Care Teams. John Hopkins University Press; 2002:83-101.
Kitwood T. Dementia Reconsidered: The Person Comes First. Open University Press; 1997.


